Assessment of the Laparoscopic Training Validity of a Virtual Reality Simulator (LAP MentorTM) Tae Hyo Kim, Jung Min Ha, Jae Wook Cho, Youn Chul You, Gyung Tak Sung From the Department of Urology, College of Medicine, Dong-A University, Busan, Korea
Purpose: The need for efficient and optimal training through a structured laparoscopic training program has become increasingly evident. Virtual reality simulation may provide a safe and efficient means of acquiring laparoscopic skills. The LAP MentorTM is a high-fidelity virtual reality simulator with haptic feedback that allows a trainee to practice 9 basic laparoscopic tasks including laparoscopic suturing. The purpose of this study was to evaluate the predictive validity of performance on the LAP Mentor before surgical simulators are incorporated into training programs. Materials and Methods: Eleven participants (6 medical students and 5 residents) underwent laparoscopic skills training on the virtual reality simulator LAP Mentor. Each participant was tested on 5 sets of 4 LAP Mentor basic laparoscopic tasks (grasping, cutting, clipping, and suturing) in a 3-week period. Total time and accuracy were measured for each task. Results: There was a significant difference between the initial session and the final session for total time and accuracy in both groups. Among the medical students, as they progressed through the training step by step, total time decreased for the grasping task, the cutting task, the clipping task, and the suturing task. At the same time, accuracy improved for the grasping task, the cutting task, the clipping task, and the suturing task, respectively. The residents group showed a similar progression. Conclusions: Basic skills straining on a LAP Mentor virtual reality simulator improves learning of the basic skills for laparoscopy. Education with virtual reality simulators, therefore, may provide an effective teaching method and lead to improved operating performance. (Korean J Urol 2009;50:989-995) Key Words: Laparoscopy, Education
Korean Journal of Urology Vol. 50 No. 10: 989-995, October 2009 DOI: 10.4111/kju.2009.50.10.989
Received:June 2, 2009 Accepted:September 21, 2009 Correspondence to: Gyung Tak Sung Department of Urology, Dong-A University, 1, 3-ga, Dongdaesindong, Seo-gu, Busan 602-715, Korea TEL: 051-240-5446 FAX: 051-253-0591 E-mail:
[email protected] Ⓒ The Korean Urological Association, 2009
imperative for surgeons to acquire adequate skills [4]. In urology, approximately 40 cases have been reported to be
INTRODUCTION
sufficient for acquiring initial proficiency in laparoscopic Since the first laparoscopic nephrectomy was performed by
procedures [5,6]. In the United States, many hospitals use a
Clayman et al, laparoscopic surgery has been widely applied
training program to teach laparoscopic skills [7]. Various
in various urologic diseases [1]. Due to the advantages of
centers of excellence provide structured training programs
laparoscopic surgery, such as shortened recovery and decreased
including dry and animal labs for a training course before the
postoperative mortality, laparoscopic approaches to various
actual clinical application [8]. Because residents usually
reconstructive and ablative surgeries have been accepted as the
participate as an assistant in the laparoscopic surgery, they are
standard treatment modality [2,3]. However, laparoscopic
exposed to some laparoscopic experiences. If residents could
surgery has been associated with a steep learning curve;
participate in a structured training program, however, this
therefore, establishment of an optimal training program is
would enhance the synergic effect in terms of comprehensive
989
990
Korean Journal of Urology vol. 50, 989-995, October 2009
training in both basic and advanced laparoscopic techniques. As a training model for basic laparoscopic skills, a pelvic
box trainer is generally used to practice grasping, cutting, clipping, or suturing [5-9]. Also, various animal models are used to teach laparoscopic techniques. A swine model has been used most often because of the relative size of the abdominal cavity, but the model is somewhat expensive. Recently, a virtual reality simulator was introduced to provide surgical training on an actual clinical level and was shown to be advantageous in acquiring various basic and advanced laparoscopic techniques. A series of simulator-based programs will be very helpful for learning laparoscopic procedures and getting accustomed to the hand-eye coordination required [10]. Given the above background, we analyzed whether a virtual reality simulator is effective in enhancing the educational level
Fig. 1. Exterior view of virtual reality simulator (LAP MentorTM).
of medical students who are novices and of residents who have some experience in laparoscopic surgery through training in basic laparoscopic skills.
(1) Grasping mode: A red ball that was encased in a jelly was exposed by using a duck bill grasper. After the ball’s color was converted to green, the ball was grasped with the use of
SUBJECTS AND METHODS 1. Subjects
the other grasper and was placed in a jelly bag. (2) Cutting mode: A cutting line that was contained in a round jelly pad was pulled with one hand with the use of a
This study included a total of 11 subjects consisting of 6
retractor. Thus, the cutting area was exposed. Using the
medical students who had no prior experience in laparoscopic
contralateral hand, the cutting was done with a straight scissor.
surgery and 5 residents who had some experience in
Thus, the exposure was attempted outside of a jelly pad.
laparoscopic surgery. The subjects who took part in the
(3) Clipping mode: The red part of a duct where the water
experiment were all men, and all of them were right-handed.
flowed downward was pulled with the use of a duck bill
The average age of the medical students was 22.5 years old
grasper. When this part was converted to green, clipping was
and that of the urologic residents was 27.4 years.
done with the use of a metal clip applier.
Changes in the training stage of the subjects were monitored
(4) Suture mode: Needling was done with the use of a
by using a simulator program during a 3-week period. No
needle driver that was grasped by both hands. Thus, the suture
subjects had previously participated in laparoscopic training
area was hooked and a C-shape loop was created. After this,
with a virtual reality simulator.
a discontinuous suture where the surgeon's knot was made was
2. Methods
The simulator that was used in the current study, the LAP TM
Mentor
(Simbionix, USA), was specifically designed for
laparoscopic training (Fig. 1).
performed. The total transit time and simulator-based accuracy for each repeated technique were compared between the two groups. In each group, the changes in transit time and technical accuracy were depicted by using a progression curve. Repeated-measures
The subjects were assigned to two groups and were asked
ANOVA was used to analyze the decrease in average transit
to train on four basic techniques in accordance with the training
time and the increase in accuracy in each session and in each
guidelines proposed by the simulator. They were asked to
group. All statistical analysis was performed by using SPSS
repeatedly perform such maneuvers as grasping, cutting,
ver. 14.0.
clipping, and suturing five times each. Attempts were made to monitor changes in total time and technical accuracy.
Tae Hyo Kim, et al:Laparoscopic Training Validity of Virtual Simulator
991
time at each stage were statistically significant (p<0.001). The change in transit time was statistically significantly different at
RESULTS
each session (p=0.002). The laparoscopic procedure was repeatedly performed by
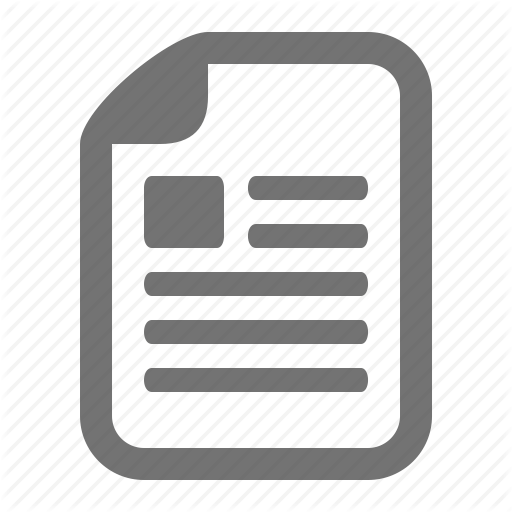
The mean accuracy for grasping increased from 54% (in the
medical students who had no experience in laparoscopic
first session) to 93% (in the fifth session) in the medical students
surgery and by residents who had participated in laparoscopic
(p=0.027). In the residents, it increased from 71% (in the first
surgery as the assistant operator. According to this, the transit
session) to 98% (in the fifth session) (p=0.043) (Fig. 2).
time was shortened and accuracy was enhanced (Table 1).
Interactions between accuracy and each group were statistically
Observations were made in a total of 11 subjects. These
significant (p=0.004). Changes in accuracy at each session were
showed that the mean transit time for grasping decreased from
statistically significant (p<0.001). Changes in accuracy were
3 minutes plus 57 seconds in the first session to 1 minute plus
statistically significantly different at each session (p<0.001).
20 seconds in the fifth session, and mean accuracy increased
The mean transit time for cutting decreased from 5 minutes
from 61% in the first session to 95% in the fifth session
plus 10 seconds (in the first session) to 2 minutes plus 20
(p=0.003). The mean transit time for cutting decreased from 4
seconds (in the fifth session) in the medical students (p=0.027).
minutes plus 29 seconds in the first session to 2 minutes plus
In the residents, it decreased from 3 minutes plus 40 seconds
1 second in the fifth session, for which mean accuracy
(in the first session) to 1 minute plus 40 seconds (in the fifth
increased from 56% in the first session to 96% in the fifth
session) (p=0.042) (Fig. 2). Interactions between transit time
session (p=0.003). The mean transit time for clipping decreased
and group were not statistically significant (p=0.058). Changes
from 4 minutes plus 22 seconds in the first session to 2 minutes
in transit time at each stage were statistically significant (p<
plus 10 seconds in the fifth session, for which mean accuracy
0.001). Changes in transit time were statistically significantly
increased from 58% in the first session to 94% in the fifth
different at each session (p<0.001).
session (p=0.003). The mean transit time for suturing decreased
The mean accuracy for cutting increased from 46% (in the
from 8 minutes plus 58 seconds in the first session to 3 minutes
first session) to 95% (in the fifth session) in the medical
plus 12 seconds in the fifth session, for which mean accuracy
students (p=0.027). In the residents, it increased from 69% (in
increased from 40% in the first session to 90% in the fifth
the first session) to 98% (in the fifth session) (p=0.043) (Fig.
session (p=0.003).
2). Interactions between accuracy and group were statistically
Changes in accuracy were monitored in both groups. The
significant (p=0.003). Changes in accuracy at each session were
mean transit time for grasping decreased from 4 minutes plus
statistically significant (p<0.001). Changes in accuracy were
20 seconds (in the first session) to 1 minute plus 50 seconds
statistically significantly different at each session (p<0.001).
(in the fifth session) in the medical students. In the residents,
The mean transit time for clipping decreased from 4 minutes
it decreased from 3 minutes plus 30 seconds (in the first
plus 50 seconds (in the first session) to 2 minutes plus 10
session) to 1 minute plus 20 seconds (in the fifth session)
seconds (in the fifth session) (p=0.027) in the medical students.
(p=0.043) (Fig. 2). Interactions between transit time and group
In the residents, it decreased from 3 minutes plus 50 seconds
were not statistically significant (p=0.511). Changes in transit
(in the first session) to 2 minutes plus 10 seconds (in the fifth
Table 1. Progress of grasping, cutting, clipping and suture in total time and accuracy by students and residents Student Group Total Time Inital Grasping 4min20sec±27sec Cutting 5min10sec±17sec Clipping 4min50sec±15sec Suture 10min20sec±57sec
Resident Group Accuracy
Total Time
Accuracy
Final
Inital
Final
Inital
Final
Inital
Final
1min50sec±19sec 2min20sec±19sec 2min10sec±18sec 3min40sec±18sec
54%±6.1 46%±5.0 53%±2.9 31%±5.9
93%±2.5 95%±2.6 92%±2.9 88%±5.1
3min30sec±35sec 3min40sec±35sec 3min50sec±24sec 7min20sec±27sec
1min20sec±15sec 1min40sec±16sec 2min10sec±21sec 2min40sec±21sec
71%±6.6 69%±5.9 65%±4.6 51%±2.9
98%±2.8 98%±1.7 97%±1.9 94%±2.2
992
Korean Journal of Urology vol. 50, 989-995, October 2009
Fig. 2. (A, B) Overall progress in grasping time (A) and accuracy (B) of two groups. (C, D) Overall progress in cutting time (C) and accuracy (D) of two groups.
