Emergency Medicine Australasia (2018) 30, 18–35
doi: 10.1111/1742-6723.12907
REVIEW ARTICLE
Review article: Best practice management of low back pain in the emergency department (part 1 of the musculoskeletal injuries rapid review series) Kirsten STRUDWICK Trevor RUSSELL3
,1,2,3 Megan MCPHEE,2 Anthony BELL,4,5 Melinda MARTIN-KHAN6 and
1
Emergency Department, Queen Elizabeth II Jubilee Hospital, Metro South Hospital and Health Service, Brisbane, Queensland, Australia, Physiotherapy Department, Queen Elizabeth II Jubilee Hospital, Metro South Hospital and Health Service, Brisbane, Queensland, Australia, 3 School of Health and Rehabilitation Sciences, The University of Queensland, Brisbane, Queensland, Australia, 4Emergency and Trauma Centre, Royal Brisbane and Women’s Hospital, Metro North Hospital and Health Service, Brisbane, Queensland, Australia, 5Faculty of Medicine, The University of Queensland, Brisbane, Queensland, Australia, and 6Centre for Health Services Research, Faculty of Medicine, The University of Queensland, Brisbane, Queensland, Australia 2
Abstract Low back pain (LBP) is a common presentation to the ED, and a frequent cause of disability globally. The ED management is often associated with high rates of imaging, misuse and overuse of pharmacology and subsequent financial implications. Given this, improved quality of care for patients with LBP in ED is essential. This rapid review investigated best practice for the assessment and management of LBP in the ED. PubMed, CINAHL, EMBASE, TRIP and the grey literature, including relevant organisational websites, were searched in 2015. Primary studies, systematic reviews and guidelines were considered for inclusion. English-language articles published in the past 10 years that addressed acute LBP assessment, management or prognosis in the ED or acute setting were included. Data extraction of included articles was conducted, followed by quality appraisal to rate the level of evidence where possible. The search revealed 1538 articles, of which 38 were
included in the review (n = 8 primary articles, n = 13 systematic reviews and n = 17 guidelines). This rapid review provides clinicians managing LBP in the ED a summary of the best available evidence to risk stratify and enhance the quality of care, optimising patient outcomes. Consistent evidence was found to support the use of ‘red flags’ to screen for serious pathologies, diagnostic tests being reserved for use only in the presence of red flags, the judicious prescribing of opioids, identification of psychosocial risk factors as predictors of poorer outcome and promotion of early return to work and function. Key words: emergency medicine, evidence-based practice, low back pain, review, sciatica.
Introduction Low back pain (LBP) is the highest ranked cause of disability globally.1 The most recent Australian data suggests one in seven Australians
Correspondence: Ms Kirsten Strudwick, Emergency Department, Queen Elizabeth II Jubilee Hospital, Locked Bag 2, Archerfield, QLD 4108, Australia. Email: kirsten.
[email protected] Kirsten Strudwick, BPhty (Hons), Emergency Physiotherapy Practitioner; Megan McPhee, BPhty (Hons), Physiotherapist; Anthony Bell, MBBS, FACEM, MBA, MPH, FRACMA, Director Emergency Department; Melinda Martin-Khan, PhD, MHthSc, GCSc (Stat), BEd (Hons), BCom (Acc), DipMan, Health Scientist; Trevor Russell, BPhty, PhD, Professor. Accepted 22 March 2017
Key findings • Screen for red flags in all patients with LBP. • Use imaging and opioids judiciously. • Identify yellow flags for predicting those at risk of a poor prognosis. • Promote early return to work and function. reported back pain in 2011–2012, and over two in five of these people reported limitations in activity due to their back problems.2,3 In Australia, healthcare expenditure due to LBP is also significant, estimated to total $1.2 billion in 2008–2009, not accounting for lost productivity.4 In one Western Australian study, LBP accounted for 22 655 ED presentations (1.9% of total) between 2000 and 2004, with an average length of stay in ED of 4.4 h.5 From these presentations, 43.8% were categorised as having ‘muscular’ LBP, and 17.1% of these patients were admitted with an average length of stay at 6.4 days.5 More recent data from an Australian metropolitan hospital has reported higher prevalence, with 2.2% of all presentations in 2013 being due to LBP, and 32.2% of these patients being admitted.6 Hospital admission accounts for significantly greater expenditure,7,8 estimated at 47.6% ($560 million) of the total healthcare
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
19
MUSCULOSKELETAL RAPID REVIEW SERIES: LOW BACK PAIN
expenditure on LBP.4 This suggests LBP is a common complaint requiring a significant outlay of healthcare resources and continues to be a substantial source of disability in the wider population. On presentation to the ED, the primary aim is to exclude serious pathology, which may require immediate intervention (such as fractures, malignancies, spinal cord or cauda equina compression). Thereafter, the ED management of LBP ideally focuses on controlling pain and restoring patient function.9 This usually includes patient education, reassurance, advice and simple analgesics.10 Patients with LBP often present to ED with high expectations of analgesia and investigations, which can make adhering to assessment and management guidelines challenging.11 In addition, the National Emergency Access Target focuses on time-related outcomes, increasing the pressure to diagnose, manage and discharge patients rapidly, which may impact on the quality of care.12,13 Thus, despite clear management aims and the availability of clinical guidelines, the practical and environmental pressures of ED often lead to wide variations in care.14,15 It has been shown that compliance with evidence-based clinical guidelines for the management of patients with LBP can offer improvements in pain relief and patient satisfaction, and reduce the need for ongoing care.16 In such guidelines, practitioners are strongly advised to limit the use of imaging17,18 and use a stepwise approach in prescribing analgesics.19 Despite these guidelines, American data from the past decade indicates there has been a three-fold increase in the use of advanced imaging techniques (both magnetic resonance imaging and computed tomography, up to 11.3%), with stable use of radiographs (17%), and an increase in prescription opioid use (29.1%, up to 61% at discharge) in place of simple analgesics.20,21 In Australia, the available data also suggest high rates of imaging in ED, with radiography requested for 26.2% of patients and advanced imaging
requested for 5.6% of patients.6 These approaches offer no improvements to patient outcomes, increase exposure to the risks of opioid medications use and unnecessary radiation and lead to increases in the economic burden of LBP.16,22–24 There are multiple reasons why a patient may attend an ED rather than seeking general practitioner (GP) care. Reasons that are not specific to the LBP population include: reduced availability of and access to GPs; limited access to after-hours GP care; the gradual shift in GPs charging co-payments for consultations and the rise in ambulance utilisation where the ED is the universal destination point. Specific to the LBP patient population, they may also perceive a more urgent need for medical attention due to high levels of pain or inability to function. The ED may also be viewed as a ‘onestop shop’ that provides the relevant medications and diagnostics for their LBP, at no cost to the patient, whereas they are likely to incur these costs in the primary care setting.25 For most patients with LBP, the condition is self-limiting, with rapid improvements in pain and function experienced in the first 6 weeks.26,27 However, in patients who seek treatment outside of the ED, high recurrence rates have been reported,28 and nearly one-third may not have recovered at 12 months after their first presentation.29 There is increasing emphasis on the role of psychosocial factors in identifying patients at risk of transitioning to chronic pain, but early screening and appropriate management of these risk factors is not routinely performed in the ED.30 These patients, with a lack of resolution of symptoms, may also contribute to the large number of LBP presentations to the ED. Given the burden of disease and financial impacts, high quality care of patients with LBP in the ED is essential. A rapid review was undertaken to identify the current best evidence for patients with acute LBP in the ED setting across the clinical cycle of care, including assessment, diagnostics, treatment and considerations for discharge and follow
up. This rapid review forms part of a larger series, which is outlined in the corresponding methodology paper.31
Methods Search strategy A rapid review, which is a streamlined approach to synthesising evidence, was conducted in March– April 2015 of the past 10 years of scientific literature, including guidelines, primary articles and systematic reviews pertaining to quality care of LBP in the ED. The methodology for the review is outlined in more detail in the corresponding methodology paper.31 Table 1 provides details of the literature search and selection process for this review.
