Indian J Med Res 118, July 2003, pp 25-28
Antimicrobial resistance in Enterococcus faecalis at a tertiary care centre of northern India Purva Mathur, Arti Kapil, Rachna Chandra, Pratibha Sharma & Bimal Das Department of Microbiology, All India Institute of Medical Sciences, New Delhi, India Received February 24, 2003 Background & objectives: Multiresistant enterococci are emerging as a leading nosocomial pathogen. Knowledge of the profile of antimicrobial resistance is essential to formulate treatment guidelines for infections caused by enterococci. This study reports the antimicrobial sensitivity of enterococci isolated during a one year period from clinical samples of patients admitted to a teriary care hospital of Delhi. Methods: A total of 444 isolates of Enterococcus faecalis were screened for antimicrobial susceptibility by the disk diffusion technique as recommended by the National Committee for Clinical Laboratory Standards (NCCLS). Screening for vancomycin resistance was done by the vancomycin screen agar method recommended by NCCLS, which was confirmed by determination of minimum inhibitory concentration (MIC) using microbroth dilution and E-test methods. Vancomycin resistance phenotypes were determined by polymerase chain reaction. Results: A total of 115 (26%) isolates had high level aminoglycoside resistance, 293 (66%) were resistant to ampicillin, 391 (88%) to ciprofloxacin and 377 (85%) to erythromycin. Vancomycin resistance was found in five (1%) isolates, of which four had van A phenotype and one had van B phenotype. Interpretation & conclusion: Emergence of vancomycin resistant enterococci is of concern due to the limited therapeutic options. Implementation of infection control measures can contain the spread of these resistant bacteria. Key words Aminoglycoside resistance - Enterococcus faecalis - India - vancomycin resistant Enterococcus
Enterococci have become important nosocomial pathogens world-wide and are associated with a high mortality1-3. The treatment of these infections poses a great challenge due to the inherent resistance of Enterococci to many antibiotics. A combination of penicillin and gentamicin had been the mainstay of treatment of enterococcal infections till now but with the emergence of high level aminoglycoside resistance (HLAR), vancomycin is the only alternative available1. The widespread use of glycopeptides in hospitals has led to the emergence of vancomycin resistant Enterococcus (VRE) which is a major concern for
health care professionals. VRE are frequently reported from hospitals in USA and Europe4-7. However, VRE are not a cause for concern in many Asian countries due to a low prevalence8-10. There is a paucity of information on vancomycin resistance in enterococci from our country. In this study, we present the antimicrobial susceptibility of clinical isolates of Enterococcus faecalis recovered at a tertiary care hospital in New Delhi during January to December 2001 and report the emergence of vancomycin resistance in Enterococci. 25
INDIAN J MED RES, JULY 2003
26
Material & Methods All isolates of E. faecalis recovered from clinical samples at the clinical bacteriology laboratory of the All India Institute of Medical Sciences, New Delhi during the study period were included. Antimicrobial susceptibility testing of the enterococci was performed by the disk diffusion method as recommended by the National Committee for Clinical Laboratory Standards (NCCLS)11. The antimicrobial disks (µg) used were ampicillin (10), ciprofloxacin (5), erythromycin (15), vancomycin (30) and teichoplanin (30). HLAR was determined using gentamicin (120 µg) disc. Control strains included Enterococcus faecalis, ATCC 51299 (ATCC E.f., vancomycin sensitive), Staphylococcus aureus ATCC 25923, WHO 3 (vancomycin resistant E. faecalis, Van A phenotype; vancomycin MIC 512 µg/ml), WHO 6 (glycopeptide intermediate S. epidermidis, vancomycin MIC 8 µg/ml, teichoplanin MIC 16 µg/ml), WHO 11 (vancomycin resistant E. gallinarum, vancomycin