Review For reprint orders, please contact:
[email protected]
Considerations in the role of male circumcision in the prevention of HIV transmission in the USA Male circumcision (MC) has been associated with a reduced risk for female–male HIV transmission in observational and ecological studies, as well as clinical trials. Three recent randomized, controlled trials in sub-Saharan Africa demonstrated a 50–60% reduction in HIV incidence among men randomized to circumcision compared with uncircumcised men. In 2007, WHO/UNAIDS recommended that MC be recognized as an additional efficacious intervention to prevent sexual transmission of HIV from women to men. This article reviews information on the potential role of MC for HIV prevention in the USA where, compared with the African clinical trial countries, the prevalence of HIV infection is lower, the main route of HIV transmission is male–male sex rather than heterosexual sex and the prevalence of MC is higher. KEYWORDS: heterosexual n
n
sexual transmission n USA
CME
HIV n male circumcision n male–male sex n prevention
Medscape: Continuing Medical Education Online
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Future Medicine Ltd. Medscape, LLC is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Medscape, LLC designates this educational activity for a maximum of 1.0 AMA PRA Category 1 Credits™. Physicians should only claim credit commensurate with the extent of their participation in the activity. All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test and/or complete the evaluation at http://cme.medscape.com/CME/futuremedicine; (4) view/print certificate.
Peter H Kilmarx†, Katrina Kretsinger & Gregorio A Millett Author for correspondence: Division of HIV/AIDS Prevention, Centers for Disease Control & Prevention, 1600 Clifton Road, MS E-45, Atlanta, GA 30333, USA Tel.: +1 404 639 8998; Fax: +1 404 639 6127; E‑mail:
[email protected]
†
Learning objectives Upon completion of this activity, participants should be able to: n Describe research into whether male circumcision is protective against HIV infection n Identify the subgroup of patients most likely to benefit from male circumcision in the prevention of HIV infection n Describe the adverse events and cost associated with male circumcision n Specify trends and recommendations for male circumcision in the USA Financial & competing interests disclosure CME Author: Charles P Vega, MD, FAAFP, Associate Professor; Residency Director, Department of Family Medicine, University of California, Irvine, USA. Disclosure: Charles P Vega, MD, FAAFP, has disclosed that he has served as an advisor or consultant to Novartis, Inc. Editor: Elisa Manzotti, Editorial Director, Future Science Group. Disclosure: Elisa Manzotti has disclosed no relevant financial relationships. Authors and Credentials: Peter H Kilmarx, Division of HIV/AIDS Prevention, Centers for Disease Control & Prevention, 1600 Clifton Road, MS E-45, Atlanta, GA 30333, USA. Disclosure: Peter H Kilmarx has disclosed no relevant financial relationships. Katrina Kretsinger, Division of HIV/AIDS Prevention, Centers for Disease Control & Prevention, 1600 Clifton Road, MS E-45, Atlanta, GA 30333, USA. Disclosure: Katrina Kretsinger has disclosed no relevant financial relationships. Gregorio A Millett, Division of HIV/AIDS Prevention, Centers for Disease Control & Prevention, 1600 Clifton Road, MS E-37, Atlanta, GA 30333, USA. Disclosure: Gregorio A Millett has disclosed no relevant financial relationships. 10.2217/HIV.09.6 © 2009 Future Medicine Ltd
HIV Ther. (2009) 3(3), 241–254
ISSN 1758-4310
241
Review | Kilmarx, Kretsinger & Millett Male circumcision (MC) is the surgical removal of some or all of the foreskin, or prepuce, from the penis [1] . MC has long been associated with cultural rites and imbued with religious significance in many regions of the world. In some settings, hygiene and health consequences of MC have been factors in adopting the practice. In recent years the role of MC in preventing female–male HIV transmission has been demonstrated and MC is being implemented as an HIV prevention intervention, especially in sub-Saharan Africa.
242
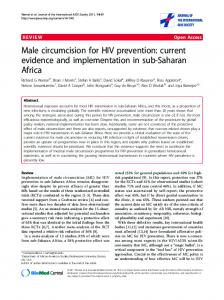
Biological plausibility of male circumcision for HIV prevention The foreskin can serve as a portal of entry for HIV infection, lending biological plausibility to the role of circumcision in preventing HIV acquisition through insertive sexual intercourse. The inner mucosa of the foreskin is less keratinized than the dry external skin of the penis shaft. It also has a higher density of target cells for HIV infection (Langerhans cells, CD4 + cells and macrophages) close to the skin surface [2,3] . Foreskin mucosal tissue has been shown to be more susceptible to HIV infection than cervical mucosa or the external foreskin surface in laboratory studies [4] . During sexual intercourse, the foreskin retracts from the glans of the erect penis and is inverted over the shaft of the penis, exposing the inner mucosal surface of the foreskin to the body fluids of the sex partner, and potentially to HIV infection (Figure 1) [2] . It has also been argued that the foreskin may have greater susceptibility than dry epithelial tissue to traumatic small tears and disruptions during sexual intercourse, thereby providing a portal of entry for pathogens including HIV [5] . The micro-environment in the preputial sac between the unretracted foreskin and the glans penis may also be conducive to viral survival [4] . Finally, higher rates of sexually transmitted diseases (STDs), such as syphilis [6] and herpes simplex virus type‑2 infection [7] , have been observed in uncircumcised men; these conditions may independently increase susceptibility to HIV infection [8] .
observations, or evaluations of HIV infection at the population level, initially suggested a link between MC and reduced risk of HIV infection. Although confounding owing to assoc iations between circumcision, culture, religion and risk be havior may account for some of the differences in HIV infection prevalence, the countries in Africa and Asia with a prevalence of MC of less than 20% have HIV infection prevalence several times higher than countries in regions where more than 80% of men are circumcised [9] . International observational studies have also suggested that MC is associated with lower rates of HIV infection. A systematic review and meta-analysis that focused on heterosexual transmission of HIV in Africa was published in 2000 [10] . It included 19 cross-sectional studies, five case–control studies, three cohort studies and one study of discordant couples. A substantial protective effect of MC on risk for HIV infection was noted, along with a reduced risk for genital ulcer disease. After adjusting for confounding factors in the populationbased studies, the relative risk for HIV infection was 44% lower in circumcised men. The strongest association was observed in high-risk men, such as patients at STD clinics, for whom the adjusted relative risk was 71% lower for circumcised men. Another review that included stringent assessment of ten potential confounding factors, which was stratified by study type or study population, was published in 2003 [11] . Most of the 35 observational studies were from Africa. A total of 19 of the studies were conducted in high-risk populations. These found a consistent, substantial protective effect, which increased with adjustment for confounding variables. Four of these studies in high-risk populations were cohort studies; all demonstrated a protective effect, with two being statistically significant. The 16 studies in the general population had inconsistent results. The one large, prospective cohort study in this group showed a significant protective effect, with the odds of infection being 42% lower in circumcised men [12] .
