Case-Fatality Rates Among Diabetic. Patients With Myocardial Infarction. Findings From National Hospital. Discharge Survey, 1979-1987. Richard S. Cooper ...
Age-Related Differences in Case-Fatality Rates Among Diabetic Patients With Myocardial Infarction
Richard S. Cooper, MD Ivan V. Pacold, MO Earl S. Ford, MD
Findings From National Hospital Discharge Survey, 1979-1987
Objective: To determine age-related differences in casefatality rates among diabetic patients with myocardial infarction (Ml). Published studies have demonstrated 60% higher case-fatality rates during acute Ml among diabetic patients compared with those without diabetes. However, many previous reports have been of insufficient size to examine the effect of age on mortality and have not been drawn from a representative sample of hospitals. The National Hospital Discharge Survey provides data on discharge diagnosis and vital status from a random sample of —500 short-stay American hospitals. Research Design and Methods: In this analysis, people with acute Ml listed as the first diagnosis on the discharge sheet were studied. Any mention of diabetes mellitus on the discharge sheet was used to stratify the patients into those with and without diabetes. Results: Age-adjusted case-fatality rates were identical in patients with and without diabetes for both sexes: 16.1 vs. 16.3 in men and 18 vs. 18.2 in women, respectively. Mortality rates were, however, higher among the younger patients with diabetes. Ratios of the case-fatality percentage by 10-yr age-groups (age 35-75 yr) and >75 yr old for diabetes versus no diabetes were 1.7, 1.8,1.2, 0.9, and 0.9 for men and 2.4, 1.2, 1.1, 1, and 0.9 for women. Conclusions: Diabetes thus appears to increase the inhospital mortality risk with acute Ml disproportionately in the younger age-groups, particularly among men, and does not appear to be a marker of increased risk among the elderly. Diabetes Care 14:903-908, 1991
From the Department of Preventive Medicine and Epidemiology, Loyola University Stritch School of Medicine, Maywood, Illinois; and the Diabetes Translation Branch, Centers for Disease Control, Atlanta, Georgia. Address correspondence and reprint requests to Richard S. Cooper, MD, Department of Preventive Medicine and Epidemiology, Loyola University Stritch School of Medicine, 2160 South First Avenue, Maywood, IL 60153. Received for publication 7 May 1990 and accepted in revised form 19 April 1991.
DIABETES CARE, VOL. 14, NO. 10, OCTOBER 1991
T
he prevalence of diabetes in the United States population is on the increase (1). Over one-third of people with diabetes >40 yr of age die of coronary heart disease (2,3)- Previous research has demonstrated consistently higher death rates from acute myocardial infarction (Ml) in patients who have diabetes (4-12). However, the published studies of mortality from acute Ml in diabetic patients were conducted before the more recently observed decline in case fatality from acute Ml (13,14). In addition, these studies did not involve a representative population-based sampling frame. We examined the in-hospital case fatality from acute Ml in a large data base drawn from a random sample of acute care U.S. hospitals, with the focus on the potential age-related effects of diabetes.
RESEARCH DESIGN AND METHODS
National Hospital Discharge Survey (NHDS) data tapes for the years 1979-1987 were obtained from the National Center for Health Statistics. The NHDS is an ongoing multistage survey of discharge sheets from representative short-stay nonfederal hospitals in the U.S. A description of the design and procedures of the NHDS has been published (15,16). Discharge sheets from —500 hospitals were abstracted, and data regarding demographic characteristics of the patients and the discharge diagnoses, procedures, and vital status at discharge were recorded (17). Data from these tapes were analyzed for acute Ml (ICD9 CM code 410) as the diagnosis listed first on the discharge sheet and for the presence or absence of diabetes mellitus (ICD9 CM code 250) listed at any other position on the discharge sheet.
