Journal of Human Hypertension (2004) 18, 187–192 & 2004 Nature Publishing Group All rights reserved 0950-9240/04 $25.00 www.nature.com/jhh
ORIGINAL ARTICLE
Blood pressure in acute intracerebral haemorrhage AHG Rasool1, ARA Rahman2, SR Choudhury3 and RB Singh4 1
Department of Pharmacology, School of Medical Sciences, Universiti Sains Malaysia, Malaysia; 2Advanced Medical and Dental Institute, Universiti Sains Malaysia, Malaysia; 3Department of Community Medicine, School of Medical Sciences, Universiti Sains Malaysia, Malaysia; 4Preventive Cardiology Medical Hospital and Research Centre, Moradabad, India
Stroke is one of the leading causes of death worldwide, and spontaneous bleeding into the brain parenchyma, intracerebral haemorrhage (ICH), is a stroke subtype associated with high morbidity and mortality. Overall, it comprises about 15% of all stroke in Caucasians, this figure being much higher in Asians and black people. Blood pressure (BP) appears to play an important role in this disease. We have reviewed available literature on the relationship of BP to the occurrence of primary and secondary ICH, the association of BP levels measured early after stroke with prognosis and complications, and evidence about the effects of early BP lowering treat-
ments on post-stroke outcomes. BP appears to be an important risk factor for primary and secondary ICH. In addition, high BP early after ICH may be detrimental to outcome, possibly contributing to complications such as rebleeding and haematoma enlargement. Few data are available about the effects of early lowering of BP on outcome after ICH with no reliable trial yet conducted. Proper randomised trials are required to establish the effect of early lowering of BP on outcome after ICH. Journal of Human Hypertension (2004) 18, 187–192. doi:10.1038/sj.jhh.1001647
Keywords: blood pressure; intracerebral haemorrhage
Introduction Stroke is one of the leading causes of death worldwide. Intracerebral haemorrhage (ICH) is a severe form of stroke subtype, more likely to result in death or major disability than cerebral infarction or subarachnoid haemorrhage.1,2 Nontraumatic ICH is defined as spontaneous bleeding into parenchyma of the brain that may extend into the ventricles and, in rare cases, the subarachnoid space.3 ICH is reported to occur more than twice as frequently as subarachnoid haemorrhage.1 The worldwide incidence of ICH ranges from 10 to 20 cases per 100 000 population3 and increases with age. Overall, ICH comprises about 15% of total acute stroke presentations, although there are racial and ethnic differences in incidence, which is reported to be higher in black people3 and Asians,4–8 occurring about 3.5 times more frequently in Taiwanese5 and about twice as frequently in Japanese6,7 compared with Caucasian populations. This is supported by results
Correspondence: Dr AHG Rasool, Department of Pharmacology, School of Medical Sciences, Universiti Sains Malaysia, Kelantan 16150, Malaysia. E-mail:
[email protected] Received 10 December 2002; revised 7 July 2003; accepted 25 August 2003
from 14 cohorts from the People’s Republic of China and Japan reporting 45% of all strokes being of the haemorrhagic subtype.9 Risk factors for ICH include elevated arterial blood pressure (BP), anticoagulant use, haematological disorders, heavy alcohol use, cerebral amyloid angiopathy and vascular abnormalities such as aneurysms and arteriovenous malformations. However, it has been reported that primary ICH due to chronic hypertension or amyloid angiopathy accounted for 78–88% of ICH cases3 and another study estimated that about 45–65% nonlobar ICH would be prevented if the effects of hypertension were eliminated.10 Case fatality rate at 1 month is high for ICH, varying between 28 and 52%,2,4,8,11–15 with most deaths occurring within the first few days after the onset of symptoms.16 Factors commonly reported to be associated with poor outcome include large haemorrhage size,13,15,17–19 reduced level of consciousness on admission,14 low Glasgow Coma Scale score,13,15,18,19 initial elevated BP,12,14,17 intraventricular extension15,18 and older age.20,21 To date, no acute intervention, whether medical or surgical, has been conclusively shown to benefit patients with ICH.11 The lack of proven medical or surgical treatment for ICH leads to great variation among physicians concerning both surgical and
Blood pressure in intracerebral haemorrhage AHG Rasool et al 188
medical therapy. Although surgical extraction of haematoma is frequently performed, there is no proven benefit for surgery.22 The guidelines for the management of acute ICH published by the Special Writing Group of the Stroke Council, American Heart Association11 acknowledge the absence of systematic overviews and randomised interventional trials. It, however, recommended treatment of hypertension as the most effective means to prevent primary ICH and its associated morbidity and mortality.