Observational studies of male circumcision & HIV infection Several types of research have suggested that MC reduces the risk of HIV acquisition by men during penile–vaginal sex, including ecological surveys, observational studies and randomized, controlled trials. Ecologic
International clinical trials of male circumcision for HIV prevention Three randomized, controlled trials (Male Circumcision and HIV Rates in Kenya; Effect of Male Circumcision on HIV Incidence [ANRS 1265]; and Male Circumcision for HIV Prevention in Rakai, Uganda) have been undertaken in
HIV Ther. (2009) 3(3)
future science group
Role of male circumcision in the prevention of HIV transmission in the USA predominately heterosexual populations in subSaharan Africa to determine whether circumcision of adult males will reduce their risk for HIV infection. The controlled follow-up period in all three was stopped early and the control group offered circumcision when interim analyses found that medical circumcision significantly reduced male participants’ HIV infection risk. The controlled follow-up period in the study in South Africa [13] was stopped in 2005 and those in Kenya [14] and Uganda [15] were stopped in 2006. In intent-to-treat analyses, men who had been randomly assigned to the circumcision group had a 60% (South Africa), 53% (Kenya) and 51% (Uganda) lower incidence of HIV infection compared with men assigned to the group to be circumcised at the end of the study. In all three studies, some men who had been assigned to be circumcised did not undergo the procedure, and vice versa. When the data were re-analyzed to account for these deviations in per-protocol analyses, men who had been circumcised had a 76% (South Africa), 60% (Kenya) and 55% (Uganda) reduction in risk of HIV infection compared with those who were not circumcised. In 2008, results of longer-term follow-up from the Kenya study were reported, indicating that the protective effect of circumcision was durable – with 42 months of follow-up, a 64% reduction in HIV infection risk was seen in circumcised men compared with uncircumcised men [16] . Although these results may not be generalizable to the USA, in general, risk compensation was not observed in the circumcised men [17] , and MC was not associated with sexual dysfunction [18] . Similarly, MC did not adversely affect sexual satisfaction or function in the Ugandan trial [19] . Male circumcision & female–male HIV transmission in the USA Two published observational studies have reported on the association between circumcision and risk of HIV infection in heterosexual men in the USA. In one prospective study of heterosexual men attending an urban STD clinic, when other risk factors were controlled, uncircumcised men had a 3.5-fold higher risk for HIV infection than men who were circumcised. However, this association was not statistically significant [8] . In an analysis of clinic records for African–American men attending STD clinics in Baltimore (MD, USA), circumcision was not associated with HIV infection status overall, but among men with known HIV exposure to an future science group
| Review
Outer foreskin Inner foreskin
Urethral meatus Glans penis
Frenulum HIV entry
Outer foreskin
Inner foreskin
No HIV entry
Frenulum
Figure 1. Position of the foreskin in the flaccid and erect uncircumcised penis. (A) Flaccid uncircumcised penis. (B) Erect uncircumcised penis with the foreskin retracted, showing likely sites of HIV-1 entry. Reproduced with permission from [2] .
HIV-infected female partner, circumcision was associated with a statistically significant 51% reduction in risk for HIV infection [20] . Male circumcision & male–female HIV transmission Studies have not conclusively demonstrated an effect of MC on the risk of HIV transmission from infected men to their female partners. Data from Uganda on male–female transmission demonstrated a somewhat higher rate of HIV acquisition among initially HIV-negative women whose HIV-infected male partners were circumcised compared with women whose HIV‑infected male partners remained uncircumcised, although this was not statistically significant [21] . The effect was greatest among couples who resumed sexual relations at least 5 days prior to certified postsurgical wound healing, suggesting an increased risk of HIV acquisition with early resumption of sex. In an earlier study of couples in Uganda in which the male partner was HIV-infected and the female partner was initially HIV-negative, the infection rates of the female partners differed by the circumcision status and viral load www.futuremedicine.com
243
Review | Kilmarx, Kretsinger & Millett of the male partners. If the male blood HIV viral load was less than 50,000 copies/ml, there was no HIV transmission if the man was circumcised, compared with a rate of 9.6 per 100 person-years if the man was uncircumcised [22] . If viral load was not controlled for, there was a nonstatistically significant trend towards a reduction in the male–female transmission rate from circumcised men compared with uncircumcised men. Such an effect may have been due to decreased viral shedding from circumcised men or to a reduction in ulcerative sexually transmitted infections acquired by female partners of circumcised men [23] . Male circumcision & HIV transmission in men who have sex with men The HIV risk reduction benefit demonstrated in the randomized trials in Africa accrued to men engaging predominately in insertive penile–vaginal sex. The presumed protective mechanism is decreased HIV entry and infection through target cells on the foreskin. Thus, any potential biologic benefit of circumcision for men who have sex with men (MSM) engaged in penile– anal sex is likely to accrue only to insertive partners and not to receptive partners. However, the risk for HIV acquisition among MSM engaging in penile–anal sex is substantially greater for the anal receptive partner than for the insertive partner [24,25] . In addition, although it is not well studied, it seems that in many settings many or most MSM practice both insertive and receptive sex. In the limited studies in the USA, approximately half of men self-identify as versatile partners, one quarter each identify as either predominately insertive or predominately receptive and substantial proportions of ‘tops’, men who are predominately insertive, also report practicing receptive anal intercourse [26,27] . Therefore, any potential benefit of MC in reducing HIV infection risk from insertive anal sex is diluted both at the individual level, as most men remain at higher risk from receptive sex and at the population level because chains of HIV transmission through receptive anal intercourse would persist even if circumcision reduced risk of transmission through insertive sex. Some observational studies have shown higher rates of HIV acquisition among uncircumcised MSM compared with circumcised MSM. When controlling for the number of male sex partners and unprotected sex with an HIV-positive partner, circumcision was associated with decreased odds of incident HIV 244
HIV Ther. (2009) 3(3)
