researchers who have studied developmental aspects of diabe- tes self-management ..... others to tell me what to do or have my life dictated by my diabe- tes.
Clinical Nursing Research http://cnr.sagepub.com
Developmental Evolution of Expertise in Diabetes Self-Management Barbara Paterson and Sally Thorne Clin Nurs Res 2000; 9; 402 DOI: 10.1177/10547730022158663 The online version of this article can be found at: http://cnr.sagepub.com/cgi/content/abstract/9/4/402
Published by: http://www.sagepublications.com
Additional services and information for Clinical Nursing Research can be found at: Email Alerts: http://cnr.sagepub.com/cgi/alerts Subscriptions: http://cnr.sagepub.com/subscriptions Reprints: http://www.sagepub.com/journalsReprints.nav Permissions: http://www.sagepub.com/journalsPermissions.nav
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
CLINICAL Thorne Paterson, NURSING / DIABETES RESEARCH SELF-MANAGEMENT / November 2000
The following is a description of the findings of a longitudinal exploratory and descriptive research study of 22 persons nominated as expert self-managers of Type 1 diabetes. It entailed an initial interview about previous experiences with self-management, self-recorded taped diaries about self-management decisions for 1 week each, and face-to-face interviews following each weeklong recording of self-management decisions. The study generated a grounded theory about the development of expertise in diabetes self-management. The development of expertise was found to occur as transition through two or more phases, to be individualized, and to involve a complex interplay between social, contextual, and personal factors, including the individual’s developmental age. The research findings challenge the traditional understanding of rebellion in self-management as a manifestation of adolescence, behaviors other than active control as testimony to ineptitude in self-management, metabolic control as the indicator of selfmanagement ability, and the role of others as collaborators in self-management.
Developmental Evolution of Expertise in Diabetes Self-Management BARBARA PATERSON SALLY THORNE University of British Columbia
It is well-known that people who live with a chronic disease for a long time can develop an expertise in the everyday management of their disease (Paterson & Sloan, 1994; Wuest, 1995). Expert self-care arises from individuals’ awareness of their own bodies and what works best for them. It is from an understanding of how experts develop expertise in self-management that Authors’ Note: The researchers gratefully acknowledge funding from British Columbia Health Research Foundation. CLINICAL NURSING RESEARCH, Vol. 9 No. 4, November 2000 402-419 © 2000 Sage Publications, Inc.
402
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
Paterson, Thorne / DIABETES SELF-MANAGEMENT
403
health care professionals can discover means to foster expert self-management in individuals who are newly diagnosed. The purpose of the following article is to describe the developmental evolution of expertise in the self-management of diabetes as it was portrayed in a research study about expert self-management of persons with long-standing Type 1 diabetes.
LITERATURE REVIEW Harper (1991) has criticized researchers for failing to recognize that adaptation to chronic illness, including learning to self-manage the disease, is a developmental process. The few researchers who have studied developmental aspects of diabetes self-management have adopted mainly two approaches: (a) according to the developmental attributes of specific age groups and (b) as a sequential staged process in which a trajectory of self-management is identified. The most common approach to the study of developmental changes in living with a chronic illness is based on the assumption that self-management reflects the developmental characteristics of a specific age, despite the lack of empirical evidence to support a relationship between age and self-management behaviors (Wysocki et al., 1996). There has been some research that has clearly demonstrated that preadolescents, adolescents, and older adults may hold different personal models, including beliefs, attitudes, and emotional responses, about diabetes (Hampson, Glasgow, & Foster, 1995; Standiford, Turner, Allen, Drozda, & McCain, 1997) but the relationship between personal models and self-management behaviors has not been established. Self-management in children has not been a significant topic of study, primarily because the underlying assumption of many researchers is that children simply follow the directives of their parents. There is a much larger body of research about the experience of adolescents. Adolescents are often perceived by researchers as a high-risk group because of their tendency toward self-management neglect (Hentinenen & Kyngas, 1992; Kyngas & Barlow, 1995). Adults are the most common focus of study about self-management in diabetes. Age-related research has contributed to an understanding of the challenges that self-management presents to various ages but it is
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
404
CLINICAL NURSING RESEARCH / November 2000