Study selection and analysis Primary studies, systematic reviews and guidelines were considered for inclusion. Articles were screened at title, abstract and full-text level by applying the inclusion/exclusion criteria. The National Health and Medical Research Council (NHMRC) levels of evidence hierarchy32 was chosen to rate the levels of evidence as the scope of the review was quite broad, yielding articles utilising many different research designs (i.e. intervention, diagnosis, prognosis, aetiology and screening studies). Each primary article and systematic review was independently assigned a level of evidence by two members of the research team. Disagreement was resolved by reaching consensus and the research team was consulted if agreement could not be reached. All guidelines reported their own quality grading system within the guideline; therefore, insufficient information was available to be able to grade these articles against the NHMRC levels of evidence. Of the primary studies, only Level II studies, as per the NHMRC levels of evidence hierarchy, were included (i.e. highest level of intervention, diagnostic accuracy and prognostic studies). Studies that were Level III-1 or lower were included in which
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
20
K STRUDWICK ET AL.
TABLE 1.
Literature search and selection criteria
Databases searched
PubMed, CINAHL, EMBASE, TRIP Database Grey literature search of relevant websites and organisations
Search terms
Combined MESH and keyword search using terms related to emergency medicine AND best practice AND low back pain (and variations of back pain) Individual database searches are presented in Appendix S1
Inclusion criteria
English language Published between 2005 and April 2015 Concerning low back pain of musculoskeletal origin, or ‘red flag’ conditions that can mimic musculoskeletal low back pain Adults only
Exclusion criteria
Chronic low back pain without acute flare up Surgical techniques or surgical management of fractures, cauda equina/cord compression Study setting or intended users external to the ED or findings not applicable to ED practice Qualitative studies, case studies, conference abstracts, commentaries and Letters to the Editor
Quality assessment
Data extraction by one author against a standardised form; checked by a second author Articles assigned NHMRC level of evidence32 by two authors independently (see page 15 of this reference for further details https://www.nhmrc. gov.au/_files_nhmrc/file/guidelines/developers/ nhmrc_levels_grades_evidence_120423.pdf) Disagreements were discussed to reach a consensus
safety and ethics concerns may have limited prospective research in that area, such as in the case of cauda equina. Systematic reviews of all evidence levels were included. Guidelines were included if the methodology for development was clearly documented.
Results Search results The initial search, following exclusion of duplicates and non-English articles, identified 1538 articles for screening (Fig. 1). At full text, eightprimary articles,33–40 13 review articles27,41–52 and 17 guidelines53–69 were included.
Article characteristics and levels of evidence Characteristics of the 38 included articles are shown in Tables 2–4. The included articles ranged from Level I to IV evidence, with Level I being considered highest in the NHMRC hierarchy, based on the probability that the research designs at this level have minimised the impact of bias on the results. Of the primary articles, five were interventional randomised controlled trials providing Level II evidence, and the remaining three articles were retrospective chart reviews describing diagnostic accuracy and/or prognosis of Level II–IV evidence. These lower level studies were included to offer a comprehensive picture given the
safety and ethical concerns with performing prospective research in some conditions. The systematic review articles included a mix of Level II interventions (n = 4), Level III-2 interventions (n = 1), Level II diagnostic accuracy (n = 4), Level II combined intervention and diagnostic accuracy (n = 1), Level II prognosis (n = 2) and a Level II qualitative review (n = 1). All included guidelines were based on literature review and expert consensus, but varied in formatting and use of critical appraisal tools.
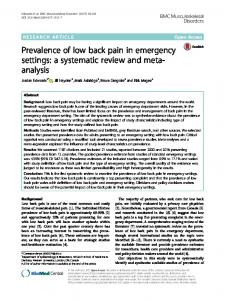
Evidence across the clinical cycle of care in the ED The included articles covered many aspects of the clinical cycle of care for the ED management of LBP, and the major findings and recommendations have been summarised in Figure 2. The findings from each included article have been synthesised into different aspects of the clinical cycle and are presented in Appendix S2.
Initial assessment There is evidence to support screening for ‘red flags’ to exclude serious pathologies. The specific conditions and ‘red flag’ signs varied between articles and are listed in Figure 2. This recommendation is supported by primary articles (n = 1 article of Level II evidence, n = 2 articles of Level III-2 evidence), systematic reviews (n = 6 articles of Level II evidence) and guidelines (n = 8). The importance of identifying psychosocial risk factors, known as ‘yellow flags’, was recommended in systematic reviews (n = 2 articles of Level II evidence) and guidelines (n = 6), reflecting the suggested value of this information in predicting those at risk of a poor prognosis.
Imaging and diagnostic tests Evidence supporting the selection, or non-selection, of imaging was covered in systematic reviews (n = 3 articles of Level II evidence), and guidelines (n = 11). It was consistently concluded that imaging should only be used in the case of trauma or
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
21
MUSCULOSKELETAL RAPID REVIEW SERIES: LOW BACK PAIN
Referrals and follow up Records identified through database search (n = 1571 ) PUBMED: n = 60 CINAHL: n = 112 EMBASE: n = 245 TRIP (systematic reviews): n = 118 TRIP (guidelines): n = 1036
Additional records identified through grey literature search (n = 8)
Records screened for duplicates and non-English language (n = 1579) Duplicates and non-English language articles removed (n = 41) Records screened on title and abstract (n = 1538)
Records excluded at title and abstract (n = 1401) Title: n = 1261 Abstract: n = 140
Full-text articles assessed for eligibility (n = 137)
Records excluded at full-text (n = 99)
Studies included in review (n = 38)
Results data not specific to LBP: n = 5 Setting not applicable to the ED: n = 9 Failed level of evidence criteria: n = 44 Failed guideline methodology criteria: n = 35 Primary article included in a systematic review: n = 3 Demographics only reported: n = 4
Primary studies: n = 8 Systematic reviews: n = 13 Guidelines: n = 17
Figure 1. PRISMA flow diagram.
when red flags were present in the assessment. Specific recommendations for each imaging modality are presented in Figure 2. Pathology tests were not routinely recommended in the management of LBP, but should be reserved for the role of excluding serious conditions. This was supported by evidence in a systematic review (n = 1 article of Level II evidence) and guidelines (n = 4).
Treatment Several articles addressed the importance of differentiating LBP between different diagnoses: the majority of LBP as those that have no pathoanatomical cause, those that are associated with radiculopathy or spinal stenosis and the minority of cases whose pain is caused by a serious
condition with a specific diagnosis. This evidence was reflected in systematic reviews (n = 3 articles of Level II evidence) and guidelines (n = 5). The diagnosis and severity of symptoms should then guide the management, where the judicious use of analgesia, particularly opioids, was supported by evidence in primary articles (n = 4 articles of Level II evidence), systematic reviews (n = 2 articles of Level II evidence) and guidelines (n = 8). It was recommended that the management of LBP in ED also include nonpharmacological strategies such as targeted education and reassurance, cold or heat and exercise recommendations. These were evidenced in a primary article (n = 1 article of Level II evidence), systematic reviews (n = 2 articles of Level II evidence) and guidelines (n = 8).
Follow up was considered in systematic reviews (n = 4 articles of Level II evidence, n = 1 article of Level III-2 evidence) and guidelines (n = 8), which broadly included GP, surgical, specialist and allied health referrals. Early follow up for patients with identified ‘yellow flags’ was recommended in a systematic review (n = 1 article of Level II evidence) and guidelines (n = 4). For those patients with a chronic history or persistent pain, guidelines (n = 4) indicated community health involvement or referral to a multidisciplinary pain management team. It was suggested in guidelines (n = 5) that an early return to work, even if on modified duties, should be encouraged to promote better patient outcomes.
Discussion This rapid review identified several key points integral to providing quality care for musculoskeletal patients within the ED. Broadly, this includes the exclusion of sinister pathologies, identification of psychosocial risk factors for poor prognosis, imaging only in the presence of ‘red flags’, first-line use of simple analgesics, judicious use of shortacting opioid analgesics in severe pain (if at all), education to regain function and increase general exercise, encouraging GP follow up and promoting early return to work in some capacity. Some of these key points, such as excluding sinister pathology, may already be common practice in many EDs. However, other key points such as psychosocial screening, judicious use of imaging and opioid analgesics and early return to work or activity promotion, may represent areas where inconsistencies in care exist.
Medical imaging and other diagnostic tests Articles reviewed consistently recommended avoiding routine imaging in patients with acute LBP. In line with this, the recent ‘Choosing Wisely Australia’ campaign made the
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
2010
2007
2008
Garra et al.37
Jalloh and Minhas38
Lau et al.39
Outcome
Presenting S&S of spinal cord and cauda equina syndrome & incidence of misdiagnosis
Reasons for delay in management of cauda equina syndrome and determine commonly presented features
Retrospective chart review (diagnostic accuracy)
Risk factors associated with serious pathology
RCT Effect of early (intervention) physiotherapy intervention
Retrospective chart review (prognosis and diagnostic accuracy)
RCT Analgesic effect of heat (intervention) vs cold
RCT Analgesic effect of (intervention) i.v. paracetamol vs i.v. morphine vs i.v. dexketoprofen given at presentation
Retrospective chart review (diagnostic accuracy)
RCT Analgesic effect of (intervention) promethazine as adjunct to morphine vs morphine alone
RCT Analgesic effect of (intervention) i.v. dexamethasone in addition to routine treatment
Study design
√
NA
√
√
√
√
X
√
√
X
NA
√
√
X
√
√
Sample size Appropriate calculation randomisation
NA
†
NA
X
‡
NA
†
‡
Blinded
√
NA
NA
NA
NA
X
NA
NA
√
√
√
X
√
NA
√
√
√
√
√
NA
NA
√
NA
NA
NA
NA
√
NA
NA
NA
NA
NA
NA
√
NA
√
√
NA
√
√
n = 329
n = 99
n = 32
n = 60
n = 137
n = 63
n = 59
n = 58
NHMRC level of evidence
Level II
Level II
Level II
1. Proportion with Level II risk factors not completed.
1. Unclear statistical significance.
1. No statistical Level IV methods. prognosis; 2. Sample size not Level III-2 powered. diagnosis
1. Results favour null hypothesis, likely type 2 error. 2. No control or blinding.
1. Only i.v. used. Level II 2. No superiority does not mean all drugs equal. 3. Outcomes at 30 min only.
1. Not statistically Level III-2 powered. 2. Not blinded.
1. Different halflives but outcomes taken at same time point.
1. 50% outcomes observations and >80% considerations
scale.
†, Single blinding; ‡, double blinding; √, yes; X, no; D/C, discharge; LOS, length of stay; NA, not applicable; OPD R/V, outpatient review; RCT, randomised controlled trial; S&S, signs and symptoms; SLR, straight leg raise; VAS, visual analogue
Thiruganasam2013 bandamoorthy et al.40
2014
Eken et al.36
2013
Behrbalk et al.34
2011
2014
Balakrishnamoorthy et al.33
Dugas et al.35
Year
Reference
TABLE 2. Primary article characteristics
22 K STRUDWICK ET AL.
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
et al.44
Henschke
et al.45
Henschke
et al.43
Downie
Search dates and
always stated and there is no
2. Levels of evidence are not
have citations throughout.
imaging in the ED
assessment and radiologic
pertaining to laboratory
√
√
√
more of the 11 methodological quality items).
at two independent authors at each stage
hand-searched reference lists
by taking a clinical history and conducting a physical examination
2. Small number of studies
studies scored fulfilled six or
patients appraisal performed by EMBASE, CINAHL,
characteristics identified
accuracy)
systematic review (3/8 of the
performance of clinical
(diagnostic
n = 6622
n = 8 papers, 1. Poor quality of studies in
blinding.
extraction and critical
Literature review, data
of bias). 2. Most studies have unclear
MEDLINE, OldMedline,
2013 Cochrane review To assess the diagnostic
Inception – 2012,
two independent authors
reference lists
(3/12 studies had a low risk
methodological quality items
patients appraisal performed by
CINAHL, hand-searched
fracture in LBP patients
accuracy)
diagnosing vertebral
n = 12 papers, 1. Low number of studies and inadequate reporting of
Literature review, data
n = 7147
Inception – 2007,
extraction and critical
of clinical features in
(diagnostic
MEDLINE, EMBASE,
2008 Systematic review To determine the accuracy
care
secondary or tertiary
with LBP to primary,
in patients presenting
poorly described.
2. Reference standards or
varied.
1. Methodological quality
diagnostic criteria were often
n = 14
authors at each stage
√
√
fracture or malignancy
appraisal performed by
√
of heterogeneity.
at least two independent
EMBASE, CINAHL
red flag signs and
accuracy)
extraction and critical
Level II
Level II
Level II
Level II
1. Meta-analysis has high level Level III-2
symptoms to screen for
MEDLINE, OldMedline,
diagnostic accuracy of
(diagnostic
Literature review, data
searched reference lists
cauda equina syndrome
(intervention) Inception – 2013,
evidence
Scholar, Scopus, hand-
surgical intervention for
analysis
2013 Systematic review To review the evidence on
NHMRC levels of
Cochrane, Google
Searched 2013: MEDLINE, Categorised according to
regarding the timing of
and meta-
author.
3. Performed by only one
included studies.
n = 24
113 listed
1. Clinical pathway does not
and considerations Unknown,
level of evidence
observations
NHMRC
Methodological
Number of inclusions
table of the characteristics of
?
√
assessment
bias
risk stratification
√
?
methods
Statistical Risk and
provides guidance on
into recommendations
appraisal and synthesis
Cochrane
evaluation of the patient with LBP, and it
extraction, critical
Literature review with data
Data collection process
Ovid MEDLINE,
1990–2013 – PubMed,
information sources
based rationale for the
Chau et al.42 2014 Systematic review To review the evidence
(intervention)
2013 Systematic review To explore an evidence-
Objective
Borczuk41
Study design
Year
Reference
TABLE 3. Review article characteristics
MUSCULOSKELETAL RAPID REVIEW SERIES: LOW BACK PAIN
23
47
et al.51
Kumar
Koes et al.49
Jenkins et al.
Notley48
and
recommendations, the membership of the guideline committee, the target population and
Institute for Health and Clinical Excellence, hand-searched reference lists
(intervention)
two independent authors
Search Premier, ANZRC, CINAHL,
LBP
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine PsycINFO, ProQuest
Scopus, Web of Science,
Cochrane Library,
SPORTDiscus, PubMed,
HealthSource,
considered weak. appraisal performed by
ICONDA, Academic
treatment of non-specific
1. The methodological quality
critically analysed.
2. Guidelines included not
country.
therapy for the
n=9
stated. 1. Only one guideline per
varied, overall articles were
√
n = 15
extraction and critical
X
√
MEDLINE, AMED,
Literature review, data
based on evidence
recommendations were
?
effectiveness of massage
2000–2012 – EMBASE,
on content of the
Clearinghouse, National
management of LBP
accuracy)
2013 Systematic review To investigate the
extracting information
Guideline
guidelines for the
and diagnostic
the extent
to four guidelines,
PEDro, National
international clinical
(intervention
Each author extracted three
2. Chronicity of LBP not
important effects.
despite potentially clinically
two independent authors
Cochrane
imaging for LBP
lack of statistical significance
appraisal performed by
EMBASE, CINAHL,
reducing the use of
1. Lack of power within some
2. Qualitative study designs.
other countries.
limited generalisability to
1. Most studies were British,
studies.
interventions aimed at
n=7
included. 3. Unclear blinding in most
included studies resulted in
√
n = 28
observations and considerations
Methodological
Number of inclusions
extraction and critical
?
