Aug 15, 1995 ... video camera (Panasonic NV -M7) with a zoom lens, a video recorder (Mitsubishi
E7. Black Diamond), and a color monitor (Sony. Trinitron) (23 ...
Journal of Vestibular Research, Vol. 6, No.2, pp. 135-139, 1996 Copyright © 1996 Elsevier Science Inc. Printed in the USA. All rights reserved 0957-4271196 $15.00 + .00
ELSEVIER
0957-4271 (95)02013-6
Short Communication
EARLY DIAZEPAM TREATMENT FOLLOWING UNILATERAL LABYRINTHECTOMY DOES NOT IMPAIR VESTIBULAR COMPENSATION OF SPONTANEOUS NYSTAGMUS IN GUINEA PIG Jacelyn Martin,* Darrin P.D. Gilchrist,* Paul F. Smith, t and Cynthia L. Darlington* *Department of Psychology and the Neuroscience Research Centre, and the tDepartment of Pharmacology, School of Medical Sciences, University of Otago Medical School, Dunedin, New Zealand Reprint address: Dr. C.L. Darlington, Department of Psychology, University of Otago, Dunedin, New Zealand
0 Abstract- Diazepam and other benzodiazepines are sometimes used to alleviate vertigo and dizziness following labyrinthine surgery in humans. While the results of some previous studies have suggested that the administration of diazepam and other CNS depressant drugs following unilateral labyrinthectomy (UL) may impair the vestibuiar compensation process, the available evidence is unclear. The objective of the present experiment was to examine the effects of multiple injections of a high dose of diazepam (that is, 10 mg/kg ip) 30 min before and following UL (10 h or 10 and 20 h) on the static symptom, spontaneous ocular nystagmus (SN), in guinea pigs. Although diazepam-treated animals exhibited consistently lower average SN frequency compared to vehicle controls, neither SN frequency nor its rate of compensation were significantly different between the 2 groups. The time to complete SN compensation was also similar for the 2 groups, as estimated from the x intercepts derived from a linear regression analysis. These results suggest that even high doses of diazepam before and following UL do not result in an impairment of compensation of SN in guinea pig. 0 Keywords- unilateral labyrinthectomy; vestibular compensation; diazepam; benzodiazepines.
Diazepam, and other sedative/hypnotic drugs of the benzodiazepine class, are sometimes prescribed for patients suffering from dizziness and vertigo as a consequence of labyrin-
thine surgery, intractable vertigo, Meniere's disease, or cerebellar /brainstem lesions (for example, 1-3; see 4 for a review). The sedative actions of these drugs may reduce theseverity of the vestibular symptoms while, at the same time, providing a useful anxiolytic effect. Benzodiazepines have been demonstrated to impair vestibular reflex function (for example, 5,6), an effect that is probably mediated at least partially by their action at the benzodiazepine recognition site on GABAA receptor complexes within the vestibular nucleus complex (VN C) (7 -10; see 11 , 12 for recent reviews). Since benzodiazepines increase the affinity of the GABAA binding site for GABA, thereby potentiating its postsynaptic effect, benzodiazepines could be expected to increase inhibition in the VNC (7 ,8). However, because systemically administered benzodiazepines will affect all areas of the CNS with GABAA reany sympioms is
z.~ve:·se
side ef-
fects such as drowsiness and ataxia (see 13 for a review). The concern has been raised that treatment with benzodiazepines and other CNS depressant drugs following vestibular lesions may delay or impair vestibular compensation (for example, 2). However, experimental studies of the effects of diazepam on vestibular compensation have yielded unexpected results. Bern-
RECEIVED 15 August 1995; AccEPTED 6 September 1995.
135
J. Martin et al
136
stein and colleagues (3) reported that diazepam did not delay the recovery of resting activity in ipsilateral medial vestibular nucleus (MVN) neurons during vestibular compensation in cats; however, this study was largely qualitative in nature. Peppard (14) reported that daily diazepam administration for 16 days following unilateral labyrinthectomy (UL) had no appreciable effect on the compensation of directional vestibula-ocular reflex (VOR) asymFlohr and Luneburg that administration of the GABAA receptor agonist, muscimol, produced decompensation in compensated frogs. Although there is evidence for changes in GABA and GABAA receptors in the ipsilateral VNC during the development of vestibular compensation (for example, 16, 17), there is no substantial evidence for any changes in benzodiazepine binding sites ( 18). The question of whether administration of benzodiazepines following labyrinthine surgery reduces or delays the process of vestibular compensation is a clinically important one (2,3). Because the available diazepam studies have used only low diazepam doses (that is, 0.4 to 1.6 mg/kg/day (3~14)) and there has been no systematic quantitative analysis of the effects of diazepam on spontaneous nystagmus (SN), we decided to investigate the effects of a highly sedative dose of diazepam (that is, 10 mg/kg ip) on the compensation of SN in guinea pig. We chose to analyze SN frequency because it shows a consistent, linear decay in severity over time and is therefore amenable to quantitative analysis using linear regression (for example, 22). Our previous studies of the effects of diazepam on the guinea pig righting reflex have demonstrated that a 10 mg/kg ip diazepam dose produces a degree of sedation that is the equivalent of a highly sedating diazepam injection in humans (for example, 19,20).
