Pathophysiology/Complications O R I G I N A L
A R T I C L E
ACE Inhibitors Improve Diabetic Nephropathy Through Suppression of Renal MCP-1 BERTHOLD AMANN, MD1 RALPH TINZMANN, MD2 BERNHARD ANGELKORT, MD2
OBJECTIVE — Chemokines play an important role in the pathogenesis of diabetic nephropathy. Angiotensin II induces several fibrogenic chemokines, namely monocyte chemoattractant protein-1 (MCP-1) and transforming growth factor-. The progression of diabetic nephropathy can be retarded by ACE inhibitors (ACEIs) in patients with type 1 and type 2 diabetes. We examined if blockade of the renin-angiotensin system lowered urinary levels of the chemokine MCP-1 and correlated urinary MCP-1 (uMCP-1) with parameters of renal function and glucose and lipid metabolism before and after 1 year of treatment with an ACE inhibitor. RESEARCH DESIGN AND METHODS — In 22 patients with type 2 diabetes and diabetic nephropathy in stages 3–5, treatment with the ACEI lisinopril was initiated. Before treatment and after 12 months of continuous therapy, proteinuria, creatinine clearance, uMCP-1 levels, BMI, HbA1c, and serum cholesterol were assessed. RESULTS — Lisinopril treatment improved renal function. Proteinuria decreased from 410 ⫾ 662 mg per 24 h to 270 ⫾ 389 mg per 24 h. Creatinine clearance rose from 61 ⫾ 26 to 77 ⫾ 41 ml/min. Urinary MCP-1 levels decreased from 0.456 ⫾ 0.22 ng/mg creatinine to 0.08 ⫾ 0.096 ng/mg creatinine. The change in uMCP-1 correlated significantly (r ⫽ 0.61, P ⬍ 0.001) with the change in proteinuria. No other parameter correlated with the improvement in renal function. CONCLUSIONS — Blockade of the renin-angiotensin system in type 2 diabetic patients with diabetic nephropathy reduces uMCP-1 levels and improves renal function. Because MCP-1 induces monocyte immigration and differentiation to macrophages, which augment extracellular matrix production and tubulointerstitial fibrosis, pharmacological reduction of angiotensin II may also exert its beneficial effects in diabetic nephropathy by downregulation of renal MCP-1. Diabetes Care 26:2421–2425, 2003
D
iabetic nephropathy due to type 2 diabetes is becoming the single most important reason for endstage renal disease in the western world (1). Besides glomerular damage and glomerulosclerosis, diabetic nephropathy is characterized by aseptic tubulitis and tubulointerstitial fibrosis (2). Macrophages and macrophage products play an impor-
tant pathogenic role in tubulointerstitial inflammatory and noninflammatory conditions and have been implicated as effector cells of tubulointerstitial damage in diabetic nephropathy (3,4). Increased numbers of glomerular and interstitial macrophages have been observed in rat models of experimental diabetes and in biopsies of patients with diabetic ne-
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
From the 1Kamillianer Hospital Mo¨nchengladbach, Mo¨nchengladbach, Germany; and the 2Diabetes Department, Medical Hospital North, Community Hospital Dortmund, Germany. Address correspondence and reprint requests to Dr. Berthold Amann, MD, Franziskus Hospital Berlin, Budapester Strasse 15-19, D 10715 Berlin, Germany. E-mail:
[email protected]. Received for publication 11 November 2002 and accepted in revised form 2 May 2003. Abbreviations: ACEI, ACE inhibitor; AT, angiotensin; MCP-1, monocyte chemoattractant protein-1; RAS, renin-angiotensin system; uMCP-1, urinary MCP-1. A table elsewhere in this issue shows conventional and Syste`me International (SI) units and conversion factors for many substances. © 2003 by the American Diabetes Association.