infection (OR: 0.5, 95% CI: 0.25–21.0) in a vaccine preparedness cohort followed from 1995 to 1997 [28] . However, other observational studies have failed to show a significant benefit (or risk) of circumcision. In a cross-sectional survey of Black and Latino MSM in three USA cities, there was no evidence that being circumcised was protective against HIV infection, even among men who had engaged in unprotected insertive but not unprotected receptive anal sex [29] . Similarly, no association was found in an Australian study of MSM [30] , although a subsequent study of MSM in Australia did report a significantly reduced HIV infection risk in circumcised men who were predominately insertive [31] . The study authors noted that because more infections were associated with receptive intercourse, lack of circumcision accounted for only 9% of the infections in the study overall. A recent meta-analysis of unpublished as well as published data from 15 studies that quantitatively examined the association between circumcision and HIV infection among MSM found little overall effect, with a weighted overall odds ratio of 0.95 (95% CI: 0.81–81.11) among a total of 53,567 MSM participants, 52% of whom were circumcised [32] . The association remained nonsignificant when stratified by study type (cross-sectional and prospective) or when limited to MSM who engaged exclusively in insertive anal sex. Some have advocated for randomized, controlled clinical trials to assess whether circumcision reduces HIV infection risk in MSM [33,34] . Designing such a trial would be challenging. Enrollment could be limited to populations of men who practice predominately insertive sex, which would exclude substantial proportions of MSM. Alternatively, the trials could be designed to be large enough to detect what would be a relatively small prevention benefit if men who also practice and remain at risk from receptive sex were enrolled. In the absence of clinical trial data, public health guidance based on the best available observational data is needed to inform men’s choices. Other potential health benefits of male circumcision Studies indicate that MC is associated with other health benefits as well [1] , such as reduced rates of some sexually transmitted infections [6,7,35–37] , penile cancer [38,39] , cervical cancer in female partners [35] and infant urinary tract infections [1,40,41] . future science group
Role of male circumcision in the prevention of HIV transmission in the USA Risks & adverse effects associated with male circumcision Any potential benefit of circumcision must be weighed against the risks. Reported rates of immediate complications from circumcision in the neonatal period range from 0.2 to 2% [1,42,43] and vary by type of study, setting, operator and surgical technique or instrument used. The most common surgical complications reported have been bleeding and infection, usually minor and easily managed. Other reported complications are rare, including dehiscence, unsatisfactory cosmesis, skin bridges, urinary retention, meatal stenosis and retained surgical devices. These studies probably underestimate the rate of postcircumcision complications since patients were not followed after discharge from the hospital. A longitudinal study found rates of penile problems after 1 year of 5% in circumcised boys and 1% in uncircumcised boys. However, after 8 years the rates were 11 and 19%, respectively. Most of these problems were penile inflammation including balanitis, meatitis and inflammation of the prepuce [44] . At least one case of fatal complications of circumcision in North America has been reported [45] . Complication rates reported for adult circumcisions in the three African clinical trials were of similar magnitude and severity and ranged from 2 to 4%, most commonly pain, bleeding, infection and unsatisfactory cosmesis [46] . There were no reported deaths or long-term sequelae documented. More recently, higher complication rates were documented for circumcisions performed outside the clinical trial setting in Kenya; 35.2% in men circumcised by traditional practitioners and 17.7% in clinical settings, underscoring the need for better training and resources in those settings [47] . Effect of male circumcision on sexual function & penile sensation The foreskin is a highly innervated structure [48] , and decreased sensitivity of the glans penis to fine touch can occur following circumcision, leading some authors to express concern that its removal may compromise sexual sensation or function [49] . In one survey of 123 men following medical circumcision in the USA, men reported worsened erectile function and decreased penile sensitivity, but reported no change in sexual activity and improved sexual satisfaction [50] . Other studies conducted among men after adult circumcision have found that future science group
| Review
relatively few men report that their sexual functioning is worse after circumcision; most report either improvement or no change [18,19,51–53] . Cost of male circumcision The medical costs of circumcision must also be accounted for in considering the role of MC for HIV prevention in any setting. While MC has been shown to be a cost-saving HIV-prevention intervention in sub-Saharan Africa [54,55] , the calculus is different in the USA where medical costs are higher and the risk of HIV infection is lower. In the USA, the estimated cost of infant circumcision ranges from US$200 to as much as $900 [56,57,101] . According to Medicaid reimbursement rates, the cost of MC in the USA after the neonatal period is at least $1700 and could be considerably higher in the private sector [102] . Cost–effectiveness analyses of male infant circumcision, circumcision for high-risk heterosexual men and circumcision for MSM are being conducted by the CDC to help guide recommendations for the USA. Ethical considerations in infant male circumcision Ethical concerns have been raised in asking parents to make decisions about elective surgery during infancy, particularly when it is done primarily to protect against risks of HIV infection and other health outcomes that do not occur until young adulthood or later [58] . By the time an infant has reached the age of sexual debut, the HIV epidemic may have changed substantially, both in terms of prevalence and risk groups, and the introduction of other modalities may have overtaken circumcision as a preventive strategy. Although infant circumcision is less expensive and has fewer associated adverse outcomes than adult circumcision, the choice by parents to circumcise an infant primarily for a distant prevention goal denies the infant the right of autonomy in medical decision-making. However, other ethicists have found this to be an appropriate parental proxy decision [59,60] . HIV infection in the USA In 2006 in the USA, there were an estimated 56,300 new HIV infections [61] . Of these, 73% were in males, 45% were in Black people and 53% were in MSM. A total of 5250 cases in men were attributed to high-risk heterosexual contact (or ~10% of all infections [in both sexes] attributed to female–male transmission [62]) . This proportion differed by race and ethnicity; in White people, www.futuremedicine.com
245
Review | Kilmarx, Kretsinger & Millett 5% of all cases were attributable to female–male transmission, compared with 13% in Black people and 10% in Hispanics. An overall HIV infection prevalence of 0.45% was estimated for the general population age greater than 13 years in the USA in 2006. The prevalence in Black people (1.7%) was nearly eight-times as high as in White people (0.22%), while the prevalence in Hispanics (0.58%) was more than twice as high [63] . Status of male circumcision in the USA Nonreligious MC was introduced to the USA in the late 1800s [64] , and by the 1940s, an increasing proportion of male children in the USA were born in hospitals and were circumcised [65] . The proportion of newborns that were circumcised annually reached 80% after World War II, peaked in the mid-1960s and has subsequently decreased. According to the National Hospital Discharge Survey, which documents circumcisions performed in hospitals but does not ascertain circumcisions performed outside of the hospital (e.g., for religious reasons), 65% of newborn boys were circumcised in 1999, and the overall proportion of newborns circumcised has remained stable from 1979 to 1999 [103] . The proportion of Black newborns who were circumcised rose over this period to approximately 65%, while the proportion of White newborns who were circumcised remained stable at 66%. Significant discrepancies in rates of circumcision exist between regions. While the proportion of newborns born in the Midwest who were circumcised increased from 74 to 81% between 1979 and 1999, the proportion of infants born in the West who were circumcised decreased over the same period, from 64% in 1979 to 37% in 1999, reflecting the increased proportion of Hispanic births. In another hospital discharge survey with different methodology (Healthcare Cost and Utilization Project National Inpatient Sample), newborn circumcision rates reportedly increased from 48% in 1988–1991 to 61% in 1997–2000. Circumcision was more common among newborns born to families of higher socioeconomic status, in the Northeast or Midwest, and among newborns who were Black [66] . Finally, in a series of national probability samples of adults surveyed during 1999–2004 as part of the National Health and Nutrition Examination Surveys, the overall prevalence of circumcision among adult males in the USA was 79% and varied by race/ethnicity (88% in non-Hispanic White men, 73% in non-Hispanic Black men, 42% in Mexican–Americans and 246
HIV Ther. (2009) 3(3)
50% in men of other races/ethnicities) [67] . The prevalence of circumcision among USA-born men decreased from the 1970s to the 1980s in all racial/ethnic categories. It should be noted that circumcision status may be subject to misclassification. In a study of adolescents¸ only 69% of circumcised and 65% of uncircumcised young men correctly identified their circumcision status as verified by physical exam [68] . In 1999, the American Academy of Pediatrics (AAP) issued a policy statement asserting that the available data at the time were insufficient to recommend routine neonatal MC. The Academy also stated “It is legitimate for the parents to take into account cultural, religious and ethnic traditions, in addition to medical factors, when making this choice” [69] . This position was reaffirmed by the Academy in 2005 following the report of the results of the first African clinical trial [70] . This policy has influenced reimbursement for and the practice of neonatal circumcision. In a 1995 review, 61% of circumcisions were paid for by private insurance, 36% were paid for by Medicaid and 3% were self-paid by the parents of the infant. Compared with infants of self-pay parents, those covered by private insurance were 2.5‑times as likely to be circumcised [71] . Since the 1999 AAP policy statement was issued, several states have eliminated Medicaid payments for circumcisions that were not deemed medically necessary and, when controlling for other factors, hospitals in states in which Medicaid covers routine MC had circumcision rates that were 24% higher than hospitals in states without such coverage [72] . However, the AAP has recently (2008) convened a panel to reconsider its circumcision policy in light of the African clinical trials and other data now available. The American Urological Association modified their previously neutral recommendation in 2007 and concluded that “While the results of studies in African nations may not necessarily be extrapolated to men in the USA at risk for HIV infection, the American Urological Association recommends that circumcision should be presented as an option for health benefits” [104] . Acceptability of male circumcision for HIV prevention in the USA It is not well understood whether American men at higher risk for HIV infection would be willing to undergo circumcision for partial HIV prevention, nor whether parents would be willing to have their infants circumcised for the purpose of reducing possible future HIV infection risk. future science group
Role of male circumcision in the prevention of HIV transmission in the USA In an analysis of interview data with selfreported HIV-negative MSM at gay pride events in 2006, uncircumcised respondents were asked about their willingness to be circumcised if it were proven to reduce risk of HIV infection among MSM [73] . Over half of uncircumcised MSM who were surveyed and 70% of Black MSM expressed willingness to be circumcised. The most commonly reported concerns about circumcision were postsurgical pain and wound infection. Further research regarding acceptability and feasibility of MC for high-risk heterosexual men is needed. To this end, a demonstration project of circumcision of men in the USA at high risk for heterosexual HIV acquisition is being funded by the CDC. In this study, acceptability of MC, HIV infection risk behaviors before and after circumcision, and other relevant attitudes and behaviors are being assessed. Surveys of medical providers, insurance payers and end-consumers (parents and adult men) are also being conducted by the CDC to assess acceptability and feasibility of MC for prevention of HIV infection and other adverse health conditions in the USA. Considerations in the role of male circumcision for HIV prevention in the USA In March 2007, shortly after publication of the final two clinical trial reports, the WHO and UNAIDS recommended that MC be recognized as an additional important intervention to reduce heterosexual acquisition of HIV infection among men in settings with high HIV prevalence and low circumcision rates [105] . For several reasons, however, the WHO/ UNAIDS recommendations are not directly applicable to the USA [74] . Policy on MC needs to be considered in light of the domestic USA HIV epidemic, prevailing norms regarding MC, feasibility, policy issues and cost–effectiveness while addressing relevant ethical concerns. The epidemiology of HIV infection in the USA differs considerably from that of regions prioritized by the WHO/UNAIDS recommendations and the sub-Saharan African areas where the randomized, circumcision trials were conducted. Most notably, the overall risk of HIV acquisition and the prevalence of HIV infection (0.45%) [63] is considerably lower in the USA than in the African clinical trials countries where the general population prevalence of HIV infection is 5–18% [106] . With regard to the risk for female–male transmission, the prevalence future science group
| Review
of HIV infection in women in the USA is only 0.22% [64] , whereas in the African clinical trial countries, the prevalence is equal or higher in women as compared with men [106] . While circumcision has only been proven to be effective in preventing female–male HIV transmission, only approximately 10% of transmission in the USA is attributed to this transmission route. Most transmission, an estimated 53% of incident cases in 2006, was through male–male sex, [61] for which circumcision could have, at best, only a limited impact as noted previously. Most men in the USA are already circumcised [68] , whereas in the African clinical trial sites, the prevalence of MC was 10–25%. Therefore, much of any possible prevention benefit has already been realized. However, it should be noted that the prevalence of MC is somewhat lower in USA racial and ethnic groups with higher rates of HIV infection. Moreover, to the extent that there is a prevention benefit to MC, that benefit is decreasing with the declining trend in infant circumcision. Taken together, the lower risk for female–male HIV transmission, the higher preexisting prevalence of MC and the higher cost of MC indicate that efforts to increase MC for HIV prevention would have less of an impact and be less cost effective in the USA than in sub‑Saharan Africa. In April 2007, the CDC held a consultation with clinicians, academics, community advocates and public health practitioners to solicit external expert advice on the potential role of male circumcision in the prevention of HIV infection and other health conditions in the USA. Views on the benefits of MC, as well as risks and downsides, were presented. Consultants suggested that the CDC consider that: Sufficient evidence exists to propose that adult/ adolescent heterosexually active men in the USA be informed about the significant but partial efficacy of circumcision in reducing risk for HIV acquisition and be provided with affordable access to voluntary, high‑quality surgical and risk-reduction counseling services;
n
Information about the potential health benefits and risks of MC should be presented to parents considering infant circumcision, and financial barriers to accessing MC should be removed;
n
Insufficient data exist about the impact (if any) of MC on HIV acquisition by homosexually active men and additional research is warranted.