MIC 8 µg/ml, sensitive to teichoplanin), WHO 14 (vancomycin resistant E. faecalis Van B, vancomycin MIC 32 µg/ml, sensitive to teichoplanin) and WHO 20 (vancomycin resistant E. faecalis, Van B, vancomycin MIC 16 µg/ml)12. (WHO 3,6,11,14 and 20 are characterized strains which were provided to us as a part of WHO/CDC External quality assurance and proficiency testing programme)12. Screening for low level vancomycin resistance was done by vancomycin screen agar method using 6 µg/ml vancomycin according to NCCLS recommendations13. Minimum inhibitory concentration (MIC) of vancomycin was determined by microbroth dilution method13 and E-test (AB Biodisk, Sweden)14. The phenotype of vancomycin resistant strains was determined by PCR done according to standard protocols6,15. For this, DNA was isolated by the heat lysis method as described by Clark et al6. The extracted DNA (5 µl) was added to a PCR mixture (25 µl) containing 200 µM dnTPs; 2.5mM MgCl2, 1 x Taq buffer, 5 U reaction taq polymerase (Promega, USA) and each primer in 50 p moles concentration. The primers were selected from published sequences6 as follows : van A (product size 732 bp), A1, 5’-GGG AAA ACG ATT GC - 3’; A2, 5’GTA CAA TGGGCCGTTA - 3’, van B (product size 635 bp), B1, 5’ ATG GGA AGC CGA TAGTC - 3’; B2, 5’ GATTTCGTTCTTCGACC-3’; Van C (product size 822 bp), C1, 5’-GGTATCAAGGAACCTC-3’; C2, 5’ CTTCCGCCATCATAGCT-3’. Amplification of DNA
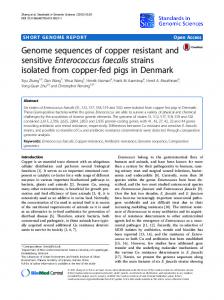
was performed in an Amplitron thermolyne II thermocycler (Barnstead Thermolyne Corporation, Dubuque, USA) with predenaturation at 94°C for 2 min, followed by 30 cycles of 94°C for 1 min, 37°C for 1 min; and 72°C for 1 min. Final extension was done at 72°C for 10 min. Amplicons were analyzed by electrophoresis on 1 per cent agarose gels along with 100 bp ladder (Boehringer Mannheim, GmbH, W. Germany) and stained with ethidium bromide. Results & Discussion A total of 444 isolates of E. faecalis were recovered from various clinical samples during the study period, of which 217 (49%) were obtained from urine samples, 170 (38%) from blood, 45 (10%) from soft tissues and 12 (3%) from the lower respiratory tract. The maximum number of isolates [209 (47%)] were obtained from patients admitted to the intensive care units (ICUs), followed by surgical words [155 (35%)], medical wards [36 (8%)] and oncology ward [44 (10%)]. Of the 444 isolates, 115 (26%) had high level aminoglycoside resistance, 293 (66%) were resistant to ampicillin, 391 (88%) to ciprofloxacin and 377 (85%) to erythromycin. Of the isolates showing HLAR, 54 were obtainted from blood, 48 from urine, 12 from soft tissues and 1 from lower respiratory tract. In a recent multicenter study, the prevalence of HLAR was reported to be 37 per cent2. With the spread of strains showing HLAR, there is now rampant use of vancomycin in hospitals since it is the only available alternative for treatment. Simultaneously, vancomycin usage has also increased in hospitals following the emergence of methicillin resistant S. aureus. Excessive use of vancomycin has been found to be a risk factor for infection or colonization by VRE 16,17. Analysis by the WHONET software programme12 revealed a gradual decline in zone diameters of vancomycin sensitive strains (Fig.), thus showing a trend towards a decreasing susceptibility to vancomycin among Enterococci. Five (1%) isolates of E. faecalis were found to be resistant to vancomycin by the disk diffusion and agar screen methods (Table). Enterococci frequently cause bacteraemia in hospitalized patients especially those on prolonged intravenous lines or antibiotic therapy18. On PCR, four isolates had van A phenotype and one had van B phenotype. Van A is the most common phenotype world-wide and confers resistance to both vancomycin and teichoplanin19.
MATHUR et al : VANCOMYCIN RESISTANT ENTEROCOCCUS FAECALIS IN NORTHERN INDIA
27
Fig. Vancomycin inhibition zone diameters of E. faecalis isolates analysed by WHONET programme (16 mm - sensitive).