DIABETES CARE, VOLUME 26, NUMBER 8, AUGUST 2003
phropathy (5). Monocytes are attracted to the place of organ damage by monocytespecific chemokines. Monocytes follow an endothelial-bound gradient of chemokine molecules and transmigrate from the vascular bed into the tissue at the point of the highest chemokine concentration (6). Therefore, systemic levels of chemokines do not reflect their local generation. A meaningful determination of chemokine expression can only be done in the anatomical compartment where chemokines are produced or in the near vicinity thereof. In renal diseases, this is either the kidney itself or urine. Monocyte chemoattractant protein-1 (MCP-1) is the strongest known chemotactic factor for monocytes and is upregulated in many renal diseases (7), including diabetic nephropathy (8). Renal MCP-1 expression is induced by elevated glucose levels, tubular reabsorbed protein, and probably advanced glycosylated end products (9). In diabetes, the tissue reninangiotensin system (RAS) of the kidneys is activated. Studies in type 1 (10) and type 2 (11) diabetes showed that abrogation of angiotensin (AT)-II activity either with ACE inhibitors (ACEIs) or AT-II type 1a receptor antagonists slowed the loss of renal function more effectively than treatment with other antihypertensive drugs even in the absence of systemic hypertension. Additional evidence from experiments with specific AT-1a receptor antagonists showed that the nephroprotective effect of ACEIs is indeed due to inhibition of the RAS and not due to other ACE-mediated processes (12,13). Besides the systemic and renal hemodynamic effects of AT-II, it has been shown recently that AT-II directly induces the expression of MCP-1 in vascular smooth muscle cells (14). Furthermore, in experimental nephritis, AT-II activates the transcription factor nuclear factor-B and initiates MCP-1 synthesis in renal cells with subsequent interstitial recruitment of monocytes and interstitial fibrosis; this effect could be blocked by ACE inhibition (15). The main renal source of MCP-1 is the tubular epithelial 2421
Nephropathy and MCP-1
cells (16). Therefore, blockade of the RAS might reduce the renal production of MCP-1, and the resulting decrease in monocyte immigration and monocyte activity would subsequently ameliorate interstitial fibrosis and, consequently, stabilize or improve renal function. To test this hypothesis, we investigated the relationship between urinary MCP-1 (uMCP-1) and renal function in patients with type 2 diabetes and diabetic nephropathy. In the absence of urinary tract infection, uMCP-1 reflects the renal production of this chemokine. Therefore, we measured uMCP-1 before and after 1 year of treatment with the ACEI lisinopril. RESEARCH DESIGN AND METHODS Patients Twenty-two patients with type 2 diabetes and diabetic nephropathy in stages 3–5 according to the definition of Mogensen et al. (17) (microalbuminuria of ⱖ30 mg/l) who had not been previously treated with an ACEI or an AT-II receptor antagonist were included. All patients received either conventional or intensified insulin therapy; no oral antidiabetics drug were given. The characteristics of the patients at baseline are shown in Table 1. Patients with hypertension were included if blood pressure with previous antihypertensive medication was ⬍150/90 mmHg. Antihypertensive medication was continued unchanged, and lisinopril was given as an add-on medication. All patients were given lisinopril (Acerbon; Astra, Wesel, Germany) in a dose ranging from 5 mg to maximally 20 mg per day for 12 months once daily. The mean ⫾ SD daily dose was 9.2 ⫾ 2.1 mg lisinopril. Compliance was checked by telephone interviews with patients and general practitioners after 6 months. Patients were reexamined after 12 months. At entry and after 12 months of continuous administration of lisinopril, the following parameters were determined: serum creatinine, HbA1c, serum total cholesterol, C-reactive protein, 24-h microalbuminuria/proteinuria, 24-h creatinine clearance, and uMCP-1 levels. Urine and blood samples were taken when no clinical and laboratory signs of systemic infection were present. Urinary tract infection at the time of sampling was excluded by normal urine sediment. Urinary albumin was measured by nephelometry (Beck2422
Table 1—Characteristics of the patients at baseline Parameters
Data
Patients (n) Type 2 diabetes (n) Age in years (range) Sex ratio (male/female) Diabetes duration (years) BMI Nephropathy Stage III Stage IV Stage V Hypertension Antihypertensive treatment -Blocking agents Diuretics ␣-Blocking agents Central ␣-adrenergic agents Calcium channel blockers Diabetes complications Retinopathy Peripheral neuropathy Cardiovascular disease
22 22 62.4 ⫾ 10.9 (38–78) 13/9 10.2 ⫾ 8.7 30.1 ⫾ 4.2 11 5 6 19 19 15 10 5 7 9 14 17 15
Data are means ⫾ SD.