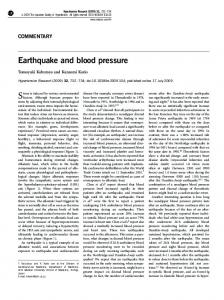
BP and the risk of primary and secondary ICH Many studies have identified hypertension as a major risk factor for the development of primary7,9,23 and recurrent24 ICH. The strength of association between BP and haemorrhagic stroke appears to be greater than that observed for ischaemic stroke. A study on 17 cohorts from the People’s Republic of China and Japan9 involving 115 757 participants showed a significantly stronger association of usual diastolic BP with haemorrhagic stroke than with nonhaemorrhagic stroke, and the odds ratio for 5 mmHg lower BP was 0.54 [95% CI, 0.50–0.58] vs 0.61 [95% CI, 0.57–0.66] for haemorrhagic and ischaemic stroke, respectively (Figure 1). The Systolic Hypertension in the Elderly Program (SHEP) Study25 determined the effects, on stroke, of treating isolated systolic hypertension in 4736 elderly patients. Antihypertensive treatment appears to be more protective against haemorrhagic stroke than ischaemic stroke, the relative risk reduction for haemorrhagic stroke being 0.46 (95% CI: 0.21–1.02) compared to 0.63 (95% CI: 0.48–0.82) for ischaemic stroke. Treatment benefits were also reported to appear earlier for haemorrhagic stroke compared to ischaemic stroke, observed within
Relative risk
Non-haemorrhagic stroke (17 studies, 115757 participants, 901 events)
Haemorrhagic stroke (17 studies, 115757 participants, 751 events)
4.00
4.00
2.00
2.00
1.00
1.00
0.50
0.50 0.25
0.25 70
80
90 100 70 80 Approximate mean usual DBP (mm Hg)
90
100
Figure 1 Relative risk of nonhaemorrhagic and haemorrhagic stroke in cohorts from Japan and the People’s Republic of China according to usual diastolic BP (Eastern Stroke and Coronary Heart Disease Collaborative Research Group, 1998). Logistic regression analyses showed a stronger association of usual diastolic BP with haemorrhagic stroke than with nonhaemorrhagic stroke (OR for 5 mmHg decrease 0.54 CI: 0.50–0.58, vs 0.61 CI: 0.57–0.66, P for heterogeneity 0.02). Reprinted with permission from Elsevier Science (The Lancet, 1998; 352: 1801–1807). Journal of Human Hypertension
1 year for haemorrhagic stroke but not until the second year for ischaemic stroke. However, the number of patients with haemorrhagic stroke was only 28. High BP has also been shown to be an important risk factor for the recurrence of ICH.24 In a prospective study of 74 patients with hypertensive brain haemorrhage,24 higher diastolic BP was related to an increased rate of rebleeding. Recurrence rate was calculated to be 10.0% per patient-year among individuals with diastolic BP490 mmHg and o1.5% in those with lower diastolic BP. A retrospective study26 of 51 patients with previous ICH also showed the stroke recurrence rate to be lower in a group with post-stroke BPo80 mmHg compared to those with post-stroke BP 490 mmHg. The recently reported Perindopril Protection Against Recurrent Stroke Study (PROGRESS) investigated the effects of BP lowering with an angiotensin-converting enzyme (ACE) inhibitor-based regimen in patients with a history of cerebrovascular disease.27 Compared with placebo, treatment with the ACE inhibitor, perindopril, with the addition of a diuretic, indapamide, in 58% of subjects, resulted in a significant 28% (95% CI: 17–38) reduction in the occurrence of all stroke. Treatment appeared to offer greater protection against haemorrhagic stroke, reducing risk by 50% (95% CI: 26–67) compared to ischaemic stroke, which reduced risk by 24% (95% CI 10–35). The role of BP in the prognosis and major complications of acute ICH and optimal management of BP in the early stages of acute ICH is still unclear. The following sections aims to review the available literature on these issues.