√
assessment
bias
2014, MEDLINE,
Literature review, data
X
methods
Statistical Risk and
effectiveness of
Beginning of databases –
two independent authors
analysis performed by
grey literature search
dissatisfaction
thematic content
CINAHL, PsycINFO,
critical appraisal and
Literature review with
Data collection process
sources of satisfaction or
MEDLINE, EMBASE,
Inception – 2012,
2010 Systematic review To compare the content of 2000–2008 – MEDLINE,
(intervention)
Search dates and information sources
sciatica patients and the
of healthcare of LBP and
2015 Systematic review To investigate the
(qualitative)
LBP
patients presenting with
spinal malignancy in
(‘red flags’) to screen for
2013 Systematic review To describe the experience
Objective
Hopayian
Study design
Year
Reference
TABLE 3. Continued
Level II
Level II
Level II
Level II
of evidence
level
NHMRC
24 K STRUDWICK ET AL.
Year
Reference
46
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
√, yes; X, no; LBP, low back pain.
at each stage
lists
examination to screen for
LBP
patients presenting with
vertebral fracture in
two independent authors
hand-searched reference
history or physical
studies.
3. Unclear blinding in some
included.
in systematic review. 2. Small number of studies
1. Poor quality of most studies Level II appraisal performed by
n=8
EMBASE, CINAHL,
√
obtained in a clinical
accuracy)
√
of included studies.
extraction and critical
accuracy of red flags
(diagnostic
limited statistical power. 3. Low methodological quality
MEDLINE, OldMedline,
2013 Cochrane review To assess the diagnostic
et al.52
state
baseline of a pain-free
transition to LBP from a
Literature review, data
necessarily first time.
Inception – 2012,
intermittent symptoms, not
two independent authors
associated with either
(prognosis)
2. Heterogeneity of studies
to be recurrent but have
appraisal performed by
SPORTDiscus, Cochrane
first-time LBP or
Level II
Level II
of evidence
level
NHMRC
1. Possible for included patients Level II
of LBP and risk factors
n = 41
analysis
√
extraction and critical
CINAHL,
√
others did not specify.
excluded sciatica/leg pain,
1. Some included studies
estimate of the incidence
Inception – 2012, PubMed, Literature review, data
n = 24
and meta-
2014 Systematic review To provide a current
similar courses
Williams
Taylor et al.
critical appraisal
pain and disability have
Data extraction and
and to investigate whether
third author if required.
lists
disability in patients with acute and persistent LBP,
authors with consensus by
hand-searched reference
course of pain and
(prognosis)
abstracts screened by two
analysis
CINAHL, EMBASE,
et al.27
literature on the clinical
and meta-
2012 Systematic review To systematically review the
√
evaluation greatly.
evaluation √
unlikely to impact economic
economic
Literature review. Title and
methodological quality but
for full
each stage
for sciatica
model
1950–2011 – MEDLINE,
studies and hence variable
n = 12
at least two authors at
(intervention)
2. Large number of included
review,
appraisal performed by
searched reference lists
management strategies
analysis.
effectiveness of different
systematic
n = 270 for 1. Meta-analysis for cost
and considerations
observations
Methodological
economic
√
Number of inclusions
analysis and
√
assessment
bias
extraction and critical
Literature review, data
methods
Statistical Risk and
28 databases, hand-
Inception – 2009,
Data collection process
Costa
Menezes
Search dates and information sources
effectiveness and cost-
To determine clinical
Objective
review, meta-
Lewis et al.50 2011 Systematic
Study design
Continued
TABLE 3.
MUSCULOSKELETAL RAPID REVIEW SERIES: LOW BACK PAIN
25
Cantrill et al.
55
of Radiologists66
Canadian Association
Bussieres et al.54
Not stated
sources
Search dates and information
opinion
References listed, expert
Data collection process
testing
in adults with potentially
2012 Guideline
methodology not published
1. Guideline development
extraction and critical appraisal, expert consensus
MEDLINE InProcess, Cochrane, hand-searched reference lists
recommendations for prescribing short-acting opioids for adult ED patients conditions while attempting
with painful acute or chronic
Literature review with data
2000–2011 – MEDLINE,
To provide evidence-based
recommendations.
1. No higher level
is not stated.
3. Number of included articles
recommendation.
of evidence and strength of
2. Used own system for levels
viewing.
n = 20
Not stated
on CAR website at date of
√
√
for LBP
working group
3. Aimed at chiropractic’s and
appropriate imaging studies
make decisions in regard to
To assist in helping physicians
Prepared by an expert advisory
EMBASE
appropriate use of diagnostic
Not stated
provided by clinicians,
decision making for the imaging for spinal disorders
emergency physicians.
references and reference
primary care providers in
consensus)
2012 Guideline
primary care but not
register, Google, cross
chiropractors and other
expert
separately to paper. 2. Hand-searched from web.
(Delphi)
Cochrane, National research
guidelines to assist
review and
1. Protocol published
assessment, expert consensus
Literature review, quality
MEDLINE (1966-),
diagnostic imaging practice
To develop evidence-based
care settings
report.
‘Summary’ via NGC
2. Only able to access
recommendation.
of evidence and strength of
1. Used own system for levels
website, and Methodology
n = 385+
Not stated
included.
2. Small number of studies
documentation.
1. Nil supporting
and considerations
n=2
Methodological observations
Studies selected
disorders seen in primary
√
√
?
assessment
bias
Risk and
work-related low back
Searched in 2003–2006 –
group technique), pilot
expert consensus (nominal
CINAHL, EMBASE, PEDro
occupational medical care and disability management,
extraction, critical appraisal,
Online, Cochrane, TRIP,
practices for key areas of
To describe evidence-based best 1966–2010 – MEDLINE, EBM Literature review, data
requesting in EDs
appropriate pathology test
To provide guidance on
Objectives
(systematic
2008 Guideline
2011 Guideline
60
ACOEM
2013 Guideline
ACEM and RCPA53
Design
Year
Guideline characteristics
Reference
TABLE 4.
26 K STRUDWICK ET AL.
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
2012 Guideline
DeLitto et al.59
Daffner et al.
2012 Guideline
secondary sources
Colorado Workers’
consensus)
58
searched for primary and
are enforceable under the
expert
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine throughout
by two independent authors with consensus by third author if required, expert group review
treatment matched to LBP subgroup responder categories, treatments that
evidence to influence the
treatments that have
recurrence of LBP and
have evidence to prevent
stated, referenced
critical appraisal performed
searched reference lists
Not specifically
CINAHL, Cochrane, hand-
√
n = 87
recommendations related to
Literature review including
√
literature and make
1966–2010 – MEDLINE,
(Delphi)
To describe peer-reviewed
of suspected spine trauma
extraction and critical
Literature review with data appraisal, expert consensus
MEDLINE
consensus
the diagnosis and evaluation
of radiologic procedures in
To evaluate the appropriateness Date range not stated,
Procedure
Compensation Rules of
reference lists, hand-
Science, Cochrane, BMJ,
the treatment of LBP that
educational guidelines for
review and
n = 103
evidence and at least
1. Used own grading system.
recommendation.
2. Used own strengths of
Guideline Clearinghouse.
1. Published in National
throughout.
recommendations
3. Does not give strength of
System, not Australian.
Workers’ Compensation
2. Based on Colorado
injury.
not all relevant to acute
1. Very extensive guideline but
harms, costs or burdens).
benefits but no significant
moderate benefits (or small
by at least fair-quality throughout
recommended if supported
1. Interventions only
referenced
Not specifically
and considerations
Methodological observations
peer review
√
Studies selected
stated,
√
assessment
bias
Risk and
consensus, multiple levels of
Literature review, expert panel
Data collection process
2006–2012 – PubMed, Web of Literature review, expert panel
(systematic
To provide advisory and
Cochrane and EMBASE
Inception – 2006, MEDLINE,
sources
Search dates and information
Compensation57
2014 Guideline
settings
chronic LBP in primary care
management of acute and
evidence for evaluation and
To present the available
prescribed opioid analgesics
abuse and overdose of
frequency of adverse events,
to address the increasing
Objectives
Workers’
Colorado Division of
algorithm
2007 Guideline and
Chou et al.56
Design
Year
Continued
Reference
TABLE 4.