unclear how age-related parameters contribute to or detract from the development of self-management expertise. The focus of this body of research is group, rather than individual, changes. Individuals are assumed to represent their age group without consideration of the diversity that exists among people of that age (Clay, 1995). The development of expertise in self-management has been presented by many researchers as a developmental trajectory, characterized by sequential phases from the point of diagnosis (see review in Paterson, Thorne, & Dewis, 1998). Ellison and Rayman (1998), for example, report that 17 participants recalled their evolution as experts in terms of three phases, management as rules, management as work, and management as living. Several have theorized that people with diabetes may “tune in” to their bodies, attempting a variety of management strategies over time until they discover what is effective for their unique needs and lifestyle (Ellison & Rayman, 1998; Hernandez, 1991; Jayne, 1993; Nyhlin, 1990; Paterson & Sloan, 1994; Price, 1988) to become expert self-managers. This may take the form of a vigilant awareness as well as reliance on intuition and personal experience to make everyday decisions. Although focusing on the development of expertise in diabetes self-management as a trajectory has enhanced our understanding of the expressive components of living with the disease (Diedricks & Bal, 1997), we know little about how people change in relation to how they perceive and make self-management decisions over time. It is assumed by most authors who have been oriented by a trajectory approach that experience with diabetes is critical to becoming an expert in self-management decision making but they do not consider why some people with long-standing diabetes are unable to sustain effective self-management strategies. This is further complicated by the finding (e.g., Blaum, Velez, Hiss, & Halter, 1997) that some people may actually become less able to sustain good glycemic control over the passage of years. This brief overview of developmental research in diabetes has revealed limitations of both age-related and trajectory approaches to the study of the development of expertise in self-management. Although there is fragmentary evidence of the complexity inherent in developing self-management exper-
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
Paterson, Thorne / DIABETES SELF-MANAGEMENT
405
tise in Type 1 diabetes, considerable gaps in what is known about such processes and how they may be influenced remain.
METHOD The current research was guided by the social psychology theory of symbolic interactionism (Blumer, 1969). We assumed that experts would make self-management decisions in accordance with the meaning that the situation/event had for them, that they would derive this meaning from their interaction with others, and that they interpret the situation according to this meaning (Annells, 1996). For example, we asked participants to record descriptions of self-management decisions they made during the research, including the setting and context, and to reflect on the personal significance that these decisions had for them. DESIGN
The study was an investigation of the self-management decisions by 22 individuals with long-standing (defined as longer than 15 years) Type 1 diabetes, identified as expert self-management decision makers. The research was a grounded theory study in the tradition of Glaser and Strauss (1967) and recent developments by Thorne, Kirkham, and MacDonald-Emes (1997). The design assumes that the insider perspective on the complex process of self-management is accessible through interpretive research methods and that this perspective represents an important contribution to traditional understanding of this phenomenon. SAMPLE
The 22 participants were Caucasian individuals who lived in British Columbia, Canada. The 14 women and 8 men ranged in age from 24 to 81 years (M = 43.3). The duration of their diabetes ranged from 15 to 41 years (M = 30.3). Ten participants resided in rural areas; the remainder lived in urban or suburban communities. Eighteen of the 22 participants had high
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
406
CLINICAL NURSING RESEARCH / November 2000
school or postsecondary education. Eight participants had one or more diabetes-related complication, including nephropathy, retinopathy, atherosclerosis, and neuropathy. As we were interested in testing and refining the concept of expertise in self-management, we selected 11 participants who were nominated by physicians and 11 who nominated themselves as experts in self-management. Each group nominated a patient in their care or themselves according to the definition of successful self-management provided; that is, able to make trustworthy decisions about self-management and to maintain good overall glycemic control. DATA COLLECTION
Participants nominated by five diabetes internists were studied in the 1st year and the remaining participants in the 2nd year of the research. This design permitted the allocation of similar data collection schedules to compare both groups’ self-management decision making according to season and type of activity. For example, 6 participants in both groups recorded their decisions during a vacation. Following an initial interview about his or her past and current experiences in diabetes self-management, each participant was randomly assigned three data collection periods of 1 week each, at least 2 months apart. Spacing data collection periods 2 months apart enabled sufficient seasonal and other variation to provide a varied context to investigate self-management and to chart changes that occurred in self-management over time. Throughout each data collection period, participants audiotaped their daily self-management decisions using a modified “think aloud” (MTA) technique (Fontana & Frey, 1994; Fonteyn & Fisher, 1995). The MTA entailed the use of a handheld tape recorder in which the participants recorded decisions they made every day throughout the 1-week period. The MTA is an inventory of self-management decisions as they occur in the context of the individual’s everyday life in a current, prospective manner (Fonteyn & Fisher, 1995). It provides qualitative data consisting of narrative statements on the decision-making process and its sequence as well as the precipitating situation and outcomes and contextual factors that affect decision making. Transcriptions of MTAs were used as prompts for additional intensive interviews, called post-think-