Association of early post-stroke BP levels with outcome Elevated blood pressure early after stroke occurs in as many as 90% of patients with acute ICH, and often to very high levels. This initial BP after haemorrhage is typically higher than after ischaemic stroke.8,28,29 Frequently, elevated BP levels after stroke decline spontaneously,28,29 although about one-third of patients remain hypertensive on the 10th day.29 The BP after a haemorrhagic stroke may remain elevated for a greater duration of time than following ischaemic stroke. There is corresponding uncertainty about the prognostic implication of high initial BP after acute ICH,12,13,14,17,19,20,30 and the findings of the principal observational studies are summarised in Table 1 (see Figure 2).
Effects of blood pressure lowering in acute ICH There are few data about the effects of lowering BP in acute ICH. An early prospective but nonrando-
Blood pressure in intracerebral haemorrhage AHG Rasool et al 189
Table 1 Observational studies on the relationship between initial BP to outcome of ICH Study
Number of ICH patients
Terayama et al17
1701
Fogelholm et al14
282
Nath et al19 Dandapani et al12
244 87
Carlberg et al30
85
Tuhrim et al13 Lisk et al20
82 75
Outcome details
Increased admission MAP related to increased mortality in putaminal and thalamic haemorrhages, most common sites for ICH. Patients who died had significantly higher MAP Admission level of consciousness, followed by maximum MAP in the first 24 h most important predictors of survival at 28 days. Survival rates decreased progressively with increasing quartiles of MAP (Figure 2). Unconscious/comatose patients, patients who died had significantly higher MAP Admission BP not statistically correlated with outcome Improved mortality and morbidity at 30 days with initial MAP p145 mmHg compared with those having MAP >145 mmHg. Improved outcomes in those whose BP better controlled using BP lowering regimens to MAP p 125 mmHg. Elevated admission MAP significantly associated with 30-day case fatality in patients with impaired consciousness. However, BP not significantly different between surviving and deceased patients BP one of the factors statistically associated with outcome, measured as fatality at 30 days No significant differences in baseline SBP or DBP between patients with bad and good outcome at 30 days/discharge, although patients with good outcome had slightly lower BP
MAP is mean arterial pressure.
Proportion surviving
1.00
0.75
0.50
0.25
1.MAP Q. 2.MAP Q. 3.MAP Q. 4.MAP Q.
0.00 0
7
14 Days of onset
21
28
Figure 2 Twenty-eight-day survival belonging to four quartlies of MAP (cutoff values 118, 132 and 145 mmHg). Survival rates decreased progressively with increasing quartiles of MAP. The differences between the first three quartiles and the fourth quartile are statistically highly significant (log-rank test Po 0.0001 to P ¼ 0.0010). Q indicates quartile. (1) MAP Q: o118 mmHg. (2) MAP Q: o132 mmHg. (3) MAP Q: o145 mmHg, (4) MAP Q: 4145 mmHg. Reprinted with permission from Stroke 1997; 28: 1396–1400 (Fogelholm et al14: Prognostic value and determinants of first day MAP in spontaneous supratentorial ICH).
mised study included 167 patients with hypertensive intracranial haemorrhage, divided into three groups that were untreated, inadequately treated or adequately treated with the antihypertensive agent reserpine.31 A poor outcome was most frequent in the group that did not receive treatment, followed by the inadequately treated group, with the best results in the adequately treated group. However, interpretation of the results is difficult due to the nonrandomised, unblinded study methodology, and the fact that criteria for classifying patients into adequate and unadequately treated groups were not clearly specified. More recently, a small randomised
controlled trial32 investigated the effects of oral nimodipine administered within 6 h of acute stroke in 261 patients with ischaemic stroke and in 35 patients with ICH. Overall, no significant effect of nimodipine was identified (relative risk of 1.2; 95% CI: 0.9–1.6), with subgroup analysis identifying relative risks for ischaemic and haemorrhagic stroke subtypes of 1.4 (95% CI of 1.0–2.1) and 1.0 (95% CI of 0.6–1.7), respectively. The Special Writing Group of the Stroke Council, American Heart Association11 suggests that, for patients with ICH, BP levels be maintained below a mean arterial pressure of 130 mmHg in the presence of a history of hypertension, and a mean arterial pressure 4110 mmHg should be avoided immediately after surgery. Pressors should be given for systolic arterial BP that falls below 90 mmHg, and patients with elevated intracranial pressure (ICP) on ICP monitors should have their cerebral perfusion pressure kept to 470 mmHg. It should be noted however that these recommendations are not based on large interventional trials of BP intervention in acute stroke.