man Instruments, Fullerton, CA); normal values are ⬍20 mg per 24 h. Creatinine clearance and total creatinine excretion were measured in a 24-h urine collection. HbA 1 c was determined with highpressure liquid chromatography (Menarini HA 8140). Fasting total serum cholesterol levels were assayed by standard enzymatic methods. MCP-1 assay MCP-1 urine levels were measured with a solid-phase enzyme linked immunosorbent assay (Quantikine MCP-1 ELISA; R&D Systems, Minneapolis, MN). All assays were done in duplicate. The mean variation in the samples of one patient was ⬍5%. The minimum detectable MCP-1 level with this kit is 5 pg/ml. There is no cross-reactivity with the closely related chemokines MIP-1␣, MIP-1, and MCP-2, -3, and -4 . Statistical methods For statistical analysis, the SPSS software package (SPSS, Chicago, IL) was used. All results are given as means ⫾ SD. The Mann-Whitney test for paired samples was used. Correlations were calculated with the Pearson product moment correlation coefficient. P ⬍0.05 was considered statistically significant.
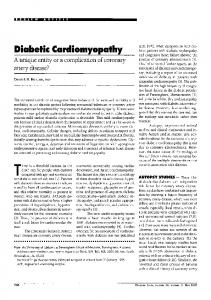
RESULTS Treatment effects After 1 year of treatment with lisinopril, there were no changes in the physical characteristics of the patients (Table 2). Urinary concentrations of MCP-1 at baseline correlated significantly with microalbuminuria/proteinuria. Under lisinopril treatment, drastically lowered MCP-1 concentrations in urine (P ⫽ 0.001, Fig. 1) were found. Creatinine clearance improved and microalbuminuria/proteinuria decreased (P ⬍ 0.002, Fig. 2). The reduction of uMCP-1 (⌬ uMCP-1) correlated highly significant (r ⫽ 0.61, P ⬍ 0.001) with the change in microalbuminuria/proteinuria (⌬ urinary protein, Fig. 3). Serum creatinine remained stable during treatment. Addition of lisinopril did not significantly lower blood pressure and had no effects on BMI. Neither serum total cholesterol levels nor glycated hemoglobin levels correlated with uMCP-1 or proteinuria. CONCLUSIONS — In this study, we describe a drastic reduction of urinary levels of the chemokine MCP-1 in patients with diabetic nephropathy who were treated with the ACEI lisinopril. Furthermore, the observed improvement DIABETES CARE, VOLUME 26, NUMBER 8, AUGUST 2003
Amann, Tinzmann, and Angelkort
Table 2—Results and correlations at baseline and after 1 year of lisinopril therapy
Parameters
Baseline 410 ⫾ 662 0.456 ⫾ 0.22 8.8 ⫾ 2.2 5.61 ⫾ 1.00 92.8 ⫾ 18.6 61 ⫾ 26 0.42 ⫾ 0.11 139 ⫾ 4 87 ⫾ 3 30.2 ⫾ 5.2 r ⫺0.04 (NS) 0.12 (NS) NA NA NA 0.19 (NS) 0.17 (NS) NA 0.29 (NS) ⫺0.1 (NS) NA 0.58 (P ⫽ 0.05) NA
Urinary protein (mg/d) uMCP-1 (ng/mg creatinine) HbA1c (%) Total cholesterol (mmol/l) Serum creatinine (mol/l) Creatinine clearance (ml 䡠 min⫺1 䡠 1.73 m⫺2) C-reactive protein (mg/dl) Mean systolic blood pressure (mmHg) Mean diastolic blood pressure (mmHg) BMI (kg/m2) Correlation coefficients (Pearson) HBA1c/urinary protein HbA1c/uMCP-1 Lisinopril dosage/uMCP-1 Lisinopril dosage/urinary protein Lisinopril dosage/blood pressure Blood pressure/uMCP-1 Blood pressure/urinary protein ⌬ Blood pressure/⌬ uMCP-1 Total cholesterol/urinary protein Total cholesterol/uMCP-1 ⌬ Cholesterol/⌬ uMCP-1 Urinary protein/uMCP-1 ⌬ Urinary protein/⌬ uMCP-1