session) (p=0.043) (Fig. 3). Interactions between transit time
students. In the residents, it decreased from 7 minutes plus 20
and group were statistically significant (p=0.013). Changes in
seconds (in the first session) to 2 minutes plus 40 seconds (in
transit time at each stage were statistically significant (p<
the fifth session) (p=0.043) (Fig. 3). Interactions between transit
0.001). Changes in transit time were statistically significantly
time and group were statistically significant (p<0.001).
different at each session (p=0.020).
Changes in transit time at each stage were statistically signifi-
The mean accuracy for clipping increased from 53% (in the first session) to 92% (in the fifth session) (p=0.027) in the
cant (p<0.001). Changes in transit time were statistically significantly different at each session (p<0.001).
medical students. In the residents, it increased from 65% (in
The mean accuracy for suturing increased from 31% (in the
the first session) to 97% (in the fifth session) (p=0.043) (Fig.
first session) to 88% (in the fifth session) in the medical
3). Interactions between accuracy and each group were not
students (p=0.028). In the residents, it increased from 51% (in
statistically significant (p=0.212). Changes in accuracy at each
the first session) to 94% (in the fifth session) (p=0.042) (Fig.
session were statistically significant (p<0.001). Changes in
3). Interactions between accuracy and group were statistically
accuracy were statistically significantly different at each session
significant (p=0.009). Changes in accuracy at each session were
(p=0.002).
statistically significant (p<0.001). Changes in accuracy were
The mean transit time for suturing decreased from 10 minutes plus 20 seconds (in the first session) to 3 minutes plus 40 seconds (in the fifth session) (p=0.027) in the medical
statistically significantly different at each session (p<0.001).
Tae Hyo Kim, et al:Laparoscopic Training Validity of Virtual Simulator
993
Fig. 3. (A, B) Overall progress in clipping time (A) and accuracy (B) of two groups. (C, D) Overall progress in suture time (C) and accuracy (D) of two groups.
surgical maneuvers are therefore needed [12]. Despite the
DISCUSSION
innovations and advancements in laparoscopic techniques, a proper and effective training program has not been offered. To
Thanks to its benefits and advantages, the demand for
make matters worse, the traditional training programs suffer
laparoscopic surgery is increasing in urology. Research on the
from cost-ineffectiveness. Also, residents do not have enough
current situation of Korean laparoscopic urological surgery
time to receive training [12].
shows that, although differences exist by hospital, laparoscopic
To perform laparoscopic surgery, two thing are essential.
operations are effective at many hospitals universally [11]. As
First, it is critical to understand the principles of laparoscopy
the technical innovation in laparoscopic surgery advances,
and the functions of the various laparoscopic instruments.
surgical technique training must evolve accordingly. In ad-
Second, a wide range of experiences is required before the
dition, it should be noted that laparoscopic surgery differs
actual clinical application of the procedure. Due to the various
significantly from traditional laparotomic surgery because the
complications of laparoscopic surgery, surgeons must com-
surgical concepts of laparotomy and laparoscopy are consider-
pletely understand the laparoscopic principles and the functions
ably different. In other words, the surgical concept of
of the laparoscopic instruments. They must also be aware of
laparoscopic surgery can be expressed as a two-dimensional
the
system. As a matter of fact, however, surgeons must get
complications [13]. Hence, trained experts are needed to teach
accustomed to it in a three-dimensional manner and relevant
a systematic laparoscopic training program. A generally used
preventive
and
treatment
measures
against
these
994
Korean Journal of Urology vol. 50, 989-995, October 2009
laparoscopic training model is a non-animal model called the
Various studies have examined the effectiveness of a virtual
‘pelvic box trainer,' with which trainees can be trained on basic
reality simulator. Similar to the previous literature, our study
laparoscopic techniques. Some researchers have shown that a
confirmed the effectiveness of the LAP Mentor system [17,21].