n
www.futuremedicine.com
247
Review | Kilmarx, Kretsinger & Millett In formulating recommendations for the USA, the CDC is coordinating with academic medical societies (e.g., A AP, which, as mentioned previously, is reconsidering its ci rcumcision policy) and other federal agencies. A rigorous systematic literature review on the clinical risks and benefits (including sur gical outcomes, changes in penile sensation and sexual function, rates of other STDs, penile cancer, cervical cancer in female partners and urinary tract infection) is also being conducted. Draft recommendations are being published for public comment and peer review before being finalized. As health authorities move forward in determining what role circumcision may play from a public health perspective, individual men may wish to consider circumcision as an additional HIV prevention measure, but must recognize that circumcision: n Has only proven effective in reducing fema le –ma le HI V transmission in predominately heterosexual populations; n Confers only partial protection and should be considered only in conjunction with other proven prevention measures, such as condom use; n Does carry risks and costs that must be considered in addition to potential benefits; n May result in increased risk for either male–female or female–male HIV transmission before wound healing is complete. Conclusion MC has been shown to substantially reduce the risk of female–male transmission of HIV and is being implemented as a HIV prevention intervention in sub-Saharan African countries where MC prevalence is low and the risk of female–male HIV transmission is high. In the USA, however, the role of MC as an HIV prevention intervention will be limited because the risk of female–male HIV transmission is lower and most men are already circumcised. Additionally, there is not good evidence that MC prevents HIV transmission through male–male sex, the most common transmission mode in the USA. As the CDC, AAP and other organizations formulate recommendations for men and parents of newborn boys in the USA, it should be kept in mind that MC offers only partial protection for female–male HIV transmission and does carry risks and costs as does any surgical 248
HIV Ther. (2009) 3(3)
procedure. However, as discussed in this paper, there are other health benefits associated with MC, including prevention of sexually transmitted infections other than HIV. Future research, programmatic and surveillance activities should ensure access to accurate information to make evidence-based individual and policy decisions about MC, access to safe and affordable MC services when appropriate, and optimal use of MC to maximize health benefits while minimizing costs and risk. Future perspective Since only a minority of HIV transmission in the USA is attributable to insertive sex, MC is unlikely to play a major role in HIV prevention in this country. The CDC and relevant professional societies such as the AAP and the American Urological Association have issued or are developing recommendations for MC for prevention of HIV infection and other adverse health conditions. Parents will consider these recommendations, together with advice from healthcare providers and others, in weighing the risk and benefits in deciding whether or not to circumcise their male newborns. Cultural, religious and family factors are likely to continue to play a significant role in parents’ decision-making, and public and private healthcare reimbursement policies will influence overall infant circumcision rates. Uncircumcised heterosexual men at high risk for HIV infection may chose to be circumcised as an additional partially protective HIV prevention measure. Randomized, controlled clinical trials of MC for HIV prevention in MSM have been proposed which, if feasible, would provide specific guidance for that population in the future. Disclaimer The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the CDC.
Financial & competing interests disclosure The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. No writing assistance was utilized in the production of this manuscript. future science group
Role of male circumcision in the prevention of HIV transmission in the USA
| Review
Executive summary Biological plausibility of male circumcision for HIV prevention The inner mucosa of the foreskin is less keratinized than the external skin of the penis shaft and has a higher density of target cells for HIV infection close to the skin surface. The foreskin may be susceptible to traumatic small tears and disruptions during sexual intercourse, providing a portal of entry for HIV. The preputial sac environment may be conducive to viral survival. Higher rates of sexually transmitted diseases in uncircumcised men may increase susceptibility to HIV infection. International clinical trials of male circumcision for HIV prevention Three randomized, controlled trials in predominately heterosexual populations in sub-Saharan Africa were each terminated early because of a significantly reduced rate of HIV infection in circumcised men as compared with uncircumcised controls. The risk reduction ranged from 51 to 60%. Taking into account men who crossed over to the other arm of the study, the risk reduction ranged from 55 to 76%. Male circumcision & HIV transmission in men who have sex with men Any potential HIV preventive effect of circumcision for penile–anal sex is likely to accrue only to insertive partners and not to receptive partners, but the risk for HIV acquisition is substantially greater for the anal receptive partner than for the insertive partner. A meta-analysis of 15 studies found that male circumcision (MC) offered no protection from HIV infection among men who have sex with men. Other potential health benefits of male circumcision MC is associated with reduced rates of some other sexually transmitted infections, penile cancer, cervical cancer in female partners and infant urinary tract infections. Risks & adverse effects associated with male circumcision Reported neonatal complication rates of MC are low. The most common complications reported have been bleeding and infection. Complication rates for adult circumcisions in the three African clinical trials ranged from 2 to 4%, most commonly pain, bleeding, infection and unsatisfactory cosmesis. Most studies find no increase in sexual dysfunction in circumcised men. HIV infection & male circumcision in the USA The overall risk of HIV acquisition is considerably lower in the USA than in the African countries where the clinical trials were conducted. Only approximately 10% of HIV transmission in the USA is attributed to female–male transmission. Most transmission is through male– male sex for which MC has not been shown to be protective. Most men in the USA are already circumcised. Accordingly, MC for HIV prevention would have less of an impact and be less cost effective in the USA than in sub-Saharan Africa.
human foreskin and cervical tissue grown in explant culture. Am. J. Pathol. 161(3), 867–873 (2002).
Bibliography Papers of special note have been highlighted as: n of interest nn of considerable interest 1
Alanis MC, Lucidi RS: Neonatal circumcision: a review of the world’s oldest and most controversial operation. Obstet. Gynecol. Surv. 59(5), 379–395 (2004).
2
McCoombe SG, Short RV: Potential HIV-1 target cells in the human penis. AIDS 20, 1491–1495 (2006).
n
3
4
Describes the thinner keratin layer and greater proximity of Langerhans’ cells to the epithelial surface in the inner foreskin tissue as compared with other penile tissues. Donoval BA, Landay AL, Moses S et al.: HIV-1 target cells in foreskins of African men with varying histories of sexually transmitted infections. Am. J. Clin. Pathol. 125, 386–391 (2006). Patterson BK, Landay A, Siegel JN et al.: Susceptibility to human immunodeficiency virus-1 infection of
future science group
n
5
6
n
Describes the greater proportion of HIV-1 target cells and greater ex vivo susceptibility to HIV-1 infection in foreskin mucosa as compared with cervical mucosa or the external surface of the foreskin. Szabo R, Short RV: How does male circumcision protect against HIV infection? BMJ 320(7249), 1592–1594 (2000). Weiss HA, Thomas SL, Munabi SK, Hayes RJ: Male circumcision and risk of syphilis, chancroid, and genital herpes: a systematic review and meta-analysis. Sex. Transm. Infect. 82(2), 101–109 (2006). In this meta-analysis of observational data, risk of syphilis and chancroid infection was lower in circumcised men for. Herpes simplex virus type-2 risk was lower, but with borderline statistical significance.
www.futuremedicine.com
7
Tobian AA, Serwadda D, Quinn TC et al.: Male circumcision for the prevention of HSV-2 and HPV infections and syphilis. N. Engl. J. Med. 360(13), 1298–1309 (2009).
8
Telzak EE, Chiasson MA, Bevier PJ, Stoneburner RL, Castro KG, Jaffe HW: HIV-1 seroconversion in patients with and without genital ulcer disease: a prospective study. Ann. Intern. Med. 119(12), 1181–1186 (1993).
9
Halperin DT, Bailey RC: Male circumcision and HIV infection: 10 years and counting. Lancet 354 (9192), 1813–1815 (1999).
10
Weiss HA, Quigley MA, Hayes RJ: Male circumcision and risk of HIV infection in sub-Saharan Africa: a systematic review and meta-analysis. AIDS 14(15), 2361–2370 (2000).
n
In this meta-analysis of observational data on male circumcision (MC) and HIV-1 infection risk in sub-Saharan Africa, HIV-1 risk was significantly lower in circumcised men, particularly those at high risk for HIV infection.
249
Review | Kilmarx, Kretsinger & Millett 11
n
Siegfried N, Muller M, Volmink J et al.: Male circumcision for prevention of heterosexual acquisition of HIV in men. Cochrane Database Syst. Rev. 3, CD003362 (2003). This systematic review of observational studies found an epidemiological association between male circumcision and prevention of HIV, especially among high-risk groups.
assessment of men enrolled in a randomized controlled trial. PLoS ONE 3(6), E2443 (2008). 18
Krieger JN, Mehta SD, Bailey RC et al.: Adult male circumcision: effects on sexual function and sexual satisfaction in Kisumu, Kenya. J. Sex. Med. 5(11), 2610–2622 (2008).
19
Kigozi G, Watya S, Polis CB et al.: The effect of male circumcision on sexual satisfaction and function, results from a randomized trial of male circumcision for human immunodeficiency virus prevention, Rakai, Uganda. Brit. J. Urol. 101(1), 65–70 (2008).
12 Gray RH, Kiwanuka N, Quinn TC et al.:
Male circumcision and HIV acquisition and transmission: cohort studies in Rakai, Uganda. Rakai Project Team. AIDS 14(15), 2371–2381 (2000).
nn
14
n
15
nn
16
17
First of the three randomized, controlled clinical trials to be concluded. With 3274 men aged 18–24 years in South Africa randomized to immediate versus delayed MC, they found a 60% reduction in HIV infection risk. Bailey RC, Moses S, Parker CB et al.: Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomized controlled trial. Lancet 369, 643–656 (2007). This randomized, controlled clinical trial in Kenya included 2784 men aged 18–24 years and found a 53% reduction in HIV infection risk in men randomized to MC. Gray RH, Kigozi G, Serwadda D et al.: Male circumcision for HIV prevention in men in Rakai, Uganda: a randomized trial. Lancet 369, 657–666 (2007). This randomized, controlled clinical trial in Uganda included 4996 men aged 18–49 years and found a 51% reduction in HIV infection risk in men randomized to MC. The investigators also studied transmission from HIV-infected men to their partners in a related study. Bailey RC, Moses S, Parker CB et al.: The protective effect of male circumcision is sustained for at least 42 months: results from the Kisumu, Kenya Trial. Presented at: XVIII International AIDS Conference. Mexico City, Mexico, 3–8 August 2008. Mattson CL, Campbell RT, Bailey RC, Agot K, Ndinya-Achola JO, Moses S: Risk compensation is not associated with male circumcision in Kisumu, Kenya: a multifaceted
250
et al.: Sexual risk, nitrite inhalant use, and lack of circumcision associated with HIV seroconversion in men who have sex with men in the United States. J. Acquir. Immune Defic. Syndr. 39(1), 82–89 (2005). 29 Millett GA, Ding H, Lauby J et al.:
Circumcision status and HIV infection among Black and Latino men who have sex with men in 3 USA cities. J. Acquir. Immune Defic. Syndr. 15(46), 643–650 (2007). 30 Grulich AE, Hendry O, Clark E, Kippax S,
Kaldor JM: Circumcision and male-to-male sexual transmission of HIV. AIDS 15, 1188–1189 (2001).
20 Warner L, Ghanem KG, Newman DR,
Macaluso M, Sullivan PS, Erbelding EJ: Male circumcision and risk of HIV infection among heterosexual African–American men attending Baltimore sexually transmitted disease clinics. J. Infect. Dis. 199(1), 59–65 (2009).
13 Auvert B, Taljaard D, Lagarde E,
Sobngwi‑Tambekou J, Sitta R, Puren A: randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: the ANRS 1265 Trial. PLoS Med. 2(11), E298 (2005).
28 Buchbinder SP, Vittinghoff E, Heagerty PJ
n
21
Among 394 visits by African–American men with known HIV exposure to Baltimore sexually transmitted disease clinics, MC was associated with a 51% lower HIV infection prevalence. Wawer M, Kigozi G, Serwadda D et al.: Trial of male circumcision in HIV+ men, Rakai, Uganda: effects in HIV+ men and in women partners. Presented at: 15th Conference on Retroviruses and Opportunistic Infections. Boston, MA, USA, 3–6 February 2008.
31
32 Millett GA, Flores SA, Marks G, Reed JB,
Herbst JH: Circumcision status and risk of HIV and sexually transmitted infections among men who have sex with men: a meta-analysis. JAMA 300(14), 1674–1684 (2008); erratum 301(11), 1126–1129 (2009). n
22 Gray RH, Kiwanuka N, Quinn TC et al.:
Male circumcision and HIV acquisition and transmission: cohort studies in Rakai, Uganda. Rakai Project Team. AIDS 14(15), 2371–2381 (2000).
24 Vittinghoff E, Douglas J, Judson F et al.:
Prevention of HIV transmission in the UK: what is the role of male circumcision? Sex. Transm. Infect. 84(3), 158–160 (2008). 34 Vermund SH, Qian HZ: Circumcision and
HIV prevention among men who have sex with men: no final word. JAMA 300(14), 1698–1700 (2008). 35
Per-contact risk of human immunodeficiency virus transmission between male sexual partners. Am. J. Epidemiol. 150(3), 306–311 (1999). 25 Varghese B, Maher JE, Peterman TA,
Branson BM, Steketee RW: Reducing the risk of sexual HIV transmission: quantifying the per-act risk for HIV on the basis of choice of partner, sex act, and condom use. Sex. Transm. Dis. 29, 38–43 (2002). 26 Hart TA, Wolitski RJ, Purcell DW, Gómez C,
Halkitis P; Seropositive Urban Men’s Study Team. Sexual behavior among HIV-positive men who have sex with men: what’s in a label? J. Sex. Res. 40(2), 179–188 (2003). 27 Moskowitz DA, Rieger G; Roloff ME: Tops,
bottoms and versatiles. Sex. Marital. Ther. 23(3), 191–202 (2008).
HIV Ther. (2009) 3(3)
In this meta-analysis of 15 studies, overall, HIV infection risk was not decreased in circumcised men who have sex with men.
33 Macdonald A, Humphreys J, Jaffe HW:
23 Gray RH, Kigozi G, Serwadda D et al.: The
effects of male circumcision on female partners’ genital tract symptoms and vaginal infections in a randomized trial in Rakai, Uganda. Am. J. Obstet. Gynecol. 200(1), E1–E42 (2009).