MUSCULOSKELETAL RAPID REVIEW SERIES: LOW BACK PAIN
27
integration of acute and
pathway to improve the
To report on the development
pathway
2010 Guideline
Staiger et al.68
trauma patients
spinal injuries in blunt
screening for thoracolumbar
recommendations on the
To provide evidence-based
of a multidisciplinary care
2013 Guideline
Sixta et al.67
management in the ED
care and optimise pain
To implement evidence-based
practice guidelines
and care
2011 Guideline
NICS
64
evidence-based clinical
implementation of common
development and
LBP through the
the management of acute
To achieve significant,
behalf of their patients
appraisal, expert consensus
Not described
extraction and critical
searched reference lists
consensus
Literature review, expert panel
appraisal, expert consensus
Literature review with data
2005–2011 – PubMed, hand-
development process
Specific methodology not stated NHMRC guideline
Inception – 2011, PubMed
?
√
√
Not stated
n = 21
n=2
published.
2. Evaluation of pathway not
documentation.
1. No supporting
recommendation.
2. Used own strengths of
Guideline Clearinghouse.
1. Published in National
articles.
2. Small number of included
now rescinded).
NHMRC, 2003 (which is
musculoskeletal pain’ by
management of acute
‘Evidence-based
1. Key messages guided by
is not stated.
3. Number of included articles
recommendation.
2. Used own strengths of
Guideline Clearinghouse.
1. Published in National
Radiologists accessed.
New Zealand College of
LBP imaging referrals on
Royal Australian and
World of Science
judicious decisions regarding
Not stated
development report by
PubMed, TRIP database,
disciplines on how to make
Literature review with critical
abstract. Module
1. Taken from conference
groups, piloted
n = 19
and considerations
Methodological observations
MEDLINE, PreMedline,
√
Studies selected
practitioners from all
√
assessment
bias
Risk and
appraisal, expert writing
Literature review, critical
Data collection process
CINAHL, EMBASE,
Inception – 2012, All EBM,
sources
Search dates and information
undergraduates and medical
To educate medical
chronic LBP and disability
progression from acute to
Objectives
Consortium63
2014 Guideline
2014 Guideline
Design
measurable improvements in
61
Year
Improvement
Michigan Quality
Goergen and Grimm
Reference
TABLE 4. Continued
28 K STRUDWICK ET AL.
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
√, yes; LBP, low back pain.
Institute69
recommendation.
CINAHL, hand-searched
compensation conditions reference lists
of evidence and strength of
MD Consult, eMedicine,
treatment of workers’
is not stated.
4. Number of included articles
report.
website, and Methodology
‘Summary’ via NGC
3. Only able to access
2. Used own system for levels
expert panel
Guideline Clearinghouse.
1. Published in National
Guideline Clearinghouse,
Not stated
recommendation.
2. Used own strengths of
Guideline Clearinghouse.
1. Published in National
for the assessment and
√
n = 11
extraction, critical appraisal,
Literature review, data
appraisal, expert consensus
Literature review with critical
Cochrane Library, National
1993–2014 – MEDLINE,
2009–2014 – PubMed
to recommendations.
by-step decision protocols
To offer evidence-based step-
quality
Industries62
2013 Guideline
syndrome is of the highest
Labor and
To help ensure diagnosis and
Science
CINAHL, EMBASE, Web of
CRD Databases, AMED,
articles
development group
Google, Chartered Society of
non-specific LBP Physiotherapy, Cochrane,
other included 2. Lists level of evidence next
consensus by guideline
group.
1. Generated from Canadian
International Network,
n = 8 ‘seed’
is not stated.
3. Number of included articles
and considerations
Methodological observations
about care of patients with
treatment of cauda equina
Work Loss Data
Studies selected
guidelines +
√
√
assessment
bias
Risk and
extraction, critical appraisal,
Literature review, data
Data collection process
Infobase, NGC Guidelines
1996–2010 – PubMed, CMA
sources
Search dates and information
evidence-informed decisions
To help clinicians make
continuity of care
patients and to ensure
community care for LBP
Objectives
Department of
Washington State
2014 Guideline
2011 Guideline
Practice65
Toward Optimized
Design
Year
Reference
TABLE 4. Continued
MUSCULOSKELETAL RAPID REVIEW SERIES: LOW BACK PAIN
29
30
Imaging & Diagnostic Tests (n = 16)
Initial Assessment (n = 21)
K STRUDWICK ET AL.
Screen and assess for ‘red flags’35, 38, 40, 41, 43-45, 49, 52, 54, 56, 57, 60, 62-65, 69 • Neurological signs: • loss of bladder/bowel function (urinary retention, incontinence, absent anal sphincter tone, patulous anus, reduced/absent bulbocavernosus reflex), sexual dysfunction, saddle anaesthesia. • bilateral numbness or weakness in the lower limbs, gait disturbance or ataxia. • unilateral multiple nerve root distribution of numbness and weakness. • Risk factors or signs of infection, systemic disease or malignancy: persistent fever, night sweats, rash, abnormal laboratory exams, intravenous drug use, recent bacterial infection, immunocompromised, history of malignancy or unexplained weight loss, nocturnal pain, 50 years of age, non-mechanical pain. • History of trauma with any focal spinal tenderness on palpation, contusion or abrasion, altered consciousness or distracting injury. • Medication effects (i.e. corticosteroid or anticoagulant use). • Persistent or intractable pain not responding to appropriate treatment.
Cauda equina and cord injury Fracture Cancer Infection Systemic disease AAA Failed surgical fusion
Identify ‘yellow flags’46, 49, 56, 57, 59, 63, 65, 68 • E.g. past history of LBP, fear of re-injury, depression / history of mental health issues, social and emotional stresses, low job satisfaction.
Psychosocial risk factors to predict prognosis
Exclude serious conditions
Imaging only indicated in trauma or red flags 41, 46, 49, 54, 56-58, 60-63, 66, 67, 69 • X-ray indicated in suspected vertebral compression fracture. • MRI indicated in presence of neurological abnormalities or suspected malignancy. • CT indicated in known high-velocity trauma, poor visualization of vertebral fracture on x-ray, or if MRI contraindicated. Pathology tests not routinely recommended unless suspected malignancy, infection, or requiring admission.41, 53, 56, 63, 65
Referrals and Follow-up (n = 14)
Treatment (n = 19)
Diagnosis 41, 46, 48, 54, 56, 57, 59, 65 • consider grouping patients into either non-specific LBP, back pain potentially with associated radiculopathy or spinal stenosis, or back pain potentially associated with another specific spinal cause. • do not provide a definitive cause for initial episodes of LBP. Pain relief is an important aspect of ED management of LBP • Pharmacological management 33, 34, 36, 37, 41, 50, 55-58, 60, 63-65, 69 • First-line analgesics should include paracetamol or ibuprofen (with consideration of their side-effect profiles in relation to the patient and their adequacy in relieving pain). • Avoid the use of opioids unless in some cases with severe pain; if prescribed, short-acting doses, for a limited duration, with consideration of the risk for misuse and abuse. • Non-pharmacological management 39, 41, 49, 56, 57, 59, 60, 63-65, 69 • Education and reassurance: good prognosis, avoid bed rest, advice for “self care”, stay active and continue with normal activities; return to ED if ‘red flags’ arise. • Heat and/or cold packs, according to availability and patient preference. • Exercise recommendations: increase physical activity with limited focus on specific exercise prescription.