903
DIABETES AND CASE FATALITY FROM M I
Age- and sex-specific population estimates for the disease categories were obtained by 10-yr age-groups beginning at 35 yr. To achieve stable estimates of event rates, the two youngest 10-yr age-groups were collapsed for some analyses. Age adjustment was accomplished by the direct method with the entire NHDS sample as the reference population. Case-fatality rates, calculated as the proportion of all people in a given age-sex-disease category that were discharged dead, were expressed as percentages. To compare the severity of comorbid conditions between diabetic and nondiabetic subjects, other listed conditions were examined. A listing of other conditions was generated, and rates of common serious illnesses were calculated. Limitations of the NHDS data set should be noted. The NHDS does not track individual patients. Thus, multiple admissions for the same person to an institution included in this survey were recorded as separate records. Data on race are also missing from 9 to 13% of the records, depending on the year. A change in coding practice in relation to acute Ml occurred in 1982. Beginning in that year, if acute Ml was recorded at any position on the discharge sheet, it was reordered to the
first position. Finally, a major limitation of this study was that no distinction was possible between insulindependent and non-insulin-dependent diabetes mellitus. Underreporting of diabetes may also have occurred, because only diagnoses appearing on the discharge sheet were coded. Diabetes is frequently not recorded on the death certificates of people who have the disease at the time of death (18). Statistical methods. Data analysis was performed with procedures available on SAS (19). We examined the significance of time trends for case-fatality rates with linear regression analysis and compared differences in agespecific case-fatality rates using the x2 test. Approximate standard errors were calculated from relative standard error curves published annually in NHDS documentation. For aggregate data, we used the standard error curves from 1983.
RESULTS Descriptive characteristics of people hospitalized for acute Ml during the period of this survey are presented in Table 1. Patients with acute Ml and coexistent dia-
TABLE 1 Descriptive characteristics of people with and without diabetes hospitalized for acute myocardial infarction (National Hospital Discharge Survey, 1979-1987) People without diabetes
People with diabetes
Age (yr) 35-44 45-54 55-64 65-74 ^75 Sex Men Women Race White Black Other Not stated Type of hospital Proprietary Church Government Nonprofit Source of payment Workmen's compensation Medicare Medicaid Other government, Title V Blue Cross Other private or commercial Self-pay No charge Other
%
95% confidence intervals
%
95% confidence intervals
2.3 9.4 25.5 34.3 28.5
1.8-2.8 8.2-10.7 22.8-28.2 30.9-37.7 25.6-31.4
5.7 14.1 24.1 28.4 27.7
4.6-6.9 12.2-16.0 21.5-26.6 25.5-31.2 24.9-30.5
51.2 48.8
46.3-56.1 44.0-53.6
64.3 35.7
58.1-70.5 32.2-39.2
83.7 7.1 2.0 7.2
78.6-88.7 6.1-8.2 1.6-2.5 6.1-8.2
85.3 5.2 1.5 8.0
80.1-90.5 4.5-6.0 1.2-1.8 6.8-9.2
8.4 21.0 16.9 53.7
7.2-9.6 18.7-23.3 15.0-18.9 48.5-58.8
9.1 20.0 20.4 50.5
7.9-10.4 17.8-22.2 18.0-22.8 45.6-55.3
1.0 57.3 10.5 2.0 12.0 13.5 2.8 0.4
0.7-1.2 51.8-62.9 9.1-11.9 1.6-2.5 10.5-13.5 11.8-15.2 2.3-3.4 0.3-0.5
0.6-1.1 45.1-54.6 8.8-11.5 1.2-1.8 12.3-15.8 17.1-21.9 2.7-4.0 0.2-0.3
0.4
0.2-0.5
0.9 49.8 10.1 1.5 14.1 19.5 3.4 0.2 0.4
0.3-0.6
Weighted numbers for people with and without diabetes 943,683 and 4,566,538, respectively. 904
DIABETES CARE, VOL. 14, NO. 10, OCTOBER 1991
R.S. COOPER, I.V. PACOLD, AND LS. FORD
25
TABLE 2 Percentage of people with acute myocardial infarction and colisting with diabetes by sex and age (National Hospital Discharge Survey, 1979-1987)
20
Women
Men
15
%
Age (yr) 35-44 45-54 55-64 65-74
10
>75
Crude Age adjusted
95% confidence intervals
%
95% confidence intervals
8.3-10.6 8.5-12.4 11.9-17.0 15.1-18.8 13.5-17.2 12.9-15.3 14.3-14.7
17.0 18.4 26.4 24.5 19.2 22.0 22.0
14.3-19.7 15.4-21.4 23.2-29.6 21.8-27.3 17.1-24.0 20.0-24.0 21.7-22.3
9.4
10.4 14.4 16.9 15.4 14.1 14.5
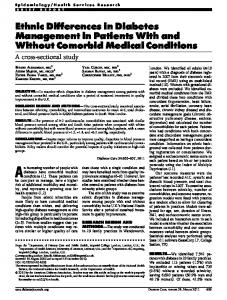
1979 1980 1981 1982 1983 1984 1985 1986 1987 Year FIG. 1. Rates of codiagnosis of diabetes mellitus among patients hospitalized with acute myocardial infarction (National Hospital Discharge Survey, 1979-1987).