Blood pressure, haematoma size and cerebral oedema after ICH One possible explanation of the early progression of neurological deficit in patients with ICH is ongoing bleeding and enlargement of the haematoma. Early growth of ICH is frequently observed, being reported to occur between 20 and 38% of patients within 120 h of symptom onset, although mostly within the first 24 h after onset.33,34 These proportions almost certainly underestimate the true frequency of haematoma growth as both studies excluded patients who died before, or were too moribund to undergo repeat CT scanning. Haematoma enlargement was Journal of Human Hypertension
Blood pressure in intracerebral haemorrhage AHG Rasool et al 190
associated with neurological deterioration in both studies, and was identified as a significant cause of intracerebral haemorrhage-related death in one of the studies.34 Based on several relatively small observational studies, it has been suggested that elevated initial BP in ICH is associated with enlargement of haematoma in the period following admission.35–37 Persistent and/or marked elevation of BP has been observed in patients who have been noted to have persistent bleeding or haematoma enlargement on serial CT scans enlargement. Persistent uncontrolled hypertension in acute ICH may increase the risk of ongoing and/or recurrent bleeding from ruptured small arteries and arterioles, leading to haematoma enlargement and clinical deterioration.36,37 However, the possibility that larger haematomas result in elevated BPs in an attempt to maintain cerebral blood flow in the presence of raised ICP cannot be excluded by these data. A prospective observational study of 103 patients to determine how frequently early growth of ICH occurs failed to identify any significant predictors for haemorrhage growth, including BP. However, early treatment of moderately or severely elevated blood pressure in the majority of the study patients may have obscured any such relationship between elevated blood pressure and haemorrhage growth.33 Untreated severe hypertension may also cause excessive perfusion pressure, which may promote or worsen existing oedema, increase ICP and ischaemia, and cause failure of cerebral perfusion.12,38,39 Worsening cerebral oedema has been implicated in neurological deterioration that occurs within 24– 48 h after the onset of haemorrhage.40 Late deterioration can also be associated with progression of oedema during the second and third weeks after the onset.41
Considerations in lowering BP early after ICH Despite the potential, but still unproven, benefits of blood pressure lowering following acute ICH, there remain some concerns about the potential adverse effects of acute lowering of blood pressure. It was previously thought that the area surrounding the ICH may behave like an area of cerebral ischaemia due to the mass effect of the haematoma. Rapid blood pressure reduction could theoretically promote hypoperfusion and further ischaemia in the brain tissue surrounding the haematoma.42,43 However, two recent prospective but small clinical studies44,45 were unable to detect consistent evidence of an ischaemic tissue penumbra adjacent to the haematoma between 24–48 h after ICH. One study45 of nine patients using magnetic resonance spectroscopic imaging had showed that only in the patient with the largest haematoma was there radiological evidence of ischaemia adjacent to the haematoma, although this was not confirmed by the Journal of Human Hypertension
presence of lactate, a metabolic marker of ischaemia. In all their cases, results were compatible with the presence of vasogenic oedema. The other study with six ICH patients and eight controls using positron emission tomography (PET) also found no evidence of an ischaemic penumbra44 as they had previously shown to occur adjacent to cerebral infarction using the same technique.46 However, neither study could exclude the possibility of ischaemia during the first 24 h after ICH. There is also concern that the elevated systemic pressure frequently observed following ICH is required to preserve cerebral blood flow in the presence of disturbed cerebral autoregulation that is believed to occur frequently following acute stroke.47,48 Autoregulation denotes the process whereby global cerebral blood flow is kept constant over a wide range of BP.49 Cerebral autoregulation usually protects against precipitous falls in blood pressure, maintaining cerebral blood flow within normal limits across a wide range of mean arterial