After 1 year of ACE1 therapy 270 ⫾ 389 (P ⫽ 0.002) 0.08 ⫾ 0.096 (P ⫽ 0.0001) 8.2 ⫾ 1.8 (NS) 4.70 ⫾ 1.00 (P ⬍ 0.05) 93.7 ⫾ 38 (NS) 77 ⫾ 41 (P ⬍ 0.03) 0.44 ⫾ 0.1 (NS) 136 ⫾ 5 (NS) 85 ⫾ 3 (NS) 30.8 ⫾ 4.7 (NS) r ⫺0.02 (NS) 0.16 (NS) 0.22 (NS) 0.18 (NS) 0.02 (NS) 0.14 (NS) 0.21 (NS) 0.26 (NS) 0.45 (NS) 0.04 (NS) ⫺0.15 (NS) 0.60 (P ⫽ 0.001) 0.61 (P ⫽ 0.001)
Data are means ⫾ SD. NS, not significant; NA, not applicable.
in proteinuria correlated well with the reduction of MCP-1 levels. There was no correlation of uMCP-1 with glycemic control, serum lipid levels, or blood pressure. These results are consistent with the findings in an animal model of diabetic
Figure 1—Change of uMCP-1 levels in individual patients before and after 1 year of ACEI therapy.
DIABETES CARE, VOLUME 26, NUMBER 8, AUGUST 2003
nephropathy. In rats with streptozotocininduced diabetes, treatment with ACEI specifically decreased renal MCP-1 mRNA and improved renal function without affecting the levels of other fibrogenic chemokines (18). In this animal model, improvement of proteinuria correlated closely with the reduction in renal MCP-1 mRNA. Glomerular and tubulointerstitial monocyte/macrophage infiltration was significantly reduced in the animals treated with ACEI or AT-II type 1a receptor antagonists. The extent of tubulointerstitial lesions is a prognostic factor for the progression of diabetic nephropathy (19). The results of our study indicate that increased intrarenal production of MCP-1 may be a pathogenic pathway also in human diabetic nephropathy. Although higher urinary levels of MCP-1 have been detected in patients with diabetic nephropathy in the macro- than in the microalbuminuric range (20,21), the connection between AT-II and MCP-1 in diabetic nephropathy is not completely understood. Because systemic blood pressure remained virtually unchanged in the study subjects, we think that predomi-
nantly nonhemodynamic actions of AT-II are responsible for the observed decrease in uMCP-1 and the accompanying improvement of renal function. Furthermore, blockade of the AT-II type 1a receptor or treatment with ACE-I is effective in reducing proteinuria in chronic renal diseases without systemic hypertension (22). The importance of nonhemodynamic mechanisms of AT-II in diabetic nephropathy has been stressed recently (23). AT-II is a direct stimulus of MCP-1 in vascular smooth muscle and in the mesangial cells of the kidney (24). AT-II itself has monocyte chemoattractant activity, and activated macrophages themselves— besides being potent sources of MCP-1— can generate AT-II via an intrinsic ACE pathway (25,26). Moreover, the infusion of AT-II into rats leads to an influx of macrophages into the kidney, which can be attenuated by the administration of an AT1a-receptor antagonist (27). In experiments with AT-1a-receptor– deficient mice, diminished expression of MCP-1 led to markedly less interstitial fibrosis and preserved renal function in a mouse 2423
Nephropathy and MCP-1
Figure 2—Change in proteinuria in individual patients before and after 1 year of ACEI therapy.