betes were older, and a higher proportion of female and black patients was seen among those who had diabetes compared with those who did not. Note that the malefemale ratio of diabetic patients with acute Ml was essentially one. The sources of payment for medical care and the types of hospitals represented in the NHDS were similar in patients with or without diabetes, and therefore these factors are not likely to influence the group differences in fatality rates. In 1987, 750,901 discharges with acute Ml listed as the first diagnosis were recorded among people aged ^35 yr, and 20.1% of patients discharged also had diabetes listed as a diagnosis on the discharge sheet. The age-adjusted proportion of acute Mis that occurred in people with diabetes rose steadily between 1979 and 1987, representing one in five cases in 1987 (P = 0.003 for a linear trend; Fig. 1). The proportion of acute Mis with coexisting diabetes was higher in women than in men at all ages (Table 2).
Both crude and age-adjusted case-fatality rates for the entire study population and for men and women separately were similar in patients with and without diabetes (Table 3). However, the examination of age-specific trends revealed that the relative risk of death from acute Ml in 35- to 54-yr-old men with diabetes was substantially higher than the risk in older diabetic men compared with men of the same age who did not have diabetes (Table 4; Fig. 2). Although the ratio of the casefatality rates was 1.4 in women 35-54 yr old, the confidence intervals included unity. Among people without diabetes, the trend in case-fatality rates tended to decrease from 1980 to 1987 (P = 0.01; Figs. 3 and 4). Whether the linear trend in case-fatality rates for people with diabetes was also downward during this period is less clear; however, the case-fatality rates after 1985 were lower than those before 1983 (P = 0.019). The increase in case-fatality rates observed in 1982 probably represents changes in coding practices, as noted in METHODS.
Diabetic patients with acute Ml remained on average ~1 day longer in the hospital than patients without diabetes regardless of sex or vital status (Table 5). Furthermore, women with acute Ml were hospitalized ~1 day longer than men regardless of diabetes status. We also compared the frequency of comorbid events
TABLE 3 Crude and age-adjusted in-hospital case-fatality rates (%) for acute myocardial infarction among people with and without diabetes by sex (National Hospital Discharge Survey, 1979-1987) Crude
Men No diabetes Diabetes Women No diabetes Diabetes
Age adjusted
Case-fatality rates
95% confidence intervals
Case-fatality rates
95% confidence intervals
14.4 15.7
13.2-15.7 13.7-17.7
16.3 16.1
16.0-16.6 15.6-16.6
21.8 20.2
19.7-23.8 17.7-22.6
18.3 18.1
17.8-18.7 17.5-18.7 .
DIABETES CARE, VOL. 14, NO. 10, OCTOBER 1991
905
DIABETES AND CASE FATALITY FROM Ml
TABLE 4 Age-specific in-hospital case-fatality rates (%) for acute myocardial infarction by sex and diabetes status (National Hospital Discharge Survey, 1979-1987) Women
Men No diabetes Case-fatality rates
95% Cl
Case-fatality rates
95% Cl
Case-fatality rates
4.2 8.7
3.5-4.9 7.6-9.8 15.8-19.8 27.5-34.3
7.6 10.3 15.3 29.3
5.8-9.4 8.3-12. 3 12.7-17. 9 24.3-34. 1
1.8 1.2 0.9 0.9
Age (yr) 35-54 55-64 65-74 S75
17.8 30.9
Diabetes
No diabetes
Ratio
Diabetes
95% Cl
Case-fatality rates
95% Cl
Case-fatality rates
95% Cl
6.3-9.3 10.5-14. 2 17.4-22. 2 27.2-33. 7
10.7
7.5-13.9 11.2-16.8 16.3-22.5 22.6-30.7
1.4 1.1
0.9-1.9 0.8-1.4
1.0 0.9
0.8-1.2 0.7-1.0
95% Cl Case-fatality rates
1. 3-2.3 0. 9-1.5 0. 7-1.0 0. 8-1.1
7 .8 12 .4 19 .8 30 .5
Ratio
14.0 19.5 26.7
Cl, confidence interval.