Methods Fifteen male and female guinea pigs (250900 g) were used in this study. The animals were housed in pairs in an animal holding
room with a 12-h dark/light cycle; food and water were available ad libitum. On the day of surgery, the animals were transferred to the laboratory and housed singly for the remainder of the experiment. The animals were randomly divided into 4 groups: 1) diazepam (Valium 10, Roche, New Zealand) 10 mg/kg ip, 2 injections, one 30 min pre-UL and another at 9 to 11 h post-UL (n = 4 animals); 2) diazepam 10 mg/kg ip, 3 injeca second at 9 to 11 h , and che third at 19 to 21 h post-UL (n = 3) vehicle 2 mL/kg ip, 2 injections, one 30 min pre-UL and another at 9 to 11 h post-UL (n = 4); 4) vehicle 2 mL/kg ip, 3 injections, one 30 min pre-UL, a second at 9 to 11 h post-UL, and the third at 19 to 21 h postUL (n = 4). All injections were delivered in a 2 mL/kg volume ip. The vehicle consisted of 890Jo saline, 80Jo ethanol, and 30Jo sodium benzoate (that is, the vehicle for Valium 10, Roche). Groups 3 and 4 were designed to control for the effects of the vehicle in the diazepam injection schedules used in Groups 1 and 2. Groups 1 and 2 were initially intended to investigate !he effects of different durations of diazepam treatment. However, the results from the 2 diazepam conditions were not significantly different (p > 0.05, 2-factor ANOVA), and therefore the data from them were pooled (n = 7), as were the data from their respective control groups (n = 8). Prior to surgery, the animals were anesthetised using a 0.4 mL/kg im injection of fentazin (0.4 mg/mL fentanyl citrate, 58.3 mg/mL xylazine HCI, 3.2 mg/mL azaperone) (21). Wound margins and pressure points were infused with 2 OJo procaine, and heart rate was monitored using ECG electrodes inserted in the forelimb muscles. A right surgical UL was performed under microscopic control as described in detail previously (for example, 22). Following surgery, the would was sutured and the animal allowed to recover in light. All injections and measurements were made according to a strict double-blind protocol. The syringes and animals were coded so that neither the person injecting the solution nor the persons measuring the UL symptoms knew which animals were receiving diazepam and
Diazepam and Vestibular Compensation
which were receiving vehicle. SN frequency was measured at 10, 20, 30, 45, and 50 h postUL. SN frequency was quantified visually by counting the number of SN quick phases ("beats") in a 15-s interval, as defined by an electronic audiotimer. This procedure was repeated 5 times at each measurement time, and the means were calculated. All SN measurements were made without restraint but only when the animal's head was stationary, in order to avoid contamination of SN by VOR nystagmus. SN was also videotaped using a video camera (Panasonic NV -M7) with a zoom lens, a video recorder (Mitsubishi E7 Black Diamond), and a color monitor (Sony Trinitron) (23,24). At 10 and 20 h post-UL, measurements were made before the diazepam or vehicle injection. Mean SN was analysed using a 2-factor ANOVA with repeated measures on time (25). Factor A ('drug effect') was used to determine whether the SN frequency changed, irrespective of time; the interaction (AB), was used to evaluate drug effects on the rate of ~SN compensation. Factor B ('time') was always significant and will not be discussed further. Linear regression analysis was also performed and, using the equation, y!b -alb= x, the x intercept for each group was calculated as an estimate of time to complete SN compensation (25). The significance level was set at .05 for all comparisons.
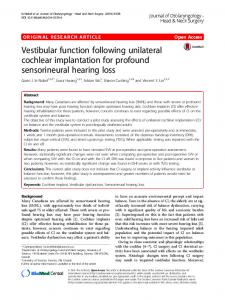
Results Animals that received diazepam injections showed lower average SN frequencies compared to the vehicle contra; group: however~ this difference was not significant (p > 0.0); see Figure Animals receiving diazepam were heavily sedated and often slept, although the duration of these effects varied considerably between different animals receiving the same duration of diazepam treatment. Although the rate of SN compensation appeared to be slower in the diazepam group, this effect was also nonsignificant (p > 0.05). Linear regression analysis showed that the 2 groups had similar x intercepts (vehicle group,
137
30
0
veh (n
e
dz (n
= 8)
= 7)
y y
= =
20.732 - 0.39071x 11.317 - 0.20830x
25
u Q)
1/)
20
,.. LC')
15 1/)
-ro C!J
e
10
c::
1/)
5
i 0
20
30
40
50
60
time post-UL (hs)
Figure 1. Compensation of spontaneous nystagmus frequency (SN, in beats/15 sec) in light. Open symbols represent means for the vehicle group (n = 8 guinea pigs in each case), closed symbols represent means for the diazepam group (n = 7 in each case). Bars represent± 1 SO of the mean. Lines are derived from linear regression analysis, the equations (y = a + bx) for which are shown in the legend.
53.2 h post-UL; diazepam group, 53.8 h postUL); therefore, they reached complete SN compensation at a similar time (see Figure 1).
Discussion The results of the present experiment demonstrate clearly that sedative doses of diazepam before and following UL in guinea pig do not result in an impairment of vestibular compensation of the static symptom, SN. Although average SN frequency was reduced in the diazepam group, probably due to the sedside effects 1requency nor iT_s ra.L.t ui' we1c significantly different from the vehicle group, and complete SN compensation was achieved at a similar time, that is, approximately 53 h post-UL. These results are in disagreement with the view that CNS depressant drugs necessarily impair vestibular compensation (2). Our results are in general agreement with those of Bernstein and colleagues (2) and Peppard (14); however, they further suggest that even high doses of diazepam can be used before and
J. Martin et al
138
following UL without impairment of SN compensation. Since diazepam has an approximately linear dose-response relationship with respect to its ataxic side effects, it is very unlikely that lower diazepam doses would produce greater impairment of SN compensation (20). Whether compensation of the dynamic VOR symptoms of UL would be impaired by diazepam remains to be tested; however, the results of Peppard (1 suggest that this is We are certain that the degree of compensation reached by the diazepam-treated animals at 53 h post-UL is not a result of remaining sedative effects from the last diazepam injection at 9 to 11 and/or 19 to 21 h post-UL. First, our previous studies have shown that the peak ataxic effects of diazepam in the guinea pig occur within 20 to 30-min following an ip injection and have largely disappeared within 5 h (20). This estimate includes the effects of active metabolites, because drugs administered ip are also subject to first-pass metabolism by the liver (20). Second, lower mammalian species metabolize diazepam and other benzodiazepines very rapidly, and pharmacokinetic studies have shown that the blood plasma half-life of diazepam in guinea pig is approximately 3 to 4 h (26). Therefore, given that drugs are generally eliminated within 4 to 5 half-lives, in the current study most of the diazepam would have been eliminated within 12 to 20 h after the last diazepam injection
(26); thus, by 40 h post-UL, even the animals that received 3 diazepam injections would have largely completed the process of elimination. Third, following the 50-h measurement, the diazepam animals did not show a gradual loss of compensation as might be expected if the symptoms were being suppressed by diazepam and the effect was gradually subsiding. Another potential explanation for the curJata ~s that t~1e diazepam doses employed were too low to adequately test the hypothesis that sedative doses of diazepam impair vestibular compensation. However, a high diazepam dose was deliberately chosen for the current experiment because it would eliminate the righting reflex and produce clear sedation (19,20). On a mg/kg basis for a 50 to 70 kg adult human, the 10 mg/kg dose that we used in guinea pigs is the equivalent of a 500 to 700 mg dose for a human. Since a single diazepam dose for a human rarely exceeds 40 mg (13), our diazepam doses were certainly high enough to evaluate the sedative effects of benzodiazepines on the compensation process. Acknowledgments- This research was supported by a Project Grant from the Health Research Council (HRC) of New Zealand (to CD and PS). DG was supported by a University of Otago Bridging Grant. We thank Andrew Sansom for assistance with some of the measurements. We thank Barry Dingwall and his staff for their excellent technical assistance.
REFERENCES l. McCabe BF, Sekitani T, Ryu JH. Drug effects on
2.
3. 4. 5. 6.
postlabyrinthectomy nystagmus. Arch Otolaryngol. 1973;98:310-3. Schaefer KP, Meyer DL. Compensation of vestibular lesions. In: Kornhuber HH, ed. Handbook of sensory physiology; Vol6: Part 2. Berlin: Springer-Verlag; 1974:463-90. Bernstein P, McCabe BF, Ryu JH. The effect of diazepam on vestibular compensation. Laryngoscope. 1973;80:267-72. Baloh RW. Approach to the dizzy patient. In: Baloh R, ed. Bailliere's Clin Neural. 1994;3:453-65. Blair SM, Gavin M. Modification of vestibula-ocular reflex induced in the macaque by diazepam. Arch Otolaryngol. 1979; 105:698-701. Padoan S, Korttila K, Magnusson M, Pyykko I, Schalen L. Reduction of gain and time constant of
7. 8. 9.
10.
vestibula-ocular reflex in man induced by diazepam and thiopental. J Vest Res. 1990;1 :97-104. Sekitani T, McCabe BF, Ryu JH. Drug effects on the medial vestibular nucleus. Arch Otolaryngol. 1971; 93:581-9. Ryu JH, McCabe BF. Effects of diazepam and dimenhydrinate on the resting activity of the vestibular neuron. Aerospace Med. 1974;45:1117-29. Zanni M, Giardino L, Toschi L, Galetti 0, Calza L. Distribution of neurotransmitters, neuropeptides, and receptors in the vestibular nuclei complex of the rat: an immunocytochemical, in situ hybridization and quantitative receptor autoradiographic study. Brain Res Bull. 1995;36:443-52. Hutchinson M, Darlington CL, Smith PF. The effects of long-term, low dose diazepam administration on guinea pig righting reflex latency and medial vestib-
Diazepam and Vestibular Compensation
11. 12. 13. 14. 15.
16.
17. 18.
ular nucleus neuronal activity. Pharmacal Biochem Behav. 1995;50:665-9. Smith PF, Darlington CL. The pharmacology of the vestibular system. In: Baloh R, ed. Bailliere's Clin Neurol. 1994;3:467-84. de Waele C, Muhlethaler M, Vidal PP. Neurochemistry of the central vestibular pathways. Brain Res Rev. 1995;20:24-46. Woods JH, Katz JL, Winger G. Benzodiazepines: use, abuse and consequences. Pharmacal Rev. 1992;44: 151-347. Peppard SB. Effect of drug therapy on compensation from vestibular injury. Laryngoscope. 1986;96: 878-98. Flohr H, Luneburg U. Neurotransmitter and neuromodulator systems involved in vestibular compensation. In: Berthoz A, Melvill Jones G, eds. Adaptive mechanisms in gaze control. Amsterdam: Elsevier; 1985:269-77. Dieringer N, Precht W. Mechanism of compensation for vestibular deficits in the frog; 2: Modifications of the inhibitory pathways. Exp Brain Res. 1979;36: 329-41. Thompson GC, Igarashi M, Cortez AM. GABA imbalance in squirrel monkey after unilateral vestibular end-organ ablation. Brain Res. 1986;370:182-5. Calza L, Giardino L, Zanni M, Galetti R, Parchi P, Galetti G. Involvement of cholinergic and GABAergic systems in vestibular compensation. In: Lacour M, Toupet M, Denise P, Christen Y, eds., Vestibular
139
19.
20.
21. 22.
23. 24.
25. 26.
compensation: facts, theories and clinical perspectives. Paris: Elsevier;1989:189-99. Scott SJ, Smith PF, Darlington CL. Quantification of the depressive effects of diazepam on the guinea pig righting reflex. Pharmacal Biochem Behav. 1994; 47:739-41. Smith PF, Darlington CL. Rapid tolerance to the depressive effects of diazepam on guinea pig motor control using divided doses. Pharmacal Biochem Behav. 1994;48:535-8. Sansom AJ, Smith PF, Darlington CL. Fentazin anesthesia for labyrinthine surgery in guinea pigs. J Vest Res. [In press]. Gilchrist DPD, Darlington CL, Smith PF. A doseresponse analysis of the beneficial effects of the ACTH-(4-9) analogue, Org 2766, on behavioural recovery following unilateral labyrinthectomy in guinea pig. Brit J Pharmacal. 1994;111:358-63. Flohr H, Luneburg U. Effects of ACTH-(4-10) on vestibular compensation. Brain Res. 1982;248: 169-73. Maclenann K, Smith PF, Darlington CL. Ginkgolide B accelerates vestibular compensation of spontaneous ocular nystagmus following unilateral labyrinthectomy in guinea pig. Exp Neurol. 1995; 131:273-8. Snedecor OW, Cochran WG. Statistical methods. 8th ed. Ames, Iowa: Iowa State University Press. Klotz U, Antonin KH, Bieck PR. Pharmacokinetics and plasma binding of diazepam in man, dog, rabbit, guinea pig and rat. J Pharmacal Exp Therap. 1976;199:67-73.