Referrals 27, 41, 42, 50, 51, 56, 57, 59, 63-65, 68, 69 • GP: Patients should be encouraged to follow-up with their GP for non-specific LBP and non-serious conditions. • Specialist: Recommended in the presence of serious pathology or red flags. • Physiotherapy: Those patients unlikely to improve with aforementioned pain relief strategies may benefit from ongoing non-pharmacological treatments with a Physiotherapist. Patients with ‘yellow flags’ 46, 56, 57, 60, 63 • May benefit from early referral to psychology if psychosocial risk factors are present. • Also consider referral to physiotherapy or other allied health. Chronic LBP 56, 63, 65, 68 • Refer for community health involvement or referral to a multidisciplinary pain management team. Return to Work 57, 60, 63, 65, 69 • An early return to work, even if on modified duties, promotes better outcomes for patients and is associated with less disability.
Figure 2. Existing evidence for LBP across the clinical cycle of care in ED (n = 38). © 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
31
MUSCULOSKELETAL RAPID REVIEW SERIES: LOW BACK PAIN
following statement, ‘Don’t perform imaging for patients with non-specific acute low back pain and no indicators of a serious cause for low back pain’.17 Convincing evidence to support this recommendation includes the inconsistent correlation between findings on imaging and patientreported symptoms,70 the lack of association with improved outcomes22 and the poorer subjective sense of well-being reported by patients who receive imaging.71 Furthermore, in the absence of neurological deficits, suspected malignancy, infection or trauma, imaging is not necessary for effective management56,72 and it may increase the likelihood of unnecessary surgery and inefficacious costly interventions.73 One reviewed article recommended a number of pathology tests;53 however, it should be noted that these are only indicated to exclude red flags, and it should not be included in the routine investigation and management of LBP in ED. It is likely that the overuse of imaging and pathology testing is driven by the pressure to exclude serious pathology, to make an accurate diagnosis and to fulfil patient expectations. Although understandable, the benefits of avoiding unnecessary diagnostic testing are clear, and clinicians must be encouraged to comply with evidence-based practice.
Opioids The prescription of opioids is currently very topical due to the dramatic increase in use, the significant variation in opioid-prescribing patterns in ED, the increase in opioidrelated harms such as hospitalisations and deaths due to accidental poisoning and the corresponding costs to the Australian government.74,75 Analysis of opioid-prescribing patterns in EDs suggest an increase in the use of opioids in place of simple analgesics,20,74 an increasing trend of opioids prescribing on discharge from EDs21 and significant variations between clinicians in prescribing opioids specifically for LBP in ED.76 The evidence in this rapid review clearly supports a reduction in the use of opioids, with some articles recommending reserving opioid use for
severe pain, or recommended against opioid use due to questionable efficacy and increased adverse events.50,55–57,60,63–65 Although early prescription of opioids in this setting may reduce pain severity more rapidly, research shows that this is associated with longer term opioid use, increased costs and increased risk of adverse events.23 For this reason, opioid prescription in ED must be reserved for the most severe cases of LBP, where simple analgesics have been insufficient.
Psychosocial factors In the past few decades, psychosocial factors known as ‘yellow flags’ have emerged as the most important consideration to identify those at risk of developing chronic pain.77,78 This view was supported by the reviewed articles, which promoted psychosocial screening during assessment. Disappointingly, there was little suggestion of what action should be taken when these factors are identified in the acute setting and some might argue that as these factors do not pose an immediate threat to well-being, they are not a priority for management in the ED. It is acknowledged that ED clinicians are often under significant time pressure, and psychosocial factors can be complex and can take some time to properly assess and understand. However, given the known personal, societal and economic burden of chronic LBP1 and the potential for early intervention to reduce this burden,77–79 proactive strategies should be encouraged in the ED. In the absence of clear evidence for the management of ‘yellow flags’ in the ED, the authors recommend that clinicians make use of readily available, quick, easy and reliable psychosocial screening tools, such as the Örebro Musculoskeletal Pain Screening Questionnaire80 or the STarT Back Tool,79 to identify patients at high risk for a poor recovery and to aid in the initial decision making for referrals and follow up. While in the ED, high-risk patients should be given appropriate reassurance, education on simple self-management strategies and
encouragement to resume normal activity. These patients should then be referred on for early psychological intervention and/or active physiotherapy management where possible,77,78 coordinated with their regular GP.
Early return to work Evidence from the rapid review supports that an early return to work for patients with LBP, even if on modified duties, promotes better outcomes for patients and is associated with less disability. Careful consideration should be made to the issuing of medical certificates, as there is evidence to suggest that medical certificates recommending a complete absence from work creates major challenges later in terms of return to work, labour force productivity, the viability of the compensation system and long-term social and economic development.81 Although it may not be the ED’s responsibility to ensure that systems exist in the work place to facilitate a return to work, it is the ED’s role to refer patients appropriately for early co-ordinated care in the community so that a return to work plan is enacted and extended leave is avoided.82 Evidence suggests there is significant variability in duration of work absence in people with LBP who eventually do return to work, ranging from 5–61 days, which further highlights the importance of early community follow up in order to capture the higher risk patients.83 It is also essential to commence patient education on return to work options and outline the health consequences of remaining off work, which include the adverse impacts on mental and physical health, high social and economic costs and possible permanent work disability.
Limitations As described in the corresponding methodology paper,31 there are limitations with conducting a rapid review. Strict inclusion and exclusion criteria were used in order to curtail the duration of the review process, which may have introduced the risk of bias; however, the limitations in this
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
32
K STRUDWICK ET AL.
instance also serve to provide the best and most recent evidence. For this rapid review on LBP, primary articles of a lower level of evidence were included when the topic was related to red flag conditions in which prospective methodology would be both unsafe and unethical. Similarly, while systematic database searches were undertaken, a systematic and exhaustive handsearch was not, which may mean that some relevant articles were not included.
aspects of the work. AB contributed to the conception and design of the work, drafting and revising, final approval of the version to be published and agreement to be accountable for all aspects of the work.
Competing interests
This rapid review serves to provide a summary of the most recent and highest quality evidence supporting best practice for the assessment, use of diagnostic testing, pharmacological and non-pharmacological management and discharge considerations and advice for patients who present to ED with LBP. There is abundant and strong evidence supporting the exclusion of serious pathology by screening for ‘red flags’, more targeted use of imaging and pharmacological management, the identification of psychosocial risk factors from ‘yellow flags’ with associated appropriate discharge planning and promoting an early return to work and functioning following the ED visit. LBP is a common presentation to all EDs and clinicians should aim to adhere to the evidence base and best practice management presented in this review in order to improve patient outcomes and utilise resources more effectively.
References
2.
3.
4.
5.
6.
Acknowledgements Funding by the Emergency Medicine Foundation assisted with the completion of these rapid reviews. The research team acknowledge the contribution of Mr Joseph Danicic.
7.
Author contributions KS, MM, MM-K and TR contributed to the conception and design of the work, acquisition, analysis and interpretation of data for the work, drafting and revising, final approval of the version to be published and agreement to be accountable for all
10.
AB is a section editor for Emergency Medicine Australasia.
1.
Conclusion
9.
8.
Hoy D, March L, Brooks P et al. The global burden of low back pain: estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014; 73: 968–74. Walker BF, Muller R, Grant WD. Low back pain in Australian adults. Prevalence and associated disability. J. Manipulative Physiol. Ther. 2004; 27: 238–44. Australian Institute of Health and Welfare. Musculoskeletal Fact Sheet: Back Problems. Arthritis series no. 21. Cat. no. PHE 185. Canberra: Australian Institute of Health and Welfare, 2015. Australian Institute of Health and Welfare. How Much Is Spent on Back Problems? 2015. [Cited 30 Nov 2016.] Available from URL: http:// www.aihw.gov.au/back-problems/ expenditure/2016 Lovegrove MT, Jelinek GA, Gibson NP, Jacobs IG. Analysis of 22,655 presentations with back pain to Perth emergency departments over five years. Int. J. Emerg. Med. 2011; 4: 1–6. McCaughey EJ, Li L, Georgiou A, Golding MH, Westbrook JI. Imaging for patients presenting to an emergency department with back pain: impact on patient pathway. Emerg. Med. Australas. 2016; 28: 412–8. Luo X, Pietrobon R, Sun SX, Liu GG, Hey L. Estimates and patterns of direct health care expenditures among individuals with back pain in the United States. Spine (Phila Pa 1976) 2004; 29: 79–86. Rizzardo A, Miceli L, Bednarova R, Guadagnin GM, Sbrojavacca R, Della RG. Low-back pain at the
11.