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
Paterson, Thorne / DIABETES SELF-MANAGEMENT
407
aloud interviews (PTAI), at the conclusion of each data collection period. The primary purpose of the PTAI is to clarify or extend data that the participants provide in the MTA to elicit a comprehensive understanding of the complex, multifactorial reasoning and decision-making processes. In the PTAI, the interviewer repeated the participant’s statements about a particular self-management decision in the MTA to foster the participant’s recall of the situation and then asked detailed questions about it. For example, a participant stated in her MTA, “I took an extra unit of insulin because I was climbing the hill after breakfast and it’s a steep hill.” The interviewer asked questions such as, “Tell me why you took insulin on this occasion. What does the steepness of the hill have to do with how much insulin you take? What are some other ways in which you might respond to such a situation?” Interview questions were also generated from themes that arose in data of other interviews (e.g., when participants indicated that specific household tasks made them particularly vulnerable to hypoglycemic episodes, we explored with other participants whether there were specific household activities that seemed to produce greater changes in blood sugar than others). The participants attended a 2-hour focus group interview at the end of the research with 4 to 7 other participants in the same sample group. During the focus interview, the researchers shared the research findings and asked the participants, “How do the research findings fit with your experience? What surprised you about the research findings? What aspects of the research findings did you find confusing or unclear? What other comments do you have about what we discovered?” The participants’ comments were entered as further data. The participants validated the findings; only two changes were suggested to refine the wording of two categories. DATA ANALYSIS
Analysis of the transcripts was guided by traditional constant comparative analytic (Glaser & Strauss, 1967) techniques. We developed hypotheses as the fieldwork progressed and tested these hypothetical relationships by means of further data collection and analysis in the search for confirming or disconfirming evidence to support or negate the emerging the-
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
408
CLINICAL NURSING RESEARCH / November 2000
ory (Stern & Pyles, 1986). We coded early data with descriptive phrases or words. As more data were collected, these codes were revised. We developed emerging categories from the clustering of codes and compared them against each other to ensure that they were mutually exclusive and covered the range of variations within the data (Baker, Wuest, & Stern, 1992). For example, some participants indicated that at times, they gave someone else the responsibility of their diabetes management, particularly when they or a significant other was in crisis. Initially, we described this behavior as “abandoning control.” As we gathered more data, we began to see that some participants reported such situations in terms of “deciding who would take control.” In subsequent interviews, we asked questions about the criteria they used to determine when to give the control of their diabetes to another and what such situations represented to them. We subsequently revised the category to “assuming control.”
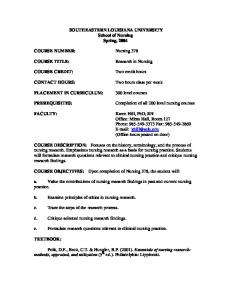
RESEARCH FINDINGS The developmental model of expertise in diabetes management that has arisen from the research findings (see Figure 1) includes both trajectory and age-related development. It is trajectory based in that there are sequential phases, characterized by landmarks, transitions, and alterations in one’s response to diabetes management. The development of expertise is age related in that movement through these phases is often determined or influenced by the developmental age at the time as well as the person’s age at the onset of the disease. The participants described the progression of becoming an expert in the management of Type 1 diabetes as a developmental process in which one evolves from passive recipient to active participant. They viewed this as similar to physical development in that one develops increasingly sophisticated skills, knowledge, and abilities to cope with the progressively complex demands of each phase. A schematic representation of the grounded theory of the developmental evolution of expertise in self-management of diabetes is found in Figure 1. The development of expertise is portrayed as a movement through four phases: passive compli-
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
Paterson, Thorne / DIABETES SELF-MANAGEMENT
409
Figure 1. Model of the development of expertise in diabetes selfmanagement.