pressures between approximately 60 and 150 mmHg.42 When cerebral autoregulation is impaired, cerebral blood flow becomes dependent upon systemic BP. Lowering BP in such circumstances may render the brain susceptible to hypoperfusion. Studies in head trauma patients have shown that a mean arterial pressure (MAP) o80 mmHg is usually associated with loss of cerebral autoregulation and a decline in cerebral perfusion pressure.47,50 However, in chronic hypertension there is reported to be an upward shift in the lower limit at which autoregulation of cerebral blood flow is maintained, although the amount of such a shift is unpredictable.51,52 Three studies have examined autoregulation and cerebral blood flow following acute BP lowering in acute ICH. In a trial of eight patients with small- to medium-sized ICH presenting within 24 h of a stroke, trimethophan was used to produce a gradual decline in BP.53 Cerebral autoregulation was shown to be present and whole brain cerebral blood flow was shown to be preserved after MAP was reduced by 19% from admission pressure to a lower limit of 110 mmHg. In most patients, the lower limit of autoregulation occurred at a level corresponding to approximately 80% of initial post-ICH BP. Therefore, they suggested that blood pressure should be reduced by no more than 20% in the acute phase following an ICH. A larger study of 68 patients presenting with small acute haematomata in the thalamic and putaminal regions measured regional cerebral blood flow following BP reductions induced by trimethaphan or diltiazem, administered to reduce a mean BP of about 20%.54 In patients studied, on average 3 days after onset, cerebral blood flow was found to decrease only after a 20% or greater fall in BP. A further study examined cerebral blood flow in 14 patients with acute supratentorial haemorrhage 6–22 h following the onset of symptoms.55 Pharmacologic reduction of MAP with nicardipine or labetolol by up to about
Blood pressure in intracerebral haemorrhage AHG Rasool et al 191
17% from baseline (MAP 143–119 mmHg) produced no change in global or peri-clot regional cerebral blood flow. Autoregulation was not found to be impaired and there was no evidence of cerebral ischaemia. However, all the above studies were performed in patients with small- or medium-sized haematoma and there are no data on outcome following BP lowering in the presence of large ICHs. None of the studies provide data on ICP or its relationship with cerebral blood flow. Those with large ICH may have increased ICP associated with a secondary rise in systemic BP.12,43 As cerebral arterial perfusion is a function of the difference between systemic arterial pressure and ICP, a fall in systemic BP may compromise cerebral perfusion. This problem may be exacerbated in patients with chronic hypertension.43
Conclusion There appears to be a direct relationship between BP and the risk of primary and secondary ICH. The effect of BP on outcome in the acute phase of stroke is more controversial, but it appears that very high blood pressure may be detrimental to the outcome of acute ICH. Although it had been shown that elevated BP will fall spontaneously in about twothirds of patients with acute stroke, the effect of an earlier modest lowering of BP may be beneficial or crucial in preventing certain complications like rebleeding and haematoma enlargement in acute ICH. Antihypertensive treatment would also be useful to those patients whose BPs do not fall spontaneously over time, as occur in about one-third of patients with acute stroke. There is little reliable evidence about the effects of BP lowering in acute haemorrhagic stroke. We therefore see a strong justification for the need of a large, well-designed and executed randomised trial to determine the safety and efficacy of BP lowering in acute ICH. A trial to explore the effect of BP treatment on the expansion of haematoma will also be useful.
References 1 Broderick J et al. Intracerebral hemorrhage is more than twice as common as subarachnoid haemorrhage. J Neurosurg 1993; 78: 188–191. 2 Anderson CS, Jamrozik KD, Broadhurst RJ, StewartWynne EG. Predicting survival for 1 year among different subtypes of stroke: results from the Perth Community Stroke Group. Stroke 1994; 25: 1935–1944. 3 Qureshi A, Tuhrim S, Broderick J. Medical progress: spontaneous intracerebral hemorrhage. N Eng J Med 2001; 344: 1450–1460. 4 Jaya F et al. Stroke patterns in northeast Malaysia: a hospital based prospective study. Neuroepidemiology 2002; 21: 28–35.
