Send Orders for Reprints to
[email protected] Current Medicinal Chemistry, 2016, 23, 1-17
1
Evaluation of Novel Biomarkers of Acute Kidney Injury: The Possibilities and Limitations Branislava Medić¹, Branislav Rovčanin2, Katarina Savić Vujović1, Danilo Obradović3, Dušan Đurić4,5 and Milica Prostran1,* ¹Department of Pharmacology, Clinical Pharmacology and Toxicology, Faculty of Medicine, University of Belgrade, Serbia; 2Department of Human Genetics, Faculty of Medicine, University of Belgrade, Serbia; 3Department of Pathology, Faculty of Medicine, University of Belgrade, Serbia; 4 Department of Clinical Pharmacy, Faculty of Medical Sciences, University of Kragujevac, Serbia; 5Institute for Rehabilitation, Belgrade, Serbia
Please provide corresponding author(s) photograph
Abstract: Despite the recent findings concerning pathogenesis and novel therapeutic strategies, the mortality rate in patients with acute kidney injury (AKI) remains very high. Early detection of patients with impaired renal function may help to ensure more aggresive treatment and to improve clinical outcome. Serum creatinine is still gold standard of kidney injury, although it is well known as an insensitive and unreliable biomarker (for example, its concentration does not increase significantly until about half of the kidney function is lost). Considering these data, researches and clinicians are making great efforts in the past decade in order to discover and validate novel AKI biomarkers. Kidney injury molecule-1 (KIM-1), Neutrophil gelatinase-associated lipocalin (NGAL), Interleukin-18 (IL-18), Cystatin C (Cys-C) are some of new, promising markers of kidney damage which are currently in the focus of preclinical and clinical studies. Recent data suggest that some of these new biomarkers represent important parametars of acute tubular necrosis (ATN) and reliable predictors of development and prognosis of AKI. Beside that, monitoring of these markers could have significant importance for early diagnosis and clinical course, not only in patients with various forms of AKI and other renal diseases, but also in patients with cardiorenal syndrome, heart failure, cardiopulmonary bypass, cardiothoracical surgical interventions, in the pediatric emergency setting etc. The Aim of this review is to summarize the literature data concerning some new biomarkers, evaluate their role as well as their limitations in the early diagnosis and predict clinical outcome of some renal diseases.
Keywords: Acute kidney injure (AKI), novel renal biomarkers, kidney injury molecule (KIM-1), neutrophil gelatinase-associated lipocalin (NGAL), interleukin-18 (IL-18), cystatin C (Cys-C). 1. INTRODUCTION The term “acute kidney injury” (AKI) represents a wide range of structural and functional renal changes from mild alteration to complete organ failure with very high mortality rate. RIFLE classification [RiskInjury-Failure-Loss-End-stage kidney disease (ESKD)] was established by the Acute Dialysis Quality Initiative (ADQI) group in order to create uniform way to define,
detect and grade many different types of AKI1. After this, the AKIN criterion was created by the Acute Kidney Injury Network (AKIN) for further refinement of the definition of AKI [1]. Although significant progress has been made in understanding the origin, classification and the treatment of AKI, still approximately 2 million people 1
*Address correspondence to this author at the Department of Pharmacology, Clinical Pharmacology and Toxicology, Faculty of Medicine, University of Belgrade, Dr. Subotica starijeg 1, 11129 Belgrade, Serbia; Tel:/Fax: +381 11 3643 381; E-mail:
[email protected] 0929-8673/16 $58.00+.00
RIFLE classification: Risk (1.5 fold increase in serum creatinine - SCr or glomerul filtration rate – GFR decrease more than 25%; urine outout – UO less than 0.5 mg/kg/h for 6h), Injury (2 fold increase in SCr or GFR decrease more than 50%; UO less than 0.5 mg/kg/h for 12h), Failure (3 fold increase in SCr, GFR decrease more than 75% or acute rise in SCr more or equal as 0.5 mg/dl; UO less than 0.3 mg/kg/h for 24h or anuria for 12h), Loss (Complete loss of kidney function more than 4 weeks), ESKD (endstage kidney disease more than 3 months).
© 2016 Bentham Science Publishers
2 Current Medicinal Chemistry, 2016, Vol. 23, No. 8
worldwide pass away every year because of AKI and its consequences [2-4]. One of the principal reasons for this poor prognosis is too late detection of renal impairement and the fact that preventive strategies are most effective when started before oliguria. Serum creatinine is still gold standard of kidney injury although it is well known as an insensitive and unreliable biomarker: its concentration does not increase significantly until about half of the kidney function is lost. Beside that, its concentration does not differentiate structural kidney damage and functional hemodynamic triggers and could be unfluenced by numerous factors [5, 6]. In addition, few years ago, the American Society of Nephrology (ASN) in agreement with the National Health Institute (NHI) selected the AKI as area of interest which needed a more indepth study [7]. Considering these data, researches and clinicians worldwide are making great efforts in the past decade in order to discover and validate novel AKI biomarkers. The search for such biomarker(s) often specifies to as the ‘search for the renal troponin I’ [8]. The term biomarker (acronym for biological marker) is used to define a characteristic that can be measured and evaluated as normal biological process, pathological process or pharmacological response to therapeutic intervention [9, 10]. Soni et al. proposed that the ideal marker for AKI should be: 1) Non-invasive, 2) Easily detectable in accessible body samples (e.g. serum or urine), 3) Highly sensitive and specific for AKI, 4) Rapidly and reliably measurable, 5) Capable of early detection, 6) Predictor of AKI severity and prognosis, 7) Unaffected by other biological variables, 8) Inexpensive etc. [11]. Kidney injury molecule-1 (KIM-1), Neutrophil gelatinase-associated lipocalin (NGAL), Interleukin-18 (IL-18), Cystatin C (Cys-C) are some of new, and the most promising markers of kidney damage due to theirs translatability between preclinical and clinical trials. At the moment, these markers are in focus of preclinical and clinical studies. The Aim of this review is to summarize the literature data concerning novel biomarkers of acute kidney injury, evaluate their role as well as their limitations in the early diagnosis and predict clinical outcome. 2. KIDNEY INJURY MOLECULE-1 (KIM-1) 2.1. KIM-1: Molecular Structure The KIM-1 protein represents a membrane receptor for human hepatitis A virus (HHAV). It has one transmembrane domain and a short intracellular
Medić et al.
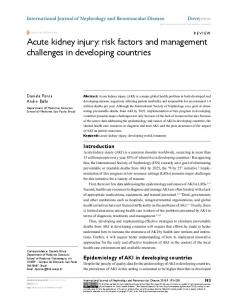
domain which contains a signaling protein for tyrosine phosphorylation (KIM-1b). It is believed that this molecule participates in the process of both kidney injury and healing [12]. KIM-1 is expressed at low to undetectable levels in the normal adult rat kidney, but significantly expressed by the epithelial proximal tubular cells in response to ischemic or toxic AKI [13]. Also, in situ hybridization indicated KIM-1 as a marker of proliferation and regeneration in proximal tubules [14]. Beside that, KIM-1 shows the ability to recognize and phagocytose dead cells presented in the postischemic kidney [15, 16]. 2.2. KIM-1 in Preclinical Studies Additional studies have been performed in order to examine the diagnostic role of KIM-1 in other models of AKI. Ichimura et al. examined tissue and urinary KIM-1 expression in a cisplatin-induced nephrotoxicity in rats and revealed KIM-1 as a superior marker than serum creatinine [14]. At this moment it is possible to measure KIM-1 concentration in tissue samples, urine and plasma/serume in a simple, rapid and accurate manner. Some recent studies confirmed KIM-1 as an important biomarker of AKI and acute tubular necrosis (ATN) and showed correlation between its concentration and the degree of renal dysfunction [17]. The latter preclinical study showed the diagnostic value of urinary KIM-1 as predictors of kidney tubular histopathological changes in rats [18]. Recently, research group from our project provided the first evidence that KIM-1 staining scores could be used as an indicator of the therapeutic benefit of different pharmacological agents in the experimental model of renal ischemia-reperfusion (I/R) injury. KIM-1 reliably confirmed that chloroquine affords an acute protective effect on kidney function and morphology as shown in Fig. (1) below [19]. In addition, KIM-1 has been approved by the US Food and Drug Administration as an AKI biomarker for preclinical drug development [20]. 2.3. KIM-1 in Clinical Studies Subsequent studies in adults suggested that urinary KIM-1 can discriminate patients with different types of acute tubular necrosis from those without AKI and predict adverse clinical outcomes such as dialysis requirement and mortality [21, 22, 25].
Evaluation of Novel Biomarkers of Acute Kidney Injury
Current Medicinal Chemistry, 2016, Vol. 23, No. 8
3
Fig. (1). The effects of chloroquine (0.3 mg/kg, i.v; 3 mg/kg, i.v.) on renal I/R injury and histological micrographs of renal tissues: KIM-1 staining score. Chloroquine in dose of 0.3 and 3 mg/kg, i.v. was injected 30 min before ischemia. Control groups, Sham+Saline and IR+ Saline received instead of drug i.v. bolus of 0.5 ml saline only (unpublished data from our laboratory project). Histological micrographs of renal tissues: kidney sections taken from Sham-operated rats or rats subjected to renal I/R injury. Kidney injury molecul-1 (KIM-1) staining. Original magnification ×200. Figures were randomly chosen from the series of at least 6 experiments (Panels A-D). Panel A: Sham-operated animals treated with saline only - absence of immunoreactivity for KIM-1. Panel B: Rats subjected to renal I /R injury, pretreated with chloroquine at 0.3 mg/kg, i.v. 30 min before ischemia – most of proximal and some distal tubules show mild staining for KIM-1. Panel C: Rats subjected to renal I /R injury, pretreated with chloroquine at 3 mg/kg, i.v. 30 min before ischemia - most of proximal and some distal tubules show moderate staining for KIM-1. Panel D: Rats subjected to renal I / R injury, pretreated with saline only - proximal and distal tubules show moderate to intensive positive KIM staining.
A rapid testing method for KIM-1 has been described, yielding semiquantitative results in just 15 minutes [23, 24]. Additional studies have confirmed that KIM-1 urinary concentration is upregulated in various kidney diseases including diabetic nephropathy, focal glomerulosclerosis, membranoproliferative glomerulonephritis, IgA nephropathy, even renal cell carcinoma [26]. Ichimura and his team has demonstrated that in ischemic injury KIM-1 expression is the most prominent in the S3 segment (i.e., the segment most susceptible to ischemic injury) [27].
2.3.1. KIM-1 in Cardiorenal Syndrome Clinical outcome of cardiorenal syndrome remains poor with a high mortality rate, partly because delayed diagnosis (on average 24h are after the event) [28]. Damman et al. recently confirmed KIM-1 as an excellent predictive marker for the detection of acute tubular injury in patients with chronic heart failure (HF) [29]. In this study, KIM-1 defeat other markers (such as NGAL and N-acetyl-β-D-glucosaminidase - NAG) and show how changes in volume status can lead to subclinical tubular injury that may be undetected by traditional biomarkers.
4 Current Medicinal Chemistry, 2016, Vol. 23, No. 8
Also, it is shown that urinary KIM-1 was also associated with increased risk of death or hospitalization, independent of GFR in patients with chronic heart failure [30]. 2.3.2. KIM-1 in Cardiac Surgery-Associated AKI Cardiac surgery-associated acute kidney injury (CSA-AKI) often includes coronary artery bypass grafting (CABG), surgery for valvular disease, as well as congenital heart surgery reportedly occurring in 30%-40% of cases [31]. It represents the second most common cause of AKI in the intensive care units and an independent predictor after cardiac surgery [32, 33]. Although pathogenesis of CSA-AKI is multifactorial and not fully understood, it is believed that it includes ischemia-reperfusion injury, inflammation and oxidative stress [34]. One of the initial studies regarding this issue showed KIM-1 levels increased significantly at both 2 hours and 24 hours postoperatively in patients with AKI after cardiopulmonary bypass (CPB) [35]. Koyner et al. compared the ability of several biomarkers to predict the progression of kidney damage in patients with elevated serum creatinine concentration levels who were underwent to cardiac surgery. KIM-1 was shown as a predictor of secondary importance in these situations [36]. Similar conclusion was shown by Hall et al. in their research that urine NGAL had the best results, followed by KIM-1 and IL-18 [37]. Recently, it has been shown that preoperative KIM1 urinary level is able to predict the development of AKI in adults undergoing to cardiac surgery [38]. Also, KIM -1 showed potential of being a good predictor for the development of AKI in pediatric cardiorenal injuries in emergency settings. [39]. Krawczeski et al. provided an evidence that KIM-1 at 12h following CPB independently correlated with CPB time and risk adjustment for congenital heart surgery score – (RACHS) [40]. Contrary to previous research, Hazle et al. did not confirm KIM-1 as a good prognostic factor in children. It was shown that KIM-1 poorly differentiated patients with either good or poor outcomes and was, therefore, removed from further analysis [41]. 2.3.3. KIM-1 in Organ Transplantation It is well known that KIM-1 values increase in acute graft rejection, but its role in delayed graft function (DGF) is still obscure [42].
Medić et al.
One small study linked urinary KIM-1 as a positive predictor of 14-wk and 1-yr posttransplantation serum creatinine in 20 brain death kidney donors before organ removal and compared these with living donors before nephrectomy [43]. In the first prospective study by Schröppel et al. KIM-1 was measured in biopsies of 30 living- and 85 deceased-donor kidneys and was correlated with histologic and clinical outcomes after transplantation. They showed that tubular KIM-1 expression correlated with GFR at the time of organ procurement, but did not correlate with the incidence of DGF [44]. Urinary KIM-1 expression is marked as a significant predictor of prognosis in patients who showed decline of renal function (group with high KIM-1 expression has significantly worse graft survival) [45]. Other study indicated KIM-1 as a potential marker in order to predict the need for renal replacement therapy (RRT) and 7-day mortality [46, 47]. 3. NEUTROPHIL GELATINASE-ASSOCIATED LIPOCALIN (NGAL) 3.1. NGAL: Molecular Structure Neutrophil gelatinase-associated lipocalin-NGAL (also known as lipocalin 2, siderocalin or oncogene 24p) is an immunological ubiquitous protein and one of the most promising and best-studied early biomarkers of AKI to date. It belongs to the family of lipocalins that are associated with many biological processes [48]. NGAL was initially discovered as a protein in granules of human neutrophils but also in different pathological conditions such as inflammation, sepsis, ischemia, renal damage, and cancer. Processes induced by NGAL include bacteriostasis, anti-apoptotic effects, and an enhanced proliferation of renal tubules, which constitute possible pathways of NGAL-mediated kidney protection in acute injury [49]. It exists in three different forms: as a 25-kDa monomer, 45-kDa homodimer and 135-kDa heterodimeric form [50]. Human NGAL exists predominantly in monomeric form and it is expressed in various tissues such as uterus, prostate, salivary gland, lung, trachea, stomach, colon, and kidney [51]. Understanding its role in human physiology and disease is rapidly increasing. 3.2. NGAL: Mechanism of Production and Preclinical Studies Although it is expressed in many human tissues, NGAL was found to be one of the most upregulated
Evaluation of Novel Biomarkers of Acute Kidney Injury
transcripts in the kidney early after acute injury, suggesting its role as an early marker of structural tubular damage [52, 53]. In the normal serum, as well in the urine, the concentration of NGAL is very low (∼20 ng/ mL at the steady state) and it is believed that its concentration is strongly upregulated in the distal part of the nephron promptly after acute kidney injury [54]. Paragas et al. found that NGAL values were increased and correlated with the degree of tubular damage only after 3 hours of kidney injury in mice. In addition, it was found that its production was located in the distal convoluted tubule and the collecting duct while the proximal tubule was involved in the process of plasma NGAL reabsorption [55]. Some other reports have showed that its expression is rapidly induced in other renal diseases such as diabetic nephropathy, nephritic syndrome, tubulointerstitial damage IgA nephropathy etc. [56, 57]. Mishra et al. conducted extensive examination of expression of numerous genes using cDNA microarray screening techniques in mouse model of AKI. NGAL was one of them whose expression was upregulated more than 10-fold within the first few hours after renal damage. Also, same group detected increased NGAL levels in the urine of rodents exposed to cisplatininduced nephrotoxicity, which is later confirmed in other studies [58]. Beside that, they reported that intravenous NGAL administered before, during, or after ischemia resulted in marked amelioration of the morphologic and functional changes in kidney in murine model of ischemiareperfusion injury. Proteomic studies have also revealed NGAL to be one of the earliest and most heavily induced proteins in the kidney after ischemic or nephrotoxic AKI in animal models. Importantly, NGAL protein is easily detected in the blood and urine soon after AKI in preclinical studies [59, 60]. In all animal models, NGAL levels reflected acute kidney injury more accurately when compared with serum creatinine. Also, urinary NGAL was the most sensitive indicator of gentamicin nephrotoxicity, compared to other biomarkers, with significant changes occurring within 24 hours, before any changes in serum creatinine were evident [61]. A study by Entin-Meer et al. in a rat model of cardiorenal syndrome demonstrated that elevated urine NGAL may potentially serve as an early non-invasive
Current Medicinal Chemistry, 2016, Vol. 23, No. 8
5
laboratory parameter for a left ventricular dysfunctionrelated renal injury [62]. These animal studies raised the interest of scientists and showed promising role of NGAL as an early and easily detected marker of ischemic and nephrotoxic kidney injury [63]. All these findings led to numerous clinical studies whose role was to evaluate NGAL as a non-invasive biomarker in human AKI. 3.3. NGAL in Clinical Studies 3.3.1. NGAL in the Prediction of AKI It is shown that NGAL is detected in human blood and urine at the earliest stages of AKI, 48-72 h before the rise in creatinine [38]. These findings have implicated NGAL as an early diagnostic and prognostic biomarker for AKI which confirmed many preclinical studies. Adiyanti et al. have demonstrated in cross-sectional study that AKI patients had significant NGAL increase in their urine and serum which anticipated increased serum creatinine level [64]. Also, large meta-analysis, conducted by Devarajan et al., identified that both urine and plasma NGAL values represented predictive factors for the development and severity of AKI, regardless of the clinical setting [65]. On the other hand, some authors gave an advantage to urinary NGAL as a reliable and fast predictive parameter of AKI in a variety of clinical conditions. Multicenter study of children with diarrhea-associated hemolytic uremic syndrome proved evidence that early urine NGAL levels predicted the severity of AKI and dialysis requirement with a high sensitivity. Additionally, urine NGAL was useful in the early diagnosis of postoