Bronchiolitis obliterans organizing pneumonia. Diagnosis by transbronchial biopsy. Z S Azzam, L Bentur, A H Rubin, O Ben-Izhak and G Alroy Chest 1993;104;1899-1901 The online version of this article, along with updated information and services can be found online on the World Wide Web at: http://chestjournal.chestpubs.org/content/104/6/1899
Chest is the official journal of the American College of Chest Physicians. It has been published monthly since 1935. Copyright1993by the American College of Chest Physicians, 3300 Dundee Road, Northbrook, IL 60062. All rights reserved. No part of this article or PDF may be reproduced or distributed without the prior written permission of the copyright holder. (http://chestjournal.chestpubs.org/site/misc/reprints.xhtml) ISSN:0012-3692
Downloaded from chestjournal.chestpubs.org by guest on July 15, 2011 © 1993 American College of Chest Physicians
BronchiolitisObliteransOrganizing Pneumonia* Diagnosis by Transbronchial Biopsy Zaher S. Azzam, M.D.; Lea Bentur, M.D.; Ami-Hay F. Rubin, M.D., FCC.?; Offer Ben-Izhak, and Gideon Airoy, M.D.
M.D.;
Transbronchial biopsy (TBB) has been considered to be inadequate for the diagnosis of bronchiolitis obliterans organizing pneumonia (BOOP). We describe herein two patients
with interstitial
diagnosis
of BOOP
pulmonary
was achieved
disease in whom the
by TBB.
The two patients
presented with progressive dyspnea, cough, tachypnea, and fine end-inspiratory crackles. The radiologic findings disclosed patchy alveolar infiltrates. Pulmonary function tests
showed
a restrictive
pattern
and decreased
diffusing
capacity The pathologic findings disclosed bronchioles, alveolar ducts, and alveoli infiltrated with mononuclear cells. The lumina
were obliterated
with fibroblasts
granulation tissue. Corticosteroid treatment significant
improvement.
Transbronchial
and loose
resulted in
biopsy
should
be
considered as a useful diagnostic tool for BOOP. (Chest 1993; 104:1899-1901) AST = aspartate
litis
aminotransferase;
obliterans
organizing
BOOP =
pneumonia;
CMV =
cytomegalovirus; Dco = diffusing capacity of carbon monoxide; EBV = Epstein-Barr virus; ESR = erythrocyte sedimentation
rate B
ronchiolitis
obliterans
organizing
pneumonia
(BOOP)
is
a clinicopathologic entity characterized by a subacute illness
with
loss present
shortness
of breath,
for a period
fever,
Spirometric studies show a restrictive ment of gas exchange. The radiologic ranging from few alveolar opacities densities.23 The bronchioles and ducts and alveoli are infiltrated
lymphocytes, disease,
malaise,
and weight
ranging from 3 to 6 months.' pattern findings
and impair are variable,
to diffuse reticulonodular the surrounding alveolar with mononuclear cells,
and plasma cells; with the progression
the air spaces
become
obliterated
of the
wi@j@fibroblasts
and granulation tissue.' Pathologic confirmatiop of BOOP is @
decreased diffusing capacity for carbon monoxide (Dco). Arterial blood gas levels showed hvpoxemia, with an increased alveolar arterial gradient (Table 1). Laboratory findings disclosed the following values: erythrocyte sedimentation rate (ESR), 20 mm/Is; hemoglobin level, 13.8 g/dl; leukocyte count, 8,200/mm3, with a normal differential cell count; platelet count, 397,000/mm3; BUN, 10 mgidl (normal range, 5 to 25 mg/dl); creatinine, 1 mg/dl (normal range, 0.5 to 1.3 mg/dl); potassium, 4.1 mEq/L (normal range, 3.5 to 5.3 mEqfL); sodium, 140 mEqfL (normal range, 136 to 147 mEqJL); lactate dehydrogen ase, 268 LUlL (normal range, 60 to 225 lU/L); alkaline phusphatase, 113 lU/L (normal range, 30 to 115 lUlL); serum aspartate amino transferase (AST), 724 lUlL (normal, 5-45 lU/L); angiotensin converting enzyme, 62 lUlL (normal, 8 to 52 lU/L); and IgG, 2,463 mg/dl (normal, 640 to 1,350 mg/dl). Levels of 1gM and IgA were normal. Levels of antinuclear antibody, anti-DNA antibody, rheu matoid factor, and anticardiolipin antibody were all normal; and complement levels were normal. Serologic assays for viral antibodies revealed no diagnostic rise for the Epstein-Barr virus (EBV), cytomegalovinis (CMV), adenovinus, influenza, or parainfluenza titers. Transbronchial biopsy (Fig 2) disclosed the characteristic polypoid fibrous-tissue plugs filling air spaces. In the surrounding air spaces, numerous foamy macrophages were evident. The interstitium showed thickened walls infiltrated by chronic inflammatory cells. With higher magnification (Fig 2), the air-space plug was composed of loose connective tissue with scattered spindle fibroblasts, a few plasma cells, and lymphocytes. The alveolar septa contained lym phocytes, macrophages, plasma cells, and type 2 pneumocytes. These pathologic findings were consistent with the diagnosis of BOOP Treatment with prednisone (60 mg/day) was initiated and resulted in significant clinical, physiologic, and radiologic improvement within 1 month; complete recovery was observed after 3 months (Table 1). The dose of prednisone was gradually tapered, and therapy was stopped after a year. CASE
2
A 66-year-old woman was admitted for progressive dyspnea accompanied by a nonproductive cough and weight loss of 4 kg over several days. The patient had had a preceding episode of influenza. Until then, she had been healthy except for mild osteoporosis. The physical examination revealed only tachycardia (108 beats per minute), tachypnea (26 breaths per minute), and diffuse bilateral fine end-inspiratory crackles. The chest x-ray film (Fig 3) showed bilateral patchy infiltrates in the lower lungs and linear opacities in the midlungs. Pulmonary function tests disclosed a mild restrictive
—¿
[email protected]'
important, as it implies a benign course and therapeutic response to corticosteroid therapy. Performing an open lung biopsy is usually recommended.' In this article, we describe two patients in whom the diagnosis of BOOP was achieved by transbronchial biopsy (TBB). CASE CASE
REPORTS
1
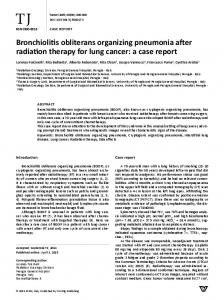
A 17-year-old patient was admitted with a nonproductive cough, progressive dyspnea, and weight loss of 3 months' duration. In the past, she had been in good health, and she denied smoking. Physical examination revealed tachycardia (120 beats per minute), tachypnea (24 breaths per minute), and end-inspiratory crackles in the lower lungs. The chest x-ray film and computed tomographic scan (Fig 1) showed bilateral alveolar infiltrates. Pulmonary function studies disclosed a restrictive pattern, with evidence of air trapping and *Fmm the Department of Medicine “¿A― (Drs. Azzam and Alroy), Pulmonary Division (Drs. Bentur and Rsuhin), and the Institute of Pathology (Dr. Ben-Izhak), Rambam Medical Center and Faculty of Medicine, Israel Institute of Technology, Haifa, Israel.
FIGuRE
1. Computed
tomogram
nous injection of contrast infiltrates (case 1).
material
with
enhancement
shows bilateral
after
CHEST / 104 / 6 / DECEMBER, 1993
Downloaded from chestjournal.chestpubs.org by guest on July 15, 2011 © 1993 American College of Chest Physicians
intrave
patchy alveolar
1899
Table 1—Pulmonary Function and Arterial Blood Gas LeveL, Before and After 3 Months of Treatment* 1Patient
%FVC,
l)ataPatient
%P0O/P,
%P00/P, %Before0After
2Before0After
0/P.
0/P,
L3.541.57443.561012.041.69832.54121FEy,, L2.971.64553.161061.671.40841.92116FEV/FVC%84.596.811588.810576.682.910878.71031W, L1.121.301161.241111.771.57891.3576TLC, L4.712.87614.66994.113.44843.8995RViTLC, %23.545.419326.611341.445.611034.883Do, msumnol/min/kPa/L2.031.18581.83901.971.09551.4172PaO,, . .54. .67.PaCO,, mm llg. mm llg. . .36. .39.p11. . .7.42. .7.46.11(X), , mnEq/L. . .24.
.
.87.
.
..
.
.55.
.
.
.38.
.
..
.
.36.
.
.
.7.45.
. ..
.
.7.40.
.
.
.
.22.
.
. .25.
..
.26.
5P predicted; 0, observed; FVC, forced vital capacity; RV, residual volume; TLC, total lung capacit@; pattern with decreased diffusing capacit@; Arterial blood gas levels fibroblasts; most patients have associated interstitial infiam showed mild hypoxensia (Table 1). mation.34 It is important to distinguish bronchiolitis oblit Lal)or,story fiusdings disclosed the following values: ESR, erans, the airflow disorder, from BOOP, the interstitial 90mm/h; normal complete blood cell count; hemoglobin level, 11.9 disorder. The former is occasionally idiopathic but generally g/dl; leokocvte count, 11,700/mm', with a normal differential cell occurs after inhalation of toxic fumes (SO2 or NO2) or after count; platelet count, 254,000/mm'; BUN, 14 mg/dl; creatinine, 0.9 a viral or mycoplasmal infection or is associated with mg/dl; l@)t@ussiuI1s. 3.5 IflEq/L; sodium, 136 mEq/L; lactate dehy connective tissue diseases. It has been associated with (lrogenass'. 313 IU/L; alkaline phosphatase, 24 lU/L; and AST, 33 penicillamine only in patients with rheumatoid arthritis, IU/L. Serum levels of immunoglohulin, antinuclear antibody anti The latter disorder, BOOP, is generally idiopathic but may l)NA antilsodv, rheumatoid factor, and anticardiolipin antibody be associated with connective tissue disorders (lupus of the were normal, and complement levels were nornial. Viral titers for EBV, CMV, adenovirus, influenza, and parainfluenza were negative lung), some types of viral infections, and a variety of for 1gM amid weakly positive (1/16) for lgG. Traosbroochial biopsy miscellaneous causes, such as amiodarone, bleomycin, or was performed and disclosed BOOP Therapy with prednisone (60 human immunodeficiency viral infection.@― Pathologic con rng) was initiated, and improvement was noticed within a month. firmation is important, as it implies a favorable prognosis After 3 months of treatment, the alveolar infiltrates resolved; and response to corticosteroid therapy.' More than 65 however, linear opacities in the midlungs persisted, and pulmonary percent of the patients have complete resolution; some may function tests showed mild reduction in Dco (Table 1). have resolution without therapy, some require low-dose maintenance
DISCUSSION Bronchiolitis
obliterans
copathologic
entity
organizing
pneumonia
first described
by Epler and his
colleagues' in 1985. Fifty patients were described; thens, diagnosis was made by open lung biopsy.
The distinguishing
histopathologic
is a clini in all of
feature of BOOP is the
therapy
with prednisone
others may have stabilization pulmonary
years,
and
with chronic symptoms
for several
and
dysfunction,
The benefit of cytotoxic agents in these cases has not yet been established. Death in idiopathic BOOP occurs in 5 percent of the cases. ‘¿@ Since the description by Epler et al'
filling of the alveolar and bronchiolar lumina by buds of loose connective tissue containing inflammatory cells and
Fe;uRu.:
2.
magnification 1900
Air
space
X 300).
with
BOOP
(hematoxylin-eosin,
original
FIGURE
3.
Chest
x—ray film
showing
diffuse
interstitial
opacities
(case 2).
BOOP Diagnosed by Transbronchial Biopsy (Azzam et a!)
Downloaded from chestjournal.chestpubs.org by guest on July 15, 2011 © 1993 American College of Chest Physicians
of 50 patients diagnosed by open lung biopsy, cited repeatedly that TBB is not recommended
the small specimens Our
own
since
and patchy nature of the disease.''@―
experience,
the diagnosis
it has been because of
as well of BOOP
as that
of others,―― differs,
was made
by TBB;
however
two criteria must be met: (1) the biopsy must contain both bronchiolar obliterans)
airway elements (proliferative and alveolar elensents (organizing
bronchiolitis pneumonia);
and (2) the clinical findings must be consistent with idio pathic BOOP, ie, influenza-like illness, crackles, patchy infiltrates
on the x-ray film, and physiologic
studies
showing
a decreased vital capacity and abnormal Dco. If these broad criteria are fulfilled, then TBB may be sufficient. In this article, we describe two patients with clinicophysiologic evidence of subacute interstitial pulmonary disease. It is interesting to note that patient 1 had transient abnormal results on hepatic function tests; recently, biochemical cholestasia was described in patients with BOOP.'2 In our
PersistentBronchopleuralFistula in a PatientWith Adult Respiratory DistressSyndrome* Treatment With Pressure-Controlled Ventilation Menachein
Lutmnanovitch,
PJonathan
F Cooper M.B.B.S.;
ment
airway
1074-82
in mechanically
a patient
with
pressures,
ARDSadult
ventilated
a traumatic
BPF,
patients.
pneumonia,
We and
may promote
respiratory
closure of the fistula. (Chest 1993; 104:1901-02) distress
syndrome;
BPF
bronchopleural fistula; CVP = central venous pressure; ETV = expired tidal volume; F1o2 = fractional inspired oxygen concen tration; I:Einspired to expired ratio; ITV=inspired tidal volume; MAP = mean airway pressure; P(A = a)02 = alveolar arterial oxygen difference; PAP peak airway pressure;
PCV= pressure-controlled ventilation; RR= ventilator respi ratory rate; SIMV = synchronized intermittent mandatory ven tilation; VCV = volume-controlled ventilation; V/Q = ventilation perfusion ratio; VD/VT = dead space to tidal volume ratio
REFERENCES
6 Epler CR. Bronchiolitis obliterans organizing pneumonia: defi nition and clinical features. Chest 1992; 102(suppl 1):2S-6S 7 Alegre-Martin J, Fernandez de Sevilla T, Garcia F, Fako V, Martinez-Vazquez JM. Three cases of idiopathic bronchiolitis obliterans organizing pneumonia. Eur Respir J 1991; 4:902-04 8 Van Theil RJ, Van der Burg 5, Croote AD, Nossent CD, Wills SH. Bronchiolitis obliterans organizing pneumonia and rheu matoid arthritis. Eur RespirJ 1991; 4:905—11 9 Costabel U, Cuzman J. BOOP: what is old, what is new? Eur Respir J 1991; 4:771-37 10 Costabel U, Teschler H, Schoenfeld B, Hartung W, Nusch A, Guzman J, et al. BOOP in Europe. In: Izumi T, ed. Proceedings of the International Congress on BOOP, Kyoto, Nov 29-Dec 1, 1990 11 Bartter T, Irwin RS, Nash C, Balikian JR Hollingsworth 1111. Idiopathic bronchiolitis obliterans organizing pneumonia with peripheral infiltrates on chest roentgenogram. Arch Intern Med 1989; 149:273-79 .12 Spiteri MA, Klenermnan F, Sheppard MN, Paddy 5, Clark TJK, Newman-Taylor A. Seasonal cryptogenic organizing pneumonia with biochemical cholestasis: a new clinical entits@ Lancet 1992; 340:280-84
M.B.B.Ch.
(PCV). This mode, by allowing the use of lower inspiratory
for diagnosis.
Med 1985; 312:152-58
M. Joynt, M.B.B.Ch.;
and II'terKraus,
adult respiratory distress syndrome (ARDS) who was suc cessfully ventilated with pressure-controlled ventilation
should be reserved for those times when the specimen from
2 McLoud TC, Epler CR, Colbs TV, Caensler EA, Carrington CB. Bronchiolitis obliterans. Radiology 1986; 159:1-8 3 Cordier JF, Loire R, Bruise J. Idiopathic bronchiolitis obliterans organizing pneumonia: definition of characteristic clinical pro files in usseries of 16 patients. Chest 1989; 96:999-1004 4 Cuerry-Force ML, Muller NL, Wright JL, \Viggs B, Cappin C, Pare FE, et al. A comparison of bronchiolitis obliterans with organizing pneumonia, usual interstitial pneumonia and small airway disease. Am Rev Respir Dis 1987; 135:705-12 5 Ingram RH Jr. Chronic bronchitis, emphysema amid airu'avs obstruction. In: Braunwald E, Isselbacher KJ, Petersdorf RC, Wilson JD, Martin JD, Fauci AS, eds. Harrison's principles of internal medicine. New York: McGraw-hill Book Cu, 1990;
problem
report
diagnosis of BOOP. The two patients responded dramatically to corticosteroid therapy. Therefore, it is concluded that TBB is a useful diagnostic tool in BOOP Open lung biopsy
1 Epler CR, Colby TV, MeLoud TC, Carrington CB, Caensler EA. Bronchiolitis obliterans organizing pneumonia. N EngI J
(;avin
Bronchopleural fistula (BPF) continues to present a treat
two patients, TBB yielded sufficient specimens for the
TBB is inadequate
M.D.;
P
ressure-controlled
ventilation
(PCV)
used
with
inverse
ratio ventilation may be a beneficial mode of ventilation in patients with adult respiratory distress syndrome ARDS.' It has been reported to improve oxygenation, ventilation, and allow decreased peak airway pressure (PAP) and lower
positive trolled
end-expiratory ventilation
pressure
is most
(PEEP).2
frequently
used
Pressure-con in conthination
with a prolonged inspiratory time and in patients with ARDS when conventional volume-controlled ventilation (VCV) is deemed to have failed. A bronchopleural fistula (BPF) may occur following trau matic lung laceration. High PAP during positive pressure ventilation is considered to be a major cause of barotrauma
and may prevent closure of a preexisting BPF.33 Conventional ventilation modalities known to reduce airway pressures and promote closure of the BPF are often not viable alternatives if ARDS coexists, as high fractional inspired oxygen (F1o2)
and airway pressures may be required to maintain adequate oxygenation and ventilation. Surgery may not be possible due to the impact of severe lung disease on gas exchange. CASE REPORT A 39-year-old black man weighing 75 kg, with no known history of cardiovascular or respiratory disease, was admitted to the hospital with multiple stal) wounds, involving the left upper chest and the axillary area. A left hemopneumothorax was drained and emergency surgery was performed, where the axillary vein was ligated and the axillary artery repaired. A combination of hypothermia, hemodynamic instabilit@çand the presence of a BPF necessitated postoperative ventilation and the patient was transferred to the ICU. At the time of admission, the patient was hemodynamically stable and was ventilated with a ventilator (Bird 8400) on synchronized intermittent mandatory *From the Intensive Care Unit, Bar,sgwanath Hospital, of the Witwatersrand, Soweto, South Africa.
University
CHEST / 104 / 6 / DECEMBER, 1993
Downloaded from chestjournal.chestpubs.org by guest on July 15, 2011 © 1993 American College of Chest Physicians
1901
Bronchiolitis obliterans organizing pneumonia. Diagnosis by transbronchial biopsy. Z S Azzam, L Bentur, A H Rubin, O Ben-Izhak and G Alroy Chest 1993;104; 1899-1901 This information is current as of July 15, 2011 Updated Information & Services Updated Information and services can be found at: http://chestjournal.chestpubs.org/content/104/6/1899 Cited Bys This article has been cited by 3 HighWire-hosted articles: http://chestjournal.chestpubs.org/content/104/6/1899#related-urls Permissions & Licensing Information about reproducing this article in parts (figures, tables) or in its entirety can be found online at: http://www.chestpubs.org/site/misc/reprints.xhtml Reprints Information about ordering reprints can be found online: http://www.chestpubs.org/site/misc/reprints.xhtml Citation Alerts Receive free e-mail alerts when new articles cite this article. To sign up, select the "Services" link to the right of the online article. Images in PowerPoint format Figures that appear in CHEST articles can be downloaded for teaching purposes in PowerPoint slide format. See any online figure for directions.
Downloaded from chestjournal.chestpubs.org by guest on July 15, 2011 © 1993 American College of Chest Physicians