5 Hung T, Chen S. Cerebral hemorrhage in Taiwan. J Formos Med Assoc 1993; 92(Suppl 4): S161–S168. 6 Suzuki K et al. Stroke incidence and case fatality in Finland and in Akita, Japan: a comparative study. Neuroepidemiology 1994; 13: 236–244. 7 Tanaka H et al. Risk factors for cerebral hemorrhage and cerebral infarction in a Japanese rural community. Stroke 1982; 13: 62–73. 8 Ong TZ, Raymond AA. Risk factors for stroke and predictors of one month mortality. Singapore Med J 2002; 43: 517–521. 9 Eastern Stroke and Coronary Heart Disease Collaborative Research Group. Blood pressure, cholesterol, and stroke in eastern Asia. Lancet 1998; 352: 1801–1807. 10 Woo D et al. Genetic and environmental risk factors for intracerebral hemorrhage. Preliminary results of a population based study. Stroke 2002; 33: 1190–1196. 11 Broderick J et al. Guidelines for the management of spontaneous intracerebral hemorrhage: a statement for healthcare professionals from a special writing group of the stroke council, American Heart Association [AHA Scientific Statement]. Stroke 1999; 30: 905–915. 12 Dandapani B et al. Relation between blood pressure and outcome in intracerebral hemorrhage. Stroke 1995; 26: 21–24. 13 Tuhrim S et al. Prediction of intracerebral hemorrhage survival. Ann Neurol 1988; 24: 258–263. 14 Fogelholm R, Avikainen S, Murros K. Prognostic value and determinants of first day mean arterial pressure in spontaneous supratentorial intracerebral hemorrhage. Stroke 1997; 28: 1396–1400. 15 Tuhrim S, Dambrosia J, Price T. Intracerebral hemorrhage: external validation and extension of a model for prediction of 30 day survival. Ann Neurol 1991; 29: 658–663. 16 Broderick J et al. Volume of intracerebral hemorrhage. A powerful and easy to use predictor of 30 day mortality. Stroke 1993; 24: 987–993. 17 Terayama Y, Tanahashi N, Fukuuchi Y, Gotoh F. Prognostic value of admission blood pressure in patients with intracerebral hemorrhage: Keio cooperative stroke study. Stroke 1997; 28: 1185–1188. 18 Portenoy R et al. Intracerebral haemorrhage: a model for the prediction of outcome. J Neurol Neurol Psychiatry 1987; 50: 976–997. 19 Nath F, Nicholls D, Fraser R. Prognosis in intracerebral hemorrhage. Acta Neurochir 1983; 67: 29–35. 20 Lisk D et al. Early presentation of hemispheric intracerebral hemorrhage: prediction of outcome and guidelines for treatment allocation. Neurology 1994; 44: 133–139. 21 Daverat P, Castel J, Dartigues J, Orgogozo J. Death and functional outcome after spontaneous intracerebral hemorrhage. A prospective study of 166 cases using multivariate analysis. Stroke 1991; 22: 1–6. 22 Prasad K, Shrivastava A. Surgery for primary supratentorial intracerebral hemorrhage (Cochrane Review). In: The Cochrane Library, Issue 2. Update Software: Oxford, 2001. 23 Prentice RL et al. Serial blood pressure measurements and cardiovascular disease in a Japanese cohort. Am J Epidemiol 1982; 116: 1–28. 24 Arakawa S et al. Blood pressure control and recurrence of hypertensive brain hemorrhage. Stroke 1998; 29: 1806–1809. Journal of Human Hypertension
Blood pressure in intracerebral haemorrhage AHG Rasool et al 192
25 Perry H et al. Effects of treating isolated systolic hypertension on the risk of developing various types and subtypes of stroke: the Systolic Hypertension in the Elderly Program (SHEP). J Am Med Assoc 2000; 284: 465–471. 26 Irie K, Yamaguchi T, Minematsu K, Omae T. The J-curve phenomenon in stroke recurrence. Stroke 1993; 24: 1844–1849. 27 PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood pressure lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet 2001; 358: 1033–1041. 28 Harper G, Castleden CM, Potter JF. Factors affecting changes in blood pressure after acute stroke. Stroke 1994; 25: 1726–1729. 