ance, naive experimentation, rebellion, and active control. Eight participants identified that they had experienced all phases of development, in that order. Others experienced only two or three out of the four phases. Three participants experienced naive experimentation after, and not before, the rebellion phase. The phases were not always distinct and were at times overlapping. Several participants indicated that they retained aspects of a previous phase until the behaviors associated with the new phase were well integrated (“I still rebelled sometimes until I was confident that I knew how to be in control.”). As well, there was evidence of change within phases. For example, one participant in the active control phase learned new aspects of self-management when she became pregnant during the course of the research. The participants emphasized, however, that once they had decided to assume active control in self-management there may have been fluctuations in the desire to assume control but “you never go back to where you were before.”
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
410
CLINICAL NURSING RESEARCH / November 2000
PASSIVE COMPLIANCE
All participants described a phase of passive compliance that occurred when the individual was still “reeling from the shock” of the diagnosis. In this stage, the individual adhered strictly to the rules of management as identified by health care professionals and family members. Participants laughed when they described how rigidly they followed the prescribed regimen in this phase (e.g., counting off 26 peas for a meal). They described this phase as one in which they “craved structure and rules.” One participant admitted she had been babied by her parents in this phase but indicated that this enabled her to learn the basics of disease management and to accept that “the diabetes was not going away.” Participants experienced passive compliance for a few weeks to 36 years. The duration was influenced by a number of factors (e.g., age at onset, degree of encouragement by others, needs of significant others). Two participants who had another chronic illness before the diagnosis of diabetes stated that experience with another disease made them realize that passive compliance was “destructive, dangerous even, to yourself and your well-being.” One woman stated that she had remained in this phase “longer than most” because her reliance on her family at this time “seemed to bring our family closer together.” NAIVE EXPERIMENTATION
Naive experimentation was characterized by a series of trial and error manipulations of a prescribed regime. In this phase, participants experimented with altering insulin or diet; however, they lacked the skills to do so effectively. Participants described this stage as “short-lived” when they discovered they were feeling too ill to do the things they wanted. “I was feeling so whacked out from all those lows that I didn’t have any energy to do anything.” I thought that I’d see what would happen if I took more insulin in the morning and none in the evening. I didn’t know what I was doing. I just knew I wanted to take charge of my diabetes. But I landed up in hospital.
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
Paterson, Thorne / DIABETES SELF-MANAGEMENT
411
Fourteen participants stated their progression from passive compliance to naive experimentation was prompted by a need to have more control about the decisions that affected them and a frustration about the strict management regimens imposed by parents, professionals, or others. Three others stated that they had progressed to this phase when they had experienced a period of denying their diabetes and rebelling against it. “I had tried to pretend I didn’t have it and I nearly died. I knew then I wanted to take control. I just didn’t know how.” The naive experimentation phase lasted from 2 days to 7 months. One man stated, “It was this that helped me realize how little I knew and how much there was to learn. I needed to learn how to control my diabetes. It wasn’t going to happen simply because I wanted it.” Four participants indicated that they progressed to naive experimentation when they left home as a young adult to attend college or to work. One said, “In my parent’s home, every decision was made for me. That first couple of years at college was my attempt to make my own decisions.” REBELLION
Fourteen participants indicated that they had experienced a stage of rebellion in learning how to manage their diabetes. They reached this phase directly from passive compliance or from naive experimentation. Rebellion was characterized by denial of the diabetes, particularly in the presence of others. This took the form of ignoring the diet and alcohol restrictions, hiding the need for insulin, and falsifying or neglecting glucometer readings. I remember going through my adolescence thinking I can deny this whole thing. I can drink Cokes with the kids. So, I go drink all the Coke, go through the hyperglycemia, suffer all the side effects rather than admit that I couldn’t keep up with them. I didn’t manage my diabetes during my adolescence. I denied it.
The rebellion stage was similar to naive experimentation in that both phases were motivated by the goal to assume control and both resulted in wide swings in blood glucose levels and negative health outcomes. As one participant said, “I didn’t want
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
412
CLINICAL NURSING RESEARCH / November 2000
others to tell me what to do or have my life dictated by my diabetes. So I pretended it didn’t exist and I felt terrible.” Participants who experienced the rebellion stage stated that there were several factors that prompted them to enter this stage. The primary reason was the desire to be the same as peers. One participant who had not experienced a rebellion phase stated that she thought she had avoided this phase because she “already had an identity of being different” by the time she was diagnosed and did not aspire to being “one of the crowd.” Other factors that prompted progression to the rebellion phase included feeling constrained by the rigid regime enforced by parents or health care professionals, being a “teenager who thinks that they’re immortal so nothing bad can happen to them,” and anger about having to attend to the disease when other life priorities seemed more important. Several participants commented that they believed that rebellion was a necessary part of learning to manage diabetes, useful in determining the parameters of behavior and the outcomes of actions, and leading to the individual seeking alternatives “other than the diabetes ruling your life.” Nine participants who had been diagnosed as children experienced the rebellion phase when they were teenagers. Some believed that this was typical adolescent rebellion. Five participants who described a rebellion in adulthood stated that every person has “a stage of rebelling, a stage of denying the diabetes.” “I was around 30 when I felt like I’d had enough. I think all diabetics do that at some time or other. So, for awhile, I rebelled just like a teenager.” ACTIVE CONTROL
The participants progressed to the phase of active control directly from the passive compliance, the rebellion, or the naive experimentation stage. In this phase, they made a conscious decision to assume control of their diabetes self-management. “I think at one point that the diabetes was controlling me and now I’m controlling it.” Participants defined control as being able to mediate the effects of the disease so that they could live as “normally as possible.” They said that assuming control entails a redefinition of the meaning of the illness, blood glucose testing, relationships with others, and the self as the person who lives with diabetes. They identified outcomes of active
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
Paterson, Thorne / DIABETES SELF-MANAGEMENT
413
control as self-satisfaction, being able to live a normal life, a good quality of life, acceptance of the illness, and health. The participants identified a number of factors that caused them to wish for and attain active control in their diabetes management. The influence of others in this regard was significant, particularly those whose experience with diabetes convinced them that assuming control was important: “She had every complication there was and she was always in hospital. I didn’t want to be like her.” Seven participants stated that a practitioner had encouraged them to assume control and taught them how to make self-management decisions. Other factors that caused participants to progress to active control included discovering that adhering to the prescribed regimen did not necessarily mean that they would feel well, perceiving diabetes-related complications as outcomes of previous phases, deciding that an inflexible regimen is impossible, recognizing that former patterns of self-management posed a risk to significant others, and losing faith in health care professionals’ ability to manage their diabetes. Developing expertise was described by the participants as “an ongoing learning process” in which one learns to “put the diabetes into perspective” in the process of assuming an active role in self-management. Expertise was also identified as a “natural outcome” of this phase that is realized only after the individual has developed sufficient confidence, competence, and social supports to assume active control in self-management in familiar and unfamiliar situations. Confidence was defined in terms of “knowing that I could do it because I wanted it badly enough” and “being confident in what I knew about diabetes and my own body that I could make the right decisions for me.” Confidence was enhanced by maintaining a “consistent routine” of diet, blood glucose testing, and exercise that rarely varied. “I have the same breakfast day in and day out. It helps me to feel that I have a handle on things.” Competence in self-management was achieved through vigilant attention to the body and the disease. Participants monitored how their bodies responded in specific situations and to particular interventions so that they would be able to effectively respond to these in the future. Vigilant attention was achieved by learning about diabetes, “listening to the body,” maintaining a record of daily self-care activities, and regular and frequent blood glucose testing.
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
414
CLINICAL NURSING RESEARCH / November 2000
I started to pay attention to my body. For clues that I was getting low or high (blood glucose), not what the blood sugar said and not what else was happening but what was happening to me internally. I started to become more aware of subtle signs . . . such as the degree of thirst, degree of blurred vision, degree of mental acuity. I learned to know my body and its responses just by really concentrating, by making a concerted effort to recognize that I have to be in control. The turning point for me was when I started seeing that the glucometer was not controlling me, it was the thing that set me free. I began to see that it let me know if I had made a right or a wrong decision and it helped me to predict what might happen later that day. I am able to have some control of my diabetes because of it.
All participants stressed that assuming active control does not equate with perfection in self-management. They stated that they accept there are times when they may not know why a blood glucose level is abnormal. They do not view such situations as testimony to their self-management ability. “Sometimes it just happens.” To assume control, the participants learned to assist others to become the partners they needed in their diabetes management. They described shopping around for and demanding health care professionals who would acknowledge their expertise and who would agree to collaborate in decisions about care. The only major difference between the physician-nominated and self-nominated participants was that all but 1 of the self-nominated group had been unable to locate such a professional. All of the physician-nominated participants had established a collaborative relationship with a health care professional. Several reported that their physicians deferred to their judgment about diet and insulin even when they were hospitalized. “I think, first of all, he gives credit to the clients for having intelligence and realizing that they can control their disease and learn to live with it.” Significant others were often recruited to be self-management partners. They provided support and encouragement as well as observations of the participant’s behavior/affect, which served as an alert to a problem. “He often knows before I do that I’m hypoglycemic, especially if I’m busy and not paying attention.” Four participants chose to ask a physician and 2 others asked a spouse to “take over the diabetes decisions” for a temporary period when they were ill, stressed, or preoccupied with
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
Paterson, Thorne / DIABETES SELF-MANAGEMENT
415
other priorities in their lives. The participants stated that this was not an attempt to regress to earlier phases but rather an effort to exert control by making a decision about what would be best. I gave the control over to Dr. X then. He made the decisions I normally would have made. I was so stressed, so tired, so scared of failing (at university) while at the same time wondering if this really was what I wanted. I couldn’t look after my diabetes then. I gave up my control to Dr. X and he took control temporarily.
Another such decision was what one participant referred to as a “calculated cheat.” On these occasions, participants chose to make an alteration to their usual diet or exercise regime by calculating the risks of this alteration and compensating for them. Participants agreed that calculated cheats are important to experience on occasion “because then you feel you are human, not just a diabetic.” They stressed, however, that these occasions are planned and occur within carefully defined parameters (“I don’t let myself go hog wild. I have a small piece of cake without much icing just to have a celebration once in awhile.”).
DISCUSSION The process of learning to become an expert was described by the participants as entailing a philosophical shift from being controlled by the disease to controlling the impact of diabetes. Developmental age provides an interplay that influences the trajectory of expertise, but neither the progression through the stages nor the nature of the interplay of age is consistent to all participants. For example, the rebellion phase may occur not in adolescence but later in middle adulthood. Instead, the development of expertise is a highly individualized evolution. It is both a process of learning to assume active control and an outcome of that process. Similar to other research that has investigated the perspectives of persons with diabetes (Paterson et al., 1998), the concept that is most prevalent in the participants’ descriptions of their evolution as experts is “control.” Their central goal was to assume control of their disease management. This was evident
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
416
CLINICAL NURSING RESEARCH / November 2000
even in the rebellion phase when they attempted to attain control by denying the disease. Participants’ struggle for control encompasses much more than the control of discomforting symptoms or blood glucose levels. Health care professionals often have regarded people who display the behaviors of the naive experimentation or rebellion as irrational (Kaplan, 1991). The findings of the research suggest an alternate explanation for this behavior; naive experimentation and rebellion may reflect attempts to exert control to achieve desired outcomes in ways that are perceived as less costly than that required by active control or passive compliance. As well, passive compliance, rebellion, and naive experimentation may be the “testing ground” (Reeves, Merriam, & Courtenay, 1999) to develop competence, self-image, social support, and affective and behavioral coping strategies to assume active control of self-management. The participants proposed that persons with diabetes need the support of others in a way that fosters their expert skills in diabetes management. Adolescents in one study who were paired with adults with long-standing diabetes developed a greater awareness of the potential for assuming control of their diabetes management (Daley, 1992). Perhaps a mentoring program in which newly diagnosed people were paired with those who were expert in self-management might accomplish the same outcome. A limitation of the research is that the participants contributed statements about pre-expert phases of development in retrospective accounts in the interviews. This may explain why the expert phase (active control) that was revealed in prospective accounts of the MTAs and PTAIs was portrayed as less linear and simplistic than in other phases. There is a danger in interpreting the results of this research as indicating that all people with diabetes should incorporate an active role in self-management. Participants in this study did not always wish to expend the energy or time that was necessary to be an expert in diabetes self-management because they had other priorities in their lives. Until we know a great deal more about who assumes the expert role and why, as well as the outcomes of the expert role, nurses should be cautious about communicating that the way of the expert is the right way to manage diabetes.