model of anti-Gbm nephritis (28). Interstitial monocyte infiltration, extracellular matrix accumulation, and fibrosis of the kidney interstitium are also characteristic histological features of diabetic nephropathy in man (29). Monocytes move along a concentration gradient to the place with highest expression of MCP-1, which in the kidneys are the proximal tubular cells (30). Here, activated monocytes/ macrophages induce proliferation and transformation of dormant fibrocytes to myofibroblasts, and interstitial scarring and tubular atrophy ensues (31).
Also, increased glomerular capillary pressure and subsequently increased protein filtration can lead to protein overload of proximal tubular epithelial cells. In response to protein overload, tubular cells can secrete MCP-1 into the tubulus and in the adjacent interstitium (32,33). Amelioration of glomerular capillary hypertension via blockade of the RAS could theoretically diminish the amount of protein in the tubular fluid, and MCP-1 secretion would subsequently decrease. Because of the impressive reduction of uMCP-1 levels in all patients and not only
Figure 3—Correlation between the difference in proteinuria (⌬ protein) and the difference in uMCP-1 levels (⌬ uMCP-1) before and after 1 year of ACEI therapy. f, regression 95% CI.
2424
in those with frank proteinuria, we think that this mechanism is probably only functional in patients with a daily protein excretion in the nephrotic range. In our study, treatment with statins for hyperlipidemia was initiated concomitantly with ACEI therapy in eight patients, and because lovastatin (34) and atorvastatin (35) have been shown to reduce MCP-1 expression in glomerular cells and vascular smooth muscle cells, respectively, we correlated the reduction in cholesterol levels in statin-treated patients with uMCP-1; however, changes in cholesterol levels did not influence uMCP-1 levels. Therefore, we conclude that in patients with type 2 diabetes and diabetic nephropathy, blockade of AT-II with ACEI may exert its beneficial effect on renal function also via suppression of the AT-II–induced tubular production of the chemokine MCP-1. This possibly results in a decrease in the number and the activity of interstitial monocytes. Subsequently, the progression of tubulointerstitial fibrosis and tubular atrophy might be slowed. This explanation for the findings in this study is consistent with the theory that AT-II/MCP-1–induced renal fibrosis is an important part of diabetic nephropathy as well as of other noninflammatory renal diseases. Long-term studies concerning the role of MCP-1 and of its specific pharmacological suppression in diabetic nephropathy are needed to further clarify this issue. References 1. Ritz E, Orth SR: Nephropathy in patients with type 2 diabetes mellitus. N Engl J Med 341:1127–1133, 1999 2. Ziyadeh FN, Goldfarb S: The renal tubulointerstitium in diabetes mellitus. Kidney Int 39:464 – 475, 1991 3. Young BA, Johnson RJ, Alpers CE, Eng E, Gordon K, Floege J, Couser WG, Seidel K: Cellular events in the evolution of experimental diabetic nephropathy. Kidney Int 47:935–944, 1995 4. Rovin BH, Phan LT: Chemotactic factors and renal inflammation. Am J Kidney Dis 31:1065–1084, 1998 5. Furuta T, Saito T, Ootaka T, Soma J, Obara K, Abe K, Yoshinaga K: The role of macrophages in diabetic glomerulosclerosis. Am J Kidney Dis 21:480 – 485, 1993 6. Gu L, Tseng SC, Rollins BJ: Monocyte chemoattractant protein-1. Chem Immunol 72:7–29, 1999 7. Prodjosadj W, Gerritsma JS, Van Es LA,
DIABETES CARE, VOLUME 26, NUMBER 8, AUGUST 2003
Amann, Tinzmann, and Angelkort
8.