29 Wallace J, Levy L. Blood pressure after stroke. JAMA 1981; 246: 2177–2180. 30 Carlberg B, Asplund K, Hagg E. The prognostic value of admission blood pressure in patients with acute stroke. Stroke 1993; 24: 1372–1375. 31 Meyer J, Raymond B. Medical treatment of spontaneous intracranial hemorrhage by the use of hypotensive drugs. Neurology 1962; 12: 36–47. 32 Horn J, de Haan R, Vermeulen M, Limburg M. Very early nimodipine use in Stroke (VENUS): a randomized, double blind, placebo-controlled trial. Stroke 2001; 32: 461–465. 33 Brott T et al. Early hemorrhage growth in patients with intracerebral hemorrhage. Stroke 1997; 28: 1–5. 34 Kazui S et al. Enlargement of spontaneous intracerebral hemorrhage: incidence and time course. Stroke 1996; 27: 1783–1787. 35 Kazui S et al. Predisposing factors to enlargement of spontaneous intracerebral hematoma. Stroke 1997; 28: 2370–2375. 36 Chen S, Chen S, Hsu C, Hogan E. Progression of hypertensive intracerebral hemorrhage. Neurology 1989; 39: 1509–1514. 37 Broderick J et al. Ultra early evaluation of intracerebral hemorrhage. J Neurosurg 1990; 72: 195–199. 38 Spence J, Del Maestro R. Hypertension in acute ischemic strokes. Treat Arch Neurol 1985; 42: 1000–1002. 39 Hayashi M. Treatment of systemic hypertension and intracranial hypertension in cases of brain hemorrhage. Stroke 1988; 19: 314–321. 40 Mayer S, Sacco R, Shi T, Mohr J. Neurological deterioration in non-comatose patients with supraten-
Journal of Human Hypertension
41 42 43 44 45
46 47 48 49 50 51 52
53
54 55
torial intracerebral haemorrhage. Neurology 1994; 44: 1379–1384. Zazulia A, Diringer M, Derdyn C, Powers W. Progression of mass effect after interacerebral hemorrhage. Stroke 1999; 30: 1167–1173. Powers W. Acute hypertension after stroke: the scientific basic for treatment decisions. Neurology 1993; 43: 461–467. Lavin P. Management of hypertension in patients with acute stroke. Arch Intern Med 1986; 146: 66–68. Hirano T. No evidence of hypoxic tissue on 18 F-fluoromisonidaole PET after intracerebral hemorrhage. Neurology 1999; 53: 2179–2182. Carhuapoma J et al. Difusion-weighted MRI and proton MR spectroscopic imaging in the study of secondary neuronal injury after intracerebral hemorrhage. Stroke 2000; 31: 726–732. Read S et al. Identifying hypoxic tissue after acute ischemic stroke using PET and 18F-fluoromisonidazole. Neurology 1998; 51: 1617–1621. Bhalla A, Wolfe C, Rudd A. Management of acute physiological parameters after stroke. Q J Med 2001; 94: 167–172. Meyer J et al. Impaired neurogenic cerebrovascular control and dysautoregulation after stroke. Stroke 1973; 4: 169–186. Strandgaard S. Autoregulation of cerebral circulation in hypertension. Acta Neurol Scand 1978; 57 (Suppl 66): S1–S82. Reilly P, Lewis S. Progress in head injury management. J Clin Neurosci 1997; 4: 9–15. Strandgaard S, Olesen J, Skinhoj E. Autoregulation of brain circulation in severe arterial hypertension. BMJ 1973; i: 507–510. Strandgaard S. Autoregulation of cerebral blood flow in hypertensive patients. The modifying influence of prolonged antihypertensive treatment on the tolerance to acute, drug induced hypotension. Circulation 1976; 53: 720–727. Kaneko T, Sawada T, Niimi T. Lower limit of blood pressure in treatment of acute hypertension in intracranial hemorrhage (AHIH). J Cereb Blood Flow Metab 1983; 29(Suppl 1): S51–S52. Kuwata N et al. Dysautoregulation in patients with hypertensive intracerebral hemorrhage. A SPECT study. Neurosurg Rev 1995; 18: 2370–2345. Powers W et al. Autoregulation of cerebral blood flow surrounding acute (6–22 hours) intracerebral hemorrhage. Neurology 2001; 57: 18–24.