Table. Characteristics of vancomycin resistant enterococci isolated in the present study Isolate no.
Source
Zone diameter (mm) (interpretation) Vancomycin
Teichoplanin
Vancomycin screen agar
MIC (µg/ml) EBroth test dilution
PCR phenotype
1.
Blood
N (R)
N (R)
R
>256
256
Van A
2.
Soft tissue
N (R)
N (R)
R
>256
256
Van A
3.
Blood
N (R)
N (R)
R
>256
512
Van A
4.
Blood
N (R)
N (R)
R
>256
256
Van A
5.
Urine
N (R)
20 (S)
R
>256
512
Van B
6. ATCCE.f
-
22 (S)
18 (S)
S
4
4
7. WHO 3
-
N (R)
10 (R)
R
>256
-
8. WHO 11
-
N (R)
17 (R)
R
8
-
9. WHO 14
-
N (R)
16 (S)
R
128
-
Van B
10. WHO 20
-
12 (R)
20 (S)
R
128
-
Van B
11. WHO 6
-
18 (S)
14 (S)
R
8
8
NA
Van A
ATCCE.f, E. faecalis vancomycin sensitive ATCC 51299; WHO 3, VRE van A; WHO 11, Vancomycin resistant E. gallinarum; WHO 14 VRE van B; WHO 20, VRE van B; WHO 6 glycopeptide intermediate S. epidermides; N, no zone; R, resistant; S, sensitive; MIC, minimum inhibitory concentration; - not done; E.f, Enterococcus faecalis; N, not applicable. All the clinical isolates were from patients admitted to the ICUs
INDIAN J MED RES, JULY 2003
28
All five isolates of VRE were recovered from patients admitted to the ICUs. Two of these patients died following VRE bacteraemia. VRE was found to be an independent predictor of death in a study done on enterococcal bacteraemia2. Surveillance cultures of the wards from which the five isolates of VRE were recovered were sterile and cultures from the hands of health care personnel also did not grow enterococci. VRE can spread rapidly in hospitals due to cross contamination and person to person spread4,20,21. It has been found that being in the same ward as a VRE case carries the highest risk for acquisition of VRE16. Hence early detection and contact isolation are important in the management. Infection by VRE was first reported in France and UK and since then it has been documented from many countries world-wide1,19,22,23. Treatment of infections caused by VRE is a challenging task, especially because the resistance appears in strains, which are multiresistant21. The optimal therapy for such infections is not known and published reports are largely anecdotal21. Measures should be taken to prevent further development and transmission of these infections by strictly implementing infection control guidelines and antibiotic policies in hospitals4,8,20. Prudent use of vancomycin and a proper surveillance for VRE may permit early recognition and containment of spread of this emerging pathogen in our country. References 1. 2.
3. 4. 5.
6.
7.
8.
Murray BE. Vancomycin resistant Enterococci. Am J Med 1997; 101 : 284-93. Vergis EN, Hayden MK, Chow JW, Snydman DR, Zervos MJ, Linden PK, et al. Determinants of vancomycin resistance and mortality rates in Enterococcal bacteremia: a prospective, multicenter study. Ann Intern Med 2001; 135 : 484-92. Meellering RC. Emergence of Enterococcus as a significant pathogen. Clin Infect Dis 1992; 14 : 1173-8. Centikaya Y, Falk P, Mayhall CG. Vancomycin-resistant Enterococci. Clin Microbiol Rev 2000; 13 : 686-707. Barnaud G, Bingen E. Genotypic characterisation of endemic Van A Enterococcus faecium strains isolated in a paediatric hospital. J Med Microbiol 2000; 49 : 793-9. Clark NC, Cooksey RC, Hill BC, Swenson JM, Tenover FC. Characterization of glycopeptide - resistant Enterococci from U.S. hospitals. Antimicrob Agents Chemother 1993; 37 : 2311-7. Gordts B, van Landuyt H, Ieven M, Vandamme P, Goossens H. Vancomycin-resistant enterococci colonizing the intestinal tracts of hospitalized patients. J Clin Microbiol 1995; 33 : 2842-6. Chong Y, Lee K. Present situation of antimicrobial resistance in Korea. J Infect Chemother 2000; 6 : 189-95.
9.
10.
11.
12.
13.
14.
15.
16.
17. 18.
19.
20.
21. 22.
Hsueh PR, Liu YC, Yang D, Yan JJ, Tu TL, Huang WK. Multicenter surveillance of antimicrobial resistance of major bacterial pathogens in intensive care unit in 2000 in Taiwan. Microb Drug Resist 2001; 7 : 373-82. Hsueh PR, Chen ML, Sun CC, Chen WH, Pan HJ, Yang LS, et al. Antimicrobial drug resistance in pathogens causing nosocomial infections at a university hospital in Taiwan, 1981-1999. Emerg Infect Dis 2002; 8 : 63-8. National Committee for Clinical Laboratory Standards. Performance standards for antimicrobiol disk susceptibility tests, vol. 20 (1); 7th ed. Approved standard. M2-A7. National Committee for Clinical Laboratory Standards. Villanova, PA 2000. Tenover FC, Mohammed MJ, Stelling J, O’ Brien T, Williams R. Ability of laboratories to detect emeging antimicrobial resistance: proficiency testing and quality control results from the World Health Organization’s external quality assurance system for antimicrobial susceptibility testing. J Clin Microbiol 2001; 39 : 241-50. National Committee for Clinical Laboratory Standards. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically. 5th ed. Approved standard. M7-A5, vol. 20 (2) Wayne, Pennsylvania: National Committee for Clinical Laboratory Standards PA 2000. Schulz JE, Sahm DF. Reliability of the E test for detection of ampicillin, vancomycin and high level aminoglycoside resistance in Enterococcus species. J Clin Microbiol 1993; 31 : 3336-9. Swenson JM, Clark NC, Ferraro MJ, Sahm DF, Doern G, Pfaller MA, et al. Development of a standardized screening method for detection of vancomycin-resistant Enterococci. J Clin Microbiol 1994; 32 : 1700-4. MacIntyre CR, Empson M, Boardman C, Sindhusake D, Lokan J, Brown GV. Risk factors for colonization with vancomycinresistant Enterococci in a Melbourne hospital. Infect Control Hosp Epidemiol 2001; 22 : 625-9. Shlaes DM. Vancomycin-resistant bacteria. Infect Control Hosp Epidemiol 1992; 13 : 193-4. Moellering RC Jr. Enterococcus species, Streptococcus bovis and Leuconostoc species. In: Mandell GL, Bennett JE, Dolin R, editors. Principles and practice of infectious diseases, 4th ed. New York: Churchill Livingstone; 1995 p. 1826-35. Scagnelli M, Pellizer G, de Lalla F, D’Emilio A, Rassu M, Bragagnolo L, et al. Epidemiological analysis of vancomycin resistant enterococci in a large tertiary care hospital in northern Italy. Eur J Clin Microbiol Infect Dis 2001; 20 : 609-16. Ishikawa K, Hayakawa S, Katayama T, Hoshinaga K, Fukaya S, Torikai K, et al. Epidemiological study of vancomycin-resistant Enterococci isolated from a single university hospital in Japan. J Infect Chemother 2001; 7 : 163-8. Murray BE. Vancomycin-resistant Enterococcal infections. N Engl J Med 2000; 342 : 710-21. Leclercq R, Derlot E, Duval J, Courvalin P. Plasmid-mediated resistance to vancomycin and teichoplanin in Enterococcus faecium. N Engl J Med 1988; 319 : 157-61.
23. Uttley AH, George RC, Naidoo J, Woodford N, Johnson AP, Collins CH, et al. High-level vancomycin-resistant Enterococci causing hospital infections. Epidemiol Infect 1989; 103 : 173-81.
Reprint requests : Dr Arti Kapil, Additional Professor, Department of Microbiology, All India Institute of Medical Sciences Ansari Nagar, New Delhi 110029, India e-mail:
[email protected]