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
Paterson, Thorne / DIABETES SELF-MANAGEMENT
417
CLINICAL APPLICATION There are a number of clinical applications of the research findings. Nurses who interact with people with diabetes who appear to be passive, deny their disease, or make naive decisions should not assume that they do not care enough about their diabetes or simply need more education about the disease to manage it successfully. Although in clinical settings nurses use physiological data to determine the efficacy of disease management strategies, people who acknowledge their expertise in self-management interpret such data in the context of what they know to be their usual patterns of body response and what they believe is necessary to achieve well-being. Nurses should focus on what the person believes to be the goals of self-management as well as the personal and social context in which the person will manage the diabetes rather than solely on glycemic control and control of symptoms. According to the participants, the struggle to attain and maintain control involves a complex interplay of factors, of which metabolic control and related symptoms are only two. This is an important insight as health care professionals have traditionally focused solely on metabolic control and diabetes-related symptoms in their discussions with clients about self-management of the disease (Price, 1993). At least equally as significant are the components of confidence, competence, and social support that contribute to individuals’ ability to maintain active control in their self-management. Practitioners should recognize that metabolic control may not be the primary goal for people who manage their diabetes successfully. This highlights the importance of knowing clients with diabetes as individuals, as people with unique goals and ways of perceiving and living with their illness. According to the participants, some health care professionals made a significant impact on their willingness and ability to progress to the active control phase. They did this by expecting and modeling an alternate way of being with health care providers; that is, that of partner. Because nurses in many settings interact with persons who are at some point in the trajectory of developing expertise in a complex self-management approach, they are ideally placed to engage with patients in a collaborative mutual learning adven-
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
418
CLINICAL NURSING RESEARCH / November 2000
ture. Understanding self-management of Type 1 diabetes as a complex and challenging developmental phenomenon gives nurses a way in which to understand a range of attitudes, coping styles, and management strategies. As we develop knowledge from the perspective of those who have successfully learned to be expert decision makers in active control of their disease management, it will be increasingly possible for nurses to interact with their patients in ways that facilitate growth and learning instead of compliance and passivity.
REFERENCES Annells, M. (1996). Grounded theory method: Philosophical perspectives, paradigm of inquiry, and postmodernism. Qualitative Health Research, 6, 379-393. Baker, C., Wuest, J., & Stern, P. N. (1992). Method slurring: The grounded theory/phenomenology example. Journal of Advanced Nursing, 17, 1355-1360. Blaum, C. S., Velez, L., Hiss, R. G., & Halter, J. B. (1997). Characteristics related to poor glycemic control in NIDDM patients in community practice. Diabetes Care, 20, 7-11. Blumer, H. (1969). Symbolic interactionism. Englewood Cliffs, NJ: Prentice Hall. Clay, D. L. (1995). Examining systematic differences in adaptation to chronic illness: A growth modelling approach. Rehabilitation Psychology, 40, 61-70. Daley, B. A. (1992). Sponsorship for adolescents with diabetes. Health Social Work, 17, 173-182. Diedricks, J.P.M., & Bal, R. M. (1997). Perspectives on patient career in chronic illness: Theoretic status and practical implications. Sociological Focus, 30, 167-175. Ellison, G. C., & Rayman, K. M. (1998). Exemplars’ experience of self-managing Type 2 diabetes. Diabetes Educator, 24, 325-330. Fontana, A., & Frey, J. H. (1994). Interviewing: The art of science. In N. Denzin & Y. Lincoln (Eds.), Handbook of qualitative research (pp. 361-376). Thousand Oaks, CA: Sage. Fonteyn, M., & Fisher, A. (1995). Research corner: Use of think aloud method to study nurses’ reasoning and decision-making in clinical practice settings. Journal of Neuroscience Nursing, 27, 124-128. Glaser, B. G., & Strauss, A. L. (1967). The discovery of grounded theory. Chicago: Aldine. Hampson, S. E., Glasgow, R. E., & Foster, L. S. (1995). Personal models of diabetes among older adults: Relationship to self-management and other variables. Diabetes Educator, 21, 300-307. Harper, D. C. (1991). Paradigms for investigating rehabilitation and adaptation to childhood disability and chronic illness. Journal of Pediatric Psychology, 16, 533-542.