training model using pigs and rabbits produces excellent results
In most phases, the residents demonstrated a faster acquisition
[14]. When trainees use a pelvic trainer, their hand-eye
and higher accuracy of laparoscopic techniques than the
coordination improves, and they get accustomed to the
medical students did. Presumably, this was due to the gap
laparoscopic instruments. As a result, the laparoscopic training
between the two groups in terms of background knowledge and
will be intensive and drastically effective [15,16]. According to
surgical experiences. Another type of virtual reality simulator,
Derossis et al intensiveness is critical in laparoscopic training
the Lapsim, generated similar results [21,22]. Medical students
[17]. Those authors divided their subjects into two groups. One
were far behind residents in terms of performance duration and
group received training for 5 weeks, whereas the other group
accuracy in the early stages of training. However, medical
received no training. Five weeks later, the two groups
students made such significant improvement in transit time and
performed laparoscopic surgery and the outcomes were
accuracy that they were almost on a par with the residents in
compared. There is a domestic report of carrying out laparo-
the later stages of training. These findings indicate that even
scopic training with a small animal such as the rabbit [18]. In
subjects with no laparoscopic experience can acquire laparo-
another study, Traxer et al compared two groups, one of which
scopic surgical techniques through a simulated training program
was trained with a pelvic trainer and one of which received
within a short period of time.
animal training [19]. Those authors reported that the latter
The study subjects were medical students and residents who
group performed better. Several studies on the clinical ap-
could not spare enough time for this experiment and therefore
plication of laparoscopic training have shown that surgeons
did not receive intensive training. This may explain why the
with laparoscopic techniques performed varicocelectomy or
learning curve was not shortened as had been expected.
pelvic lymphadenectomy an average of 9 times in the past 1-6
Furthermore, the sensor of the simulator was extremely
years [15]. In addition, 5 years after training on laparoscopic
sensitive to the slightest difference in manipulation, which
techniques, various laparoscopic surgeries were performed by
hindered the subjects from smoothly moving to the next level.
an average of 54% of training surgeons. Twelve months after
A comprehensive and effective laparoscopic training program
the training course was completed, 25 cases of laparoscopic
would place a trainee first in a virtual-reality-simulator-based
surgery were performed annually on average [20].
laparoscopic training, followed by previously suggested animal
The disadvantage of a training program is that learning the
experimentation. Our study would be a good guideline for
surgical technique in a training program is tedious, inefficient,
residents and medical students in other specialty areas who
and cost-ineffective. Furthermore, it is doubtful that each
wish to acquire laparoscopic surgical techniques.
training process is sufficient for the clinical application of a surgical technique. On the other hand, by using a virtual reality
CONCLUSIONS
simulator, we were able to conduct effective laparoscopic training in terms of cost-effectiveness and technical aspects.
The learning capability of the subjects, who were trained
Maneuvering a virtual reality simulator is not greatly different
with a virtual reality simulator and acquired fundamental
from maneuvering the laparoscopic instruments with which
laparoscopic techniques, improved in a short period of time.
surgery is performed in humans. Because a virtual reality
Therefore, a training program for laparoscopic surgical
simulator produces images almost identical to the actual
technique based on a virtual reality simulator can be used as
procedure, medical students and residents who want to learn
an effective primary method for residents and medical students
laparoscopic techniques at an early stage can be trained
who have no experience at all or insufficient experience in
anywhere and anytime. Our study shows that the parameters
laparoscopic surgery. Trainees can efficiently improve their
assessed improved through the training based on a virtual
surgical techniques in a short period of time by receiving
reality simulator, even though the 11 subjects had different
various laparoscopic training. In addition, they would be more
laparoscopic experience.
comfortable with the technique and more confident in
Tae Hyo Kim, et al:Laparoscopic Training Validity of Virtual Simulator
performance. Henceforth, if we develop a comprehensive guideline for laparoscopic training, incorporating further experiments, a systematic and effective laparoscopic training program will be possible.
REFERENCES 1. Clayman RV, Kavoussi LR, Soper NJ, Dierks SM, Meretyk S, Darcy MD, et al. Laparoscopic nephrectomy: initial case report. J Urol 1991;146:278-82. 2. Guillonneau B, Abbou CC, Doublet JD, Gaston R, Janetschek G, Mandressi A, et al. Proposal for a “European Scoring System for Laparoscopic Operations in urology”. Eur Urol 2001; 40:2-6. 3. Guillonneau B, Rozet E, Cathelineau X, Lay F, Barret E, Doublet JD, et al. Perioperative complications of laparoscopic radical prostatectomy: the Montsouris 3-year experience. J Urol 2002;167:51-6. 4. Kim HH. Laparoscopic surgery in urology (I). Korean J Urol 2003;44:945-58. 5. Hoznek A, Katz R, Gettman M, Salomon L, Antiphon P, de la Taille A, et al. Laparoscopic and robotic surgical training in urology. Curr Urol Rep 2003;4:130-7. 6. Gill IS, Zippe CD. Laparoscopic radical prostatectomy: technique. Urol Clin North Am 2001;28:423-36. 7. Shalhav AL, Dabagia MD, Wagner TT, Koch MO, Lingeman JE. Training postgraduate urologists in laparoscopic surgery: the current challenge. J Urol 2002;167:2135-7. 8. Dent TL. Training, credentialling, and granting of clinical privileges for laparoscopic general surgery. Am J Surg 1991; 161:399-403. 9. Medina M. Formidable challenges to teaching advanced laparoscopic skills. JSLS 2001;5:153-8. 10. Zhang A, Hünerbein M, Dai Y, Schlag PM, Beller S. Construct validity testing of a laparoscopic surgery simulator (Lap Mentor): evaluation of surgical skill with a virtual laparoscopic
995
training simulator. Surg Endosc 2008;22:1440-4. 11. Lim DJ, Kim HH, Moon YT, Park YY, Yang SK, Yoon SJ, et al. Endourologic procedures and laparoscopic surgery in urology training hospitals: the report of nationwide survey. Korean J Urol 2004;45:714-9. 12. McDougall EM, Corica FA, Boker JR, Sala LG, Stoliar G, Borin JF, et al. Construct validity testing of a laparoscopic surgical simulator. J Am Coll Surg 2006;202:779-87. 13. Summers AN, Rinehart GC, Simpson D, Redlich PN. Acquisition of surgical skills: a randomized trial of didactic, videotape, and computer-based training. Surgery 1999;126: 330-6. 14. Ahn KI, Bae KS, Lee JW, Park JM, Lee DK, Jeon SH. A model and a program for training laparoscopic urethrovesical anastomosis. Korean J Urol 2006;47:407-11. 15. Melvin WS, Johnson JA, Ellison EC. Laparoscopic skills enhancement. Am J Surg 1996;172:377-9. 16. Sreenivas VI, Pothula V. Videolaparoscopy in general surgery. An update. N C Med J 2001;62:205-9. 17. Derossis AM, Bothwell J, Sigman HH, Fried GM. The effect of practice on performance in a laparoscopic simulator. Surg Endosc 1998;12:1117-20. 18. Kim TH, Sung GT, Cho WY. Development of laparoscopic training protocol using small animal model in urology. Korean J Urol 2005;46:741-9. 19. Traxer O, Gettman MT, Napper CA, Scott DJ, Jones DB, Roehrborn CG, et al. The impact of intense laparoscopic skills training on the operative performance of urology residents. J Urol 2001;166:1658-61. 20. Hawasli A, Featherstone R, Lloyd L, Vorhees M. Laparoscopic training in residency program. J Laparoendosc Surg 1996;6: 171-4. 21. Berguer R, Gutt CN. Laparoscopic colon surgery in the rat model. A preliminary report. Surg Endosc 1994;8:1195-7. 22. Berguer R, Gutt C, Stiegmann GV. Laparoscopic surgery in the rat. Description of a new technique. Surg Endosc 1993; 7:345-7.