9.
10.
11.
12.
13.
14.
15.
16.
Daha MR, Bruijn JA: Monocyte chemoattractant protein-1 in normal and diseased kidneys: an immunohistochemical analysis. Clin Nephrol 44:148 –55, 1995 Banba N, Nakamura T, Matsumura M, Kuroda H, Hattori Y, Kasai K: Possible relationship of monocyte chemoattractant protein-1 with diabetic nephropathy. Kidney Int 58:684 – 690, 2000 Ihm CG, Park JK, Hong SP, Lee TW, Cho BS, Kim MJ, Cha DR, Ha H: A high glucose concentration stimulates the expression of monocyte chemotactic peptide-1 in human mesangial cells. Nephron 79: 33–37, 1998 Lewis EJ, Hunsicker LG, Bain RP, Rohde RD: The effect of angiotensin-convertingenzyme inhibition on diabetic nephropathy: the Collaborative Study Group. N Engl J Med 329:1456 –1462, 1993 Ravid M, Lang R, Rachmani R, Lishner M: Long-term renoprotective effect of angiotensin converting enzyme inhibition in non-insulin dependent diabetes mellitus: a 7-year follow-up study. Arch Int Med 156:286 –289, 1996 Anderson S, Jung FF, Ingelfinger JR: Renin-angiotensin system in diabetic rats: functional, immunohistochemical and molecular biologic correlations. Am J Physiol 265:477– 486, 1993 Remuzzi A, Malanchini B, Battaglia C, Bertani T, Remuzzi G: Comparison of the effects of angiotensin-converting enzyme inhibition and angiotensin receptor blockade on the evolution of spontaneous glomerular injury in male MWF/Ztm rats. Exp Nephrol 4:19 –25, 1996 Chen XL, Tummala PE, Olbrych MT, Alexander RW, Medford RM: Angiotensin II induces monocyte chemoattractant proteine-1 gene expression in rat vascular smooth muscle cells. Circ Res 83:952– 959, 1998 Ruiz-Ortega M, Bustos C, HernandezPresa MA, Lorenzo O, Plaza JJ, Egido J: Angiotensin II participates in mononuclear cell recruitment in experimental immune complex nephritis through nuclear factor-B activation and monocyte chemoattractant protein-1 synthesis. J Immunol 161:430 – 439, 1998 Wada T, Furuichi K, Sakai N, Iwata Y, Yoshimoto K, Shimizu M, Takeda SI, Takasawa K, Yoshimura M, Kida H, Kobayashi KI, Mukaida N, Naito T, Matsus-
DIABETES CARE, VOLUME 26, NUMBER 8, AUGUST 2003
17.
18.
19.
20.
21. 22.
23. 24.
25.
26.
hima K, Yokoyama H: Up-regulation of monocyte chemoattractant protein-1 in tubulointerstitial lesions of human diabetic nephropathy. Kidney Int 58:1492– 1499, 2000 Mogensen CE, Christensen CK, Vittinghus E: The stages in diabetic renal disease, with emphasis on the stage of incipient diabetic nephropathy. Diabetes 32 (Suppl. 2):64 –78, 1983 Kato S, Luyckx VA, Ots M, Lee KW, Ziai F, Troy JL, Brenner BM, MacKenzie HS: Renin-angiotensin blockade lowers MCP-1 expression in diabetic rats. Kidney Int 56:1037–1048, 1999 Mauer SM, Steffes MW, Ellis EN, Sutherland DE, Brown DM, Goetz FC: Structural-functional relationships in diabetic nephropathy. J Clin Invest 74:1143–1155, 1984 Tashiro K, Koyanagi I, Saitoh A, Shimizu A, Shike T, Ishiguro C, Koizumi M, Funabiki K, Horikoshi S, Shirato I, Tomino Y: Urinary levels of monocyte chemoattractant protein-1 (MCP-1) and interleukin-8 (IL-8) and renal injuries in patients with type 2 diabetic