Templeton DJ, Jin F, Mao L et al.: Reduced risk of HIV seroconversion among circumcised homosexual men who report a preference for the insertive role in anal intercourse. Presented at: Australasian Sexual Health Conference 2008. Perth, Australia, 15–17 September 2008.
n
Castellsagué X, Bosch FX, Muñoz N et al.: Male circumcision, penile human papillomavirus infection, and cervical cancer in female partners. N. Engl. J. Med. 346(15), 1105–1112 (2002). In this study, MC was associated with a reduced risk of penile human papillomavirus infection and, in the case of men with a history of multiple sexual partners, a reduced risk of cervical cancer in their female partners.
36 Sobngwi-Tambekou J, Taljaard D,
Nieuwoudt M, Lissouba P, Puren A, Auvert B: Male circumcision and Neisseria gonorrhoeae, Chlamydia trachomatis, and Trichomonas vaginalis: observations in the aftermath of a randomised controlled trial for HIV prevention. Sex. Transm. Infect. 85(2), 116–120 (2009) (Epub ahead of print).
future science group
Role of male circumcision in the prevention of HIV transmission in the USA 37 Auvert B, Sobngwi-Tambekou J, Cutler E
et al.: Effect of male circumcision on the prevalence of high-risk human papillomavirus in young men: results of a randomized controlled trial conducted in Orange Farm, South Africa. J. Infect. Dis. 199, 14–19 (2009). n
In this substudy of the randomized, controlled trial, high-risk human papillomavirus infection risk was 34% lower in circumcised men than in the uncircumcised control group.
38 Daling JR, Madeleine MM, Johnson LG
et al.: Penile cancer: importance of circumcision, human papillomavirus and smoking in in situ and invasive disease. Int. J. Cancer 116(4), 606–616 (2005).
48 Cold CJ, Taylor JR: The prepuce. BJU Int.
51
52
44 Fergusson DM, Lawton JM, Shannon FT:
Neonatal circumcision and penile problems: an 8‑year longitudinal study. Pediatrics 81, 537–541 (1988). 45
Paediatric Death Review Committee: Office of the Chief Coroner of Ontario. Circumcision: a minor procedure? Paediatr. Child Health 12(4), 311–312 (2007).
46 Kigozi G, Gray RH, Wawer MJ et al.:
The safety of adult male circumcision in HIV-infected and uninfected men in Rakai, Uganda. PLoS Med. 5(6), E116 (2008). 47 Bailey RC, Egesah O, Rosenberg S:
Male circumcision for HIV prevention: a prospective study of complications in clinical and traditional settings in Bungoma, Kenya. Bull. WHO 86(9), 669–677 (2008).
future science group
65
Collins S, Upshaw J, Rutchik S et al.: Effects of circumcision on male sexual function: debunking a myth? J. Urol. 167, 2111–2112 (2002).
66 Nelson CP, Dunn R, Wan J, Wei JT:
Senkul T, Iseri C, Sen B et al.: Circumcision in adults: effect on sexual function. Urology 63, 155–158 (2004).
54 Kahn JG, Marseille E, Auvert B:
55
Gray RH, Li X, Kigozi G et al.: The impact of male circumcision on HIV incidence and cost per infection prevented: a stochastic simulation model from Rakai, Uganda. AIDS 21(7), 845–850 (2007).
67 Xu F, Markowitz LE, Sternberg MR,
Aral SO: Prevalence of circumcision and herpes simplex virus type 2 infection in men in the United States: the National Health and Nutrition Examination Survey (NHANES), 1999–2004. Sex. Transm. Dis. 34(7), 479–484 (2007). 68 Risser JM, Risser WL, Eissa MA,
Cromwell PF, Barratt MS, Bortot A: Self-assessment of circumcision status by adolescents. Am. J. Epidemiol. 159(11), 1095–1097 (2004). 69 American Academy of Pediatrics: Task force
on circumcision. Circumcision policy statement. Pediatrics 103(3), 686–693 (1999). 70 American Academy of Pediatrics: AAP
publications retired and reaffirmed. Pediatrics 116, 796 (2005).
56 Schoen EJ, Colby CJ, To TT: Cost analysis of
neonatal circumcision in a large health maintenance organization. J. Urol. 175, 1111–1115 (2006).
71 Mansfield CJ, Hueston WJ, Rudy M:
Neonatal circumcision: associated factors and length of hospital stay. J. Fam. Pract. 41(4), 370–376 (1995).
57 van Howe RS: A cost-utility analysis of
neonatal circumcision. Med. Decis. Making 24, 584–601 (2004).
72 Leibowitz AA, Desmond K, Belin T:
Determinants and policy implications of male circumcision in the United States. Am. J. Public Health 99(1), 138–145 (2009).
58 Fox M, Thomson M: A covenant with the
status quo? Male circumcision and the new BMA guidance to doctors. J. Med. Ethics 31(8), 463–469 (2005). 59 Adler R, Ottaway MS, Gould S:
n
Circumcision: we have heard from the experts; now let’s hear from the parents. Pediatrics 107(2), E20 (2001). 60 Benatar M, Benatar D: Between prophylaxis
and child abuse: the ethics of neonatal male circumcision. Am. J. Bioeth. 3(2), 35–48 (2003). 61
(CDC): Subpopulation estimates from the HIV incidence surveillance system – United States, 2006. Morb. Mortal. Wkly Rep. 57(36), 985–989 (2008).
www.futuremedicine.com
In this nationally representative sample, hospitals in states in which Medicaid covers routine male circumcision had 24% higher circumcision rates than hospitals in states without such coverage.
73 Begley EB, Jafa K, Voetsch AC,
Heffelfinger JD, Borkowf CB, Sullivan PS: Willingness of men who have sex with men (MSM) in the United States to be circumcised as adults to reduce the risk of HIV infection. PLoS ONE 3(7), E2731 (2008).
Hall HI, Song R, Rhodes P et al.: Estimation of HIV incidence in the United States. JAMA 300(5), 520–529 (2008).
62 Centers for Disease Control and Prevention
Laumann EO, Masi CM, Zuckerman EW: Circumcision in the United States. Prevalence, prophylactic effects, and sexual practice. JAMA 277, 1052–1057 (1997). The increasing incidence of newborn circumcision: data from the nationwide inpatient sample. J. Urol. 173(3), 978–981 (2005).
Cost–effectiveness of male circumcision for HIV prevention in a South African setting. PLoS Med. 3(12), e517 (2006).
43 Christakis DA, Harvey E, Zerr DM,
Feudtner C, Wright JA, Connell FA: A trade-off analysis of routine newborn circumcision. Pediatrics 105, 246–249 (2000).
circumcision outcomes study: effect on erectile function, penile sensitivity, sexual activity and satisfaction. J. Urol. 167(5), 2113–2116 (2002).
et al.: Penile sensitivity and sexual satisfaction after circumcision: are we informing men correctly? Urol. Int. 75, 62–66 (2004).
42 Wiswell TE, Geschke DW: Risks from
circumcision during the first month of life compared with those for uncircumcised boys. Pediatrics 83(6), 1011–1015 (1989).
In: Ed Schoen, MD, on Circumcision. RDR Books, Berkeley, CA, USA (2005).
53 Masood S, Patel HRH, Himpson RC
41 Singh-Grewal D, Macdess J, Craig J:
Circumcision for the prevention of urinary tract infection in boys: a systematic review of randomized trails and observational studies. Arch. Dis. Child. 90(8), 853–858 (2003).
64 Schoen E: Introduction and overview.
50 Fink KS, Carson CC, DeVellis RF: Adult
40 Wiswell TE, Enzenauer RW, Holton ME,
Cornish JD, Hankins CT: Declining frequency of circumcision: implications for changes in the absolute incidence and male to female sex ratio of urinary tract infections in early infancy. Pediatrics 79(3) 338–342 (1987).
Green T: HIV prevalence estimates – United States, 2006. Morb. Mortal. Wkly Rep. 57(39), 1073–1076 (2008).
49 Sorrells ML, Snyder JL, Reiss MD
39 Schoen EJ, Oehrli M, Colby CJ et al.:
The highly protective effect of newborn circumcision against invasive penile cancer. Pediatrics 105, E36 (2000).
63 Campsmith ML, Rhodes P, Hall HI,
83(Suppl. 1), 34–44 (1999). et al.: Fine-touch pressure thresholds in the adult penis. BJU Int. 99(4), 854–869 (2007).
| Review
74
Sullivan PS, Kilmarx PH, Peterman TA et al.: Male circumcision for prevention of HIV transmission: what the new data mean for HIV prevention in the United States. PLoS Med. 4(7), E223 (2007).
251
Review | Kilmarx, Kretsinger & Millett Websites 101 Agency for Healthcare Research and Quality,
Healthcare Cost and Utilization Project (HCUP). Overview of the HCUP nationwide inpatient sample (2001). www.hcup-us.ahrq.gov/db/nation/nis/NIS_ Introduction_2001.jsp (Accessed 2 January 2009). 102 Centers for Medicare and Medicaid Services.
Federal Register (2006). www.cms.hhs.gov/HospitalOutpatientPPS/ HORD/list.asp#TopOfPage (Accessed 2 January 2009).
252
103 Trends in circumcisions among newborns.
www.cdc.gov/nchs/products/pubs/pubd/ hestats/circumcisions/circumcisions.htm (Accessed 2 January 2009). 104 American Urological Association circumcision
policy statement. www.auanet.org/content/guidelines-andquality-care/policy-statements/c/ circumcision.cfm (Accessed 2 January 2009). 105 New data on male circumcision and HIV
prevention: policy and program implications. http://data.unaids.org/pub/Report/2007/ mc_recommendations_en.pdf. (Accessed 30 December 2008).
HIV Ther. (2009) 3(3)
n
These recommendations that male circumcision be recognized as an additional important intervention to reduce heterosexual acquisition of HIV infection were issued soon after the second and third clinical trial results were published.
106 Joint United Nations Programme on
HIV/AIDS (UNAIDS): Report on the global HIV/AIDS epidemic. Geneva, Switzerland, 2008. http://data.unaids.org/pub/ EPISlides/2007/2007_epiupdate_en.pdf (Accessed 2 January 2009).
future science group
Role of male circumcision in the prevention of HIV transmission in the USA
CME
| Review
Considerations in the role of male circumcision in the prevention of HIV transmission in the USA
To obtain credit, you should first read the journal article. After reading the article, you should be able to answer the following, related, multiple-choice questions. To complete the questions and earn continuing medical education (CME) credit, please go to http://cme.medscape.com/CME/futuremedicine. Credit cannot be obtained for tests completed on paper, although you may use the worksheet below to keep a record of your answers. You must be a registered user on Medscape.com. If you are not registered on Medscape.com, please click on the New Users: Free Registration link on the left hand side of the website to register. Only one answer is correct for each question. Once you successfully answer all post-test questions you will be able to view and/or print your certificate. For questions regarding the content of this activity, contact the accredited provider,
[email protected]. For technical assistance, contact
[email protected]. American Medical Association’s Physician’s Recognition Award (AMA PRA) credits are accepted in the US as evidence of participation in CME activities. For further information on this award, please refer to http://www.ama-assn.org/ama/ pub/category/2922.html. The AMA has determined that physicians not licensed in the US who participate in this CME activity are eligible for AMA PRA Category 1 Credits™. Through agreements that the AMA has made with agencies in some countries, AMA PRA credit is acceptable as evidence of participation in CME activities. If you are not licensed in the US and want to obtain an AMA PRA CME credit, please complete the questions online, print the certificate and present it to your national medical association.
Activity evaluation: where 1 is strongly disagree and 5 is strongly agree. 1
2
3
4
5
The activity supported the learning objectives. The material was organized clearly for learning to occur. The content learned from this activity will impact my practice. The activity was presented objectively and free of commercial bias. 1.
All of the following statements about previous research into male circumcision and the risk for HIV infection are accurate, except:
£ A Ecologic observations have found lower rates of HIV infection in countries with higher £ B £ C £ D
2.
rates of circumcision Circumcision was most effective in preventing HIV infection among low-risk men in observational studies Three controlled trials were stopped early because of evidence of efficacy of circumcision in the prevention of HIV infection Randomized trials have suggested that circumcision can reduce the risk for HIV infection by 50–60%
Male circumcision will most likely reduce the risk for HIV infection among which of the following groups of individuals?
£ £ £ £
A
Women having vaginal intercourse with men
B
Men having vaginal intercourse with women
C
Men having receptive anal intercourse with men
D
Men having insertive anal intercourse with men
Table continued overleaf...
future science group
www.futuremedicine.com
253
Review | Kilmarx, Kretsinger & Millett 3.
Which of the following statements regarding adverse events and costs related to circumcision is most accurate?
£ A Dehiscence is the most common complication of circumcision in the neonatal period £ B The rate of complications was similar when comparing traditional practitioners with clinicians in Africa
£ C Complication rates among adults generally range between 2 and 4% £ D The cost of neonatal male circumcision in the USA is $200 4.
Which of the following statements regarding trends and attitudes toward male circumcision in the USA is most accurate?
£ A The proportion of circumcised newborns has increased dramatically since the 1960s £ B Mexican–Americans have lower rates of circumcision compared with non-Hispanic White £ C £ D
254
and non-Hispanic Black men The American Academy of Pediatrics now formally recommends universal male circumcision to reduce the transmission for HIV Only a small percentage of men who have sex with men would accept circumcision
HIV Ther. (2009) 3(3)
future science group