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
Paterson, Thorne / DIABETES SELF-MANAGEMENT
419
Hentinenen, M., & Kyngas, H. (1992). Compliance of young diabetics with health regimes. Journal of Advanced Nursing, 17, 530-536. Hernandez, C. A. (1991). The lived experience of Type 1 diabetes: Implications for diabetes education. Unpublished doctoral dissertation, University of Toronto, Canada. Jayne, R. L. (1993). Self-regulation: Negotiating treatment regimens in insulin-dependent diabetes. Unpublished doctoral dissertation, University of California, San Francisco. Kaplan, R. M. (1991). Health-related quality of life in patient decision making. Journal of Social Issues, 47, 69-90. Kyngas, H., & Barlow, J. (1995). Diabetes: An adolescent’s perspective. Journal of Advanced Nursing, 22, 941-947. Nyhlin, K. T. (1990). Patient’s experiences in the self-management of diabetes mellitus (UMEA University Medical Dissertations, ISSN 0346-6612). Umea, Sweden: University of Umea. Paterson, B. L., & Sloan, J. (1994). A phenomenological study of the decision-making experience of individuals with long-standing diabetes. Canadian Journal of Diabetes Care, 18, 10-19. Paterson, B., Thorne, S., & Dewis, M. (1998). Adapting to and managing diabetes. Image: Journal of Nursing Scholarship, 30, 57-62. Price, M. J. (1988). Perceived uncertainty associated with the management trajectory of a chronic illness—Diabetes mellitus. Unpublished doctoral dissertation, University of California, San Francisco. Price, M. (1993). Exploration of body listening: Health and physical selfawareness in chronic illness. Advances in Nursing Science, 15, 37-52. Reeves, P. M., Merriam, S. B., & Courtenay, B. C. (1999). Adaptation to HIV infection: The development of coping strategies over time. Qualitative Health Research, 9, 344-361. Standiford, D. A., Turner, A. M., Allen, S. R., Drozda, D. J., & McCain, G. C. (1997). Personal illness models of diabetes: Preadolescents and adolescents. Diabetes Educator, 23, 147-151. Stern, P., & Pyles, S. (1986). Using grounded theory methodology to study women’s culturally based decisions about health. In P. N. Stern (Ed.), Women, health, and culture (pp. 1-23). Washington, DC: Hemisphere. Thorne, S., Kirkham, S. R., & MacDonald-Emes, J. (1997). Interpretive description: A noncategorical qualitative alternative for developing nursing knowledge. Research in Nursing & Health, 20, 169-177. Wuest, J. (1995). Precarious ordering: A theory of women’s caring. Unpublished doctoral dissertation, Wayne State University, Detroit, MI. Wysocki, T., Taylor, A., Hough, B. S., Linscheid, T. R., Yeates, K. O., & Naglieri, J. A. (1996). Deviation from developmentally appropriate self-care autonomy. Diabetes Care, 19, 119-125.
Barbara Paterson, R.N., Ph.D., is an associate professor at the University of British Columbia School of Nursing. Sally Thorne, R.N., Ph.D., is a professor at the University of British Columbia School of Nursing.
Downloaded from http://cnr.sagepub.com at PENNSYLVANIA STATE UNIV on February 5, 2008 © 2000 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.