nephropathy. J Clin Lab Anal 16:1– 4, 2002 Ihm CG: Monocyte chemotactic peptide-1 in diabetic nephropathy. Kidney Int 52:S20 –22, 1997 Russo D, Pisani A, Balletta MM, De Nicola L, Savino FA, Andreucci M, Minutolo R: Additive antiproteinuric effect of converting enzyme inhibitor and losartan in normotensive patients with IgA nephropathy. Am J Kidney Dis 33:851–856, 1999 Chen S, Wolf G, Ziyadeh FN: The reninangiotensin system in diabetic nephropathy. Contrib Nephrol 135:212–221, 2001 Poon M, Hsu WC, Bogdanov VY, Taubman MB: Secretion of monocyte chemotactic activity by cultured rat aortic smooth muscle cells in response to PDGF is due predominantly to the induction of JE/MCP-1. Am J Pathol 149:307–317, 1996 Goetzel EJ, Klickstein LB, Watt KWK, Weintroub BU: The preferential human mononuclear leukocyte chemotactic activity of the substituent tetrapeptides of angiotensin II. Biochem Biophys Res Commun 97:1097–1102, 1980 Okamura A, Rakugi H, Ohishi M, Yanagitani Y, Takiuchi S, Moriguchi K, Fennessy PA, Higaki J, Ogihara T: Upregulation of
27.
28.
29.
30.
31.
32.
33.
34.
35.
renin-angiotensin system during differentiation of monocytes to macrophages. J Hypertens 17:537–545, 1999 Wolf G, Schneider A, Helmchen U, Stahl RA: AT1-receptor antagonists abolish glomerular MCP-1 expression in a model of mesangial proliferative glomerulonephritis. Exp Nephrol 6:112–120, 1998 Hisada Y, Sugaya T, Yamanouchi M, Uchida H, Fujimura H, Sakurai H, Fukamizu A, Murakami K: Angiotensin II plays a pathogenic role in immune-mediated renal injury in mice. J Clin Invest 103:627– 635, 1999 El-Nahas AM, Muchaneta-Kubara EC, Essawy M, Soylemezoglu O: Renal fibrosis: insights into pathogenesis and treatment. Int J Biochem Cell Biol 29:55– 62, 1997 Prodjosudjadi W, Gerritsma JS, Klar-Mohamad N, Gerritsen AF, Bruijn JA, Daha MR, van Es LA: Production and cytokine mediated regulation of monocyte chemoattractant protein-1 by human proximal tubular epithelial cells. Kidney Int 48: 1477–1486, 1995 Gonzalez-Cuadrado S, Bustos C, RuizOrtega M, Ortiz A, Guijarro C, Plaza JJ, Egido J: Expression of leukocyte chemoattractants by interstitial renal fibroblasts: up-regulation by drugs associated with interstitial fibrosis. Clin Exp Immunol 106:518 –522, 1996 Wang Y, Chen J, Chen L, Tay YC, Rangan GK, Harris DCH: Induction of MCP-1 in proximal tubule cells by urinary protein. J Am Soc Nephrol 8:1537–1545, 1997 Wang Y, Rangan GK, Tay Y-C, Wang Y, Harris DCH: Induction of monocyte chemoattractant protein-1 by albumin is mediated by nuclear factor B in proximal tubule cells. J Am Soc Nephrol 10:1204 – 1213, 1999 Park YS, Guijarro C, Kim Y, Massy ZA, Kasiske BL, Keane WF, O’Donnell MP: Lovastatin reduces glomerular macrophage influx and expression of monocyte chemoattractant protein-1 mRNA in nephrotic rats. Am J Kidney Dis 31:190 –194, 1998 Ortego M, Bustos C, Hernandez-Presa MA, Tunon J, Diaz C, Hernandez G, Egido J: Atorvastatin reduces NF-b activation and chemokine expression in vascular smooth muscle cells and mononuclear cells. Atherosclerosis 147:253– 261, 1999
2425