that were listed on the discharge sheets. Conditions listed among the top 10 events were mostly cardiovascular in nature and were similar among patients with and without diabetes, although the rank order differed. Among diabetic patients, obesity (ICD9 278) was the fifth most frequently recorded comorbid condition, and among nondiabetic patients, a personal history of certain other diseases (ICD9 V12) was the ninth most frequently recorded comorbid condition.
CONCLUSIONS Coronary heart disease is the largest cause of excess mortality among diabetic subjects (1). Previous studies of the effect of diabetes on mortality with acute Ml have consistently shown higher case-fatality rates among patients with diabetes (4-11; Tables 6 and 7). Our data, based on a large random sample of U.S. hospitals, fail
35 30 ~
25
I » 1 .5 10
35-54
65-74
55-64
75+
35-54
Diabetes
FIG. 2. Age-specific case-fatality rates among women hospitalized with acute myocardial infarction (National Hospital Discharge Survey, 1979-1987).
906
75+
Age
Age No diabetes
65-74
55-64
-0-
No diabetes
Diabetes
FIG. 3. Age-adjusted case-fatality rates among men with and without diabetes mellitus by year (National Hospital Discharge Survey, 1979-1987).
DIABETES CARE, VOL. 14, NO. 10, OCTOBER 1991
R.S. COOPER, I.V. PACOLD, AND E.S. FORD
24
TABLE 6 Selected retrospective and registry studies on diabetes and case-fatality rate with diabetes and myocardial infarction
22 Case-fatality rate (%)
20
I" 0
16
Ref.
Diabetes
1No diabetes
Case-fatality ratio
Opie et al. (4) Singer et al. (5) Rytteret al. (6) Gwilt et al. (7) Molstad and Nustad (8) Yudkin and Oswald (9) Combined
28 27 42 30 26 42 31
14 16 20 19 21 25 19
2.0 1.6 2.1 1.6 1.2 1.7 1.6
14
alence, but a more important concern is the potential impact of underreporting of diabetes on case-fatality 1979 1980 1981 1982 1983 1984 1985 1986 1987 rates. For us to have obtained falsely low case-fatality rates in the diabetic patients, it would have been necYear essary for physicians to have systematically not recorded diabetes on the discharge sheets of the more severe or •- Diabetes -G- No diabetes complicated cases of acute Ml. Although we cannot rule FIG. 4. Crude case-fatality rates among patients with and out this possibility, it seems unlikely. Introduction of without diabetes by year (National Hospital Discharge Sur- new reimbursement policies may have led hospitals to list diabetes or acute Ml more frequently on the disvey, 1979-1987). charge sheets, thus inflating the number of mild cases. If this trend was important in our data, it should have emerged around 1982. However, there was no sudden to confirm the finding of overall higher case-fatality rates increase in the percentage of people with acute Ml who from acute Ml in patients with diabetes and demonstrate had diabetes during that time (Fig. 1). instead only higher rates in people 75 yr of age. It is possible that elderly patients with diabetes have relatively less severe atherosclerosis than younger patients. Recent analysis of the death certificate data indicates a marked decline in cardiovascular and coronary heart disease mortality among patients with diabetes >45 yr of age, whereas hospitalization rates for coronary heart disease continue to increase (22). These findings are consistent with the evidence of lower case-fatality rates reported among older diabetic patients in this study and may in part explain the discrepancy between our data and previous reports. Thus, a shift to a relatively larger proportion of elderly people in the universe of patients with acute Ml, and the secular trend toward falling casefatality rates, may have resulted in the elimination of the survival disadvantage due to diabetes in patients with acute Ml. Although diabetes undoubtedly continues to contribute to the risk of incident coronary heart disease, its sole impact on survival at the time of acute Ml should be reevaluated, particularly in the elderly.
Jarrett RJ, Ed. New York, Elsevier, 1984, p. 1-23 3. Barrett-Connor E, Orchard T: Diabetes and heart disease. In Diabetes in America. Harris Mi, Hamman RF, Eds. Washington, DC, U.S. Govt. Printing Office, 1985, p. XVI-1-41 (DHHS NIH publ. no. 85-1468) 4. Opie LH, Tansey MJ, Kennelly BM: The heart in diabetes mellitus. II. Acute myocardial infarction and diabetes. 5 AfrMed) 56:256-60, 1979 5. Singer DE, Moulton AW, Nathan DM: Diabetic myocardial infarction: interaction of diabetes with other preinfarction risk factors. Diabetes 38:350-57, 1989 6. Rytter L, Troelsen S, Beck-Nielsen H: Prevalence and mortality of acute myocardial infarction in patients with diabetes. Diabetes Care 8:230-34, 1985 7. Gwilt DJ, Petri M, Lewis PW, Nattrass M, Pentecost BL: Myocardial infarction size and mortality in diabetic patients. Br Heart J 54:466-72, 1985 8. Molstad P, Nustad M: Acute myocardial infarction in diabetic patients. Acta Med Scand 222:433-37, 1987 9. Yudkin JS, Oswald GA: Determinants of hospital admission and case fatality in diabetic patients with myocardial infarction. Diabetes Care 11:351-58, 1988 10. Czyzyk A, Krolewski AS, Szablowska S, Alot A, Kopczynski J: Clinical course of myocardial infarction among diabetic patients. Diabetes Care 3:526-29, 1980 11. Rytter L, Beck-Nielsen H, Troelsen S: Diabetic patients and myocardial infarction. Acta Endocrinol 262:83-87, 1984 12. Kereiakes DJ: Myocardial infarction in the diabetic patient. Clin Cardiol 8:446-50, 1985 13. Elveback LR, Connolly DC, Kurland LT: Coronary heart disease in residents of Rochester, Minnesota. II. Mortality, incidence, and survivorship, 1950-1975. Mayo Clin Proc 56:665-72, 1981 14. Goldberg RJ, Gore JM, Alpert JS, Dalen JE: Recent changes in attack and survival rates of acute myocardial infarction (1975 through 1981): the Worcester heart attack study. JAMA 255:2774-79, 1986 15. National Center for Health Statistics: Health, United States, 1985. Washington, DC, U.S. Govt. Printing Office, September 1985 (DHHS publ. no. [PHS]86-1232) 16. National Center for Health Statistics: Development of the Design of the NCHS Hospital Discharge Survey. Vital and Health Statistics. Washington, DC, U.S. Govt. Printing Office, September 1970 (PHS publ. no. 1000) 17. Feinleib M, Havlik RJ, Gillum RF, Pokras R, McCarthy E, Moien M: Coronary heart disease and related procedures: National Hospital Discharge Survey data. Circulation 79 (Suppl. 0:113-18, 1989 18. Trends in diabetes mellitus mortality. MMWR 50:769ACKNOWLEDGMENTS 73, 1988 19. SAS User's Guide: Statistics. Version 5 Edition. Cary, NC, SAS Inst., 1985 This study was presented in part at the American Heart Association 30th Annual Conference on Cardiovascular 20. Manton KG, Stallard E: Methods for evaluating the heterogeneity of aging processes in human populations using Epidemiology, San Diego, California, 29 April 1990. vital statistics data: explaining the black/white mortality crossover by a model of mortality selection. Hum Biol 53:47-58, 1981 REFERENCES 21. Roig E, Castaner A, Simmons B, Patel R, Ford E, Cooper R: In-hospital mortality rates from acute myocardial infarction by race in U.S. hospitals: findings from the Na1. Harris Ml, Hamman RF (Eds.): Diabetes in America. tional Hospital Discharge Survey. Circulation 76:280Washington, DC, U.S. Govt. Printing Office, 1985 88, 1987 (DHHS NIH publ. no. 85-1468) 2. Jarrett RJ: The epidemiology of coronary heart disease and 22. Diabetes and cardiovascular disease. In Diabetes Surveillance, 1980-1987. Atlanta, GA, Centers for Disease related factors in the context of diabetes mellitus and imControl, 1987, p. 17-21 paired glucose tolerance. In Diabetes and Heart Disease. 908
DIABETES CARE, VOL. 14, NO. 10, OCTOBER 1991