12.
13.
14.
15.
16.
17.
18.
19.
emergency department: still not being managed? Ther. Clin. Risk Manag. 2016; 12: 183–7. Atlas SJ, Deyo RA. Evaluating and managing acute low back pain in the primary care setting. J. Gen. Intern. Med. 2001; 16: 120–31. Australian Acute Musculoskeletal Pain Guidelines Group. EvidenceBased Management of Acute Musculoskeletal Pain – A Guide for Clinicians. Bowen Hills: Australian Academic Press, 2004. D’Arcy Y. Treatment strategies for low back pain relief. Nurse Pract. 2006; 31: 16–25. Stokes B. Four Hour Rule Program Progress and Issues Review. Perth: Government of Western Australia, Department of Health, 2011. Hospitals Principal Committee. Emergency Department Outcome Indicators: Consultation Report (Attachment 1). Australia: Australian Health Ministers’ Advisory Council, 2014. Webster BS, Courtney TK, Huang YH, Matz S, Christiani DC. Physicians’ initial management of acute low back pain versus evidence-based guidelines. J. Gen. Intern. Med. 2005; 20: 1132–5. Williams CM, Maher CG, Hancock MJ et al. Low back pain and best practice care: a survey of general practice physicians. Arch. Intern. Med. 2010; 170: 271–7. McGuirk B, King W, Govind J, Lowry J, Bogduk N. Safety, efficacy, and cost effectiveness of evidence-based guidelines for the management of acute low back pain in primary care. Spine (Phila Pa 1976) 2001; 26: 2615–22. NPS MedicineWise. Choosing Wisely Australia 2016. [Cited 5 Sep 2016.] Available from URL: http:// www.choosingwisely.org.au/home Karel YH, Verkerk K, Endenburg S, Metselaar S, Verhagen AP. Effect of routine diagnostic imaging for patients with musculoskeletal disorders: a metaanalysis. Eur. J. Intern. Med. 2015; 26: 585–95. World Health Organization. Cancer Pain Relief: With a Guide to Opioid Availability. Geneva: World Health Organization, 1996.
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
33
MUSCULOSKELETAL RAPID REVIEW SERIES: LOW BACK PAIN
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
Mafi JN, McCarthy EP, Davis RB, Landon BE. Worsening trends in the management and treatment of back pain. JAMA Intern. Med. 2013; 173: 1573–81. Friedman BW, Chilstrom M, Bijur PE, Gallagher EJ. Diagnostic testing and treatment of low back pain in US emergency departments. A national perspective. Spine (Phila Pa 1976) 2010; 35: E1406. Kendrick D, Fielding K, Bentley E, Kerslake R, Miller P, Pringle M. Radiography of the lumbar spine in primary care patients with low back pain: randomised controlled trial. BMJ 2001; 322: 400–5. Lee SS, Choi Y, Pransky GS. Extent and impact of opioid prescribing for acute occupational low back pain in the emergency department. J. Emerg. Med. 2016; 50: 376–84. Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet 2017; 389: 736–47. Lowthian JA, Curtis AJ, Cameron PA, Stoelwinder JU, Cooke MW, McNeil JJ. Systematic review of trends in emergency department attendances: an Australian perspective. Emerg. Med. J. 2011; 28: 373–7. Van Tulder M, Becker A, Bekkering T et al. Chapter 3 European guidelines for the management of acute nonspecific low back pain in primary care. Eur. Spine J. 2006; 15: s169–s91. Menezes Costa LC, Maher CG, Hancock MJ, McAuley JH, Herbert RD, Costa LOP. The prognosis of acute and persistent lowback pain: a meta-analysis. Can. Med. Assoc. J. 2012; 184: E613–24. Carey TS, Garrett JM, Jackman A, Hadler N. Recurrence and care seeking after acute back pain: results of a long-term follow-up study. Med. Care 1999; 37: 157–64. Henschke N, Maher CG, Refshauge KM et al. Prognosis in patients with recent onset low back pain in Australian primary care: inception cohort study. BMJ 2008; 337: a171. Crawford C, Ryan K, Shipton E. Exploring general practitioner identification and management of psychosocial Yellow Flags in acute low
31.
32.
33.
34.
35.
36.
37.
38.
back pain. NZ Med. J. 2007; 120: U2536. Strudwick K, McPhee M, Bell A, Martin-Khan M, Russell T. Review article: Methodology for the ‘rapid review’ series on musculoskeletal injuries in the emergency department. Emerg. Med. Australas. 2018; 30: 13–7. National Health and Medical Research Council. NHMRC Additional Levels of Evidence and Grades for Recommendations for Developers of Guidelines. 2009. [Cited 23 Feb 2015.] Available from URL: https:// www.nhmrc.gov.au/_files_nhmrc/file/ guidelines/developers/nhmrc_levels_gr ades_evidence_120423.pdf Balakrishnamoorthy R, Horgan I, Perez S, Steele MC, Keijzers GB. Does a single dose of intravenous dexamethasone reduce symptoms in emergency department patients with low back pain and RAdiculopathy (SEBRA)? A double-blind randomised controlled trial. Emerg. Med. J. 2015; 32: 525–30. Behrbalk E, Halpern P, Boszczyk BM et al. Anxiolytic medication as an adjunct to morphine analgesia for acute low back pain management in the emergency department: a prospective randomized trial. Spine (Phila Pa 1976) 2014; 39: 17–22. Dugas AF, Lucas JM, Edlow JA. Diagnosis of spinal cord compression in nontrauma patients in the emergency department. Acad. Emerg. Med. 2011; 18: 719–25. Eken C, Serinken M, Elicabuk H, Uyanik E, Erdal M. Intravenous paracetamol versus dexketoprofen versus morphine in acute mechanical low back pain in the emergency department: a randomised double-blind controlled trial. Emerg. Med. J. 2014; 31: 177–81. Garra G, Singer AJ, Leno R et al. Heat or cold packs for neck and back strain: a randomized controlled trial of efficacy. Acad. Emerg. Med. 2010; 17: 484–9. Jalloh I, Minhas P. Delays in the treatment of cauda equina syndrome due to its variable clinical features in patients presenting to the emergency department. Emerg. Med. J. 2007; 24: 33–4.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
Lau PM, Chow DH, Pope MH. Early physiotherapy intervention in an accident and emergency department reduces pain and improves satisfaction for patients with acute low back pain: a randomised trial. Aust. J. Physiother. 2008; 54: 243–9. Thiruganasambandamoorthy V, Turko E, Ansell D, Vaidyanathan A, Wells GA, Stiell IG. Risk factors for serious underlying pathology in adult emergency department nontraumatic low back pain patients. J. Emerg. Med. 2014; 47: 1–11. Borczuk P. An evidence-based approach to the evaluation and treatment of low back pain in the emergency department. Emerg. Med. Pract. 2013; 15: 1–23. Chau AMT, Xu LL, Pelzer NR, Gragnaniello C. Timing of surgical intervention in cauda equina syndrome: a systematic critical review. World Neurosurg. 2014; 81: 640–50. Downie A, Williams CM, Henschke N et al. Red flags to screen for malignancy and fracture in patients with low back pain: systematic review. BMJ 2013; 347: f7095. Henschke N, Maher CG, Ostelo RW, de Vet HC, Macaskill P, Irwig L. Red flags to screen for malignancy in patients with low-back pain. Cochrane Database Syst. Rev. 2013: CD008686. Henschke N, Maher CG, Refshauge KM. A systematic review identifies five ‘red flags’ to screen for vertebral fracture in patients with low back pain. J. Clin. Epidemiol. 2008; 61: 110–8.e1. Taylor JB, Goode AP, George SZ, Cook CE. Incidence and risk factors for first-time incident low back pain: a systematic review and metaanalysis. Spine J. 2014; 14: 2299–319. Jenkins HJ, Hancock MJ, French SD, Maher CG, Engel RM, Magnussen JS. Effectiveness of interventions designed to reduce the use of imaging for low-back pain: a systematic review. Can. Med. Assoc. J. 2015; 187: 401–8. Hopayian K, Notley C. A systematic review of low back pain and sciatica patients’ expectations and
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
34
49.
50.
51.
52.
53.
54.
55.
56.
57.
K STRUDWICK ET AL.
experiences of health care. Spine J. 2014; 14: 1769–80. Koes BW, van Tulder M, Lin CWC, Macedo LG, McAuley J, Maher C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur. Spine J. 2010; 19: 1–20. Lewis R, Williams N, Matar H et al. The clinical effectiveness and cost-effectiveness of management strategies for sciatica: systematic review and economic model. Health Technol. Assess. 2011; 15: 1–578. Kumar S, Beaton K, Hughes T. The effectiveness of massage therapy for the treatment of nonspecific low back pain: a systematic review of systematic reviews. Int. J. Gen. Med. 2013; 6: 733–41. Williams CM, Henschke N, Maher CG et al. Red flags to screen for vertebral fracture in patients presenting with low-back pain. Cochrane Database Syst. Rev. 2013: CD008643. ACEM and the Royal College of Pathologists of Australasia. Guideline on Pathology Testing in the Emergency Department. 2013. [Cited 4 Mar 2015.] Available from URL: http://www.acem.org.au/standards-pub lications/policies-guidelines.aspx Bussieres AE, Taylor JA, Peterson C. Diagnostic imaging practice guidelines for musculoskeletal complaints in adults-an evidence-based approach-part 3: spinal disorders. J. Manipulative Physiol. Ther. 2008; 31: 33–88. Cantrill SV, Brown MD, Carlisle RJ et al. Clinical policy: critical issues in the prescribing of opioids for adult patients in the emergency department. Ann. Emerg. Med. 2012; 60: 499–525. Chou R, Qaseem A, Snow V et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann. Intern. Med. 2007; 147: 478–91. Colorado Division of Workers’ Compensation. Guideline Summary: Low Back Pain Medical Treatment Guidelines. Denver, CO: Colorado Division of Workers’ Compensation, 2014.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
Daffner R, Weissman B, Wippold FI et al. ACR Appropriateness Criteria: Suspected Spine Trauma. Reston, VA: American College of Radiology, 2012. DeLitto A, George SZ, Van Dillen L et al. Low back pain clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2012; 42: A1–A57. American College of Occupational and Environmental Medicine (ACOEM). Low back disorders. 2011. [Cited 8 Apr 2015.] Available from URL: http://guidelines.gov/content.aspx? f=rss&id=38438 Goergen S, Grimm J. Educational Modules for Appropriate Imaging Referrals: Point of Care Tools for the Emergency Department. Sydney: The Royal Australian and New Zealand College of Radiologists, 2014. Washington State Department of Labor and Industries. WorkRelated Acute Cauda Equina Syndrome (CES) Diagnosis and Treatment. Olympia, WA: Washington State Department of Labor and Industries, 2014. Michigan Quality Improvement Consortium. Management of Acute Low Back Pain in Adults. Southfield, MI: Institute for Clinical Systems Improvement, 2014. National Institute of Clinical Studies. Emergency Care Acute Pain Management Manual. Canberra: National Health and Medical Research Council, 2011. Toward Optimized Practice. Guideline for the Evidence-Informed Primary Care Management of Low Back Pain, 2nd edn. Alberta, Canada: Toward Optimized Practice, 2011. Canadian Association of Radiologists. CAR Diagnostic Imaging Referral Guidelines. 2012. [Cited 12 May 2015.] Available from URL: http://www.car.ca/uploads/ standards%20guidelines/car-referral guidelines-c-en_20120918.pdf Sixta S, Moore FO, Ditillo MF et al. Screening for thoracolumbar
68.
69.
70.
71.
72.
73.
74.
75.
76.
spinal injuries in blunt trauma: an Eastern Association for the Surgery of Trauma practice management guideline. J. Trauma Acute Care Surg. 2012; 73: S326–32. Staiger PK, Serlachius A, Macfarlane S, Anderson S, Chan T, Young G. Improving the coordination of care for low back pain patients by creating better links between acute and community services. Aust. Health Rev. 2010; 34: 139–43. Work Loss Data Institute. Guideline Summary: Low Back – Lumbar & Thoracic (Acute & Chronic). 2013. [Cited 8 Apr 2015.] Available from URL: http://guideline. gov/content.aspx?f=rss&id=47586 van Tulder MW, Assendelft WJ, Koes BW, Bouter LM. Spinal radiographic findings and nonspecific low back pain: a systematic review of observational studies. Spine (Phila Pa 1976) 1997; 22: 427–34. Ash L, Modic M, Obuchowski N, Ross J, Brant-Zawadzki M, Grooff P. Effects of diagnostic information, per se, on patient outcomes in acute radiculopathy and low back pain. Am. J. Neuroradiol. 2008; 29: 1098–103. Chou R, Fu R, Carrino JA, Deyo RA. Imaging strategies for low-back pain: systematic review and meta-analysis. Lancet 2009; 373: 463–72. Shreibati JB, Baker LC. The relationship between low back magnetic resonance imaging, surgery, and spending: impact of physician self-referral status. Health Serv. Res. 2011; 46: 1362–81. Blanch B, Pearson SA, Haber PS. An overview of the patterns of prescription opioid use, costs and related harms in Australia. Br. J. Clin. Pharmacol. 2014; 78: 1159–66. Smulowitz PB, Cary C, Boyle KL, Novack V, Jagminas L. Variation in opioid prescribing patterns between ED providers. Intern. Emerg. Med. 2016; 11: 1–4. Tamayo-Sarver JH, Dawson NV, Cydulka RK, Wigton RS, Baker DW. Variability in emergency physician decision making about prescribing opioid analgesics. Ann. Emerg. Med. 2004; 43: 483–93.
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
35
MUSCULOSKELETAL RAPID REVIEW SERIES: LOW BACK PAIN
77.
78.
79.
Nicholas MK, Linton SJ, Watson PJ, Main CJ. Early identification and management of psychological risk factors (‘yellow flags’) in patients with low back pain: a reappraisal. Phys. Ther. 2011; 91: 737–53. Nicholas MK. Preventing disabling chronic pain by engaging psychologists in the acute phase. InPsych 2016; 38: 12–3. Hill JC, Whitehurst DG, Lewis M et al. Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial. Lancet 2011; 378: 1560–71.
80.
81.
82.
83.
Linton SJ, Nicholas M, MacDonald S. Development of a short form of the Örebro musculoskeletal pain screening questionnaire. Spine (Phila Pa 1976) 2011; 36: 1891–5. Collie A, Ruseckaite R, Brijnath B, Kosny AA, Mazza D. Sickness certification of workers compensation claimants by general practitioners in Victoria, 2003–2010. Med. J. Aust. 2013; 199: 480–3. Fenner P. Returning to work after an injury. Aust. Fam. Physician 2013; 42: 182–5. Wynne-Jones G, Cowen J, Jordan JL et al. Absence from work and return to work in people with
back pain: a systematic review and meta-analysis. Occup. Environ. Med. 2014; 71: 448–56.
Supporting information Additional supporting information may be found in the online version of this article at the publisher’s web site: Appendix S1. Specific search terms for each database. Appendix S2. Summary of the evidence across the clinical cycle of care for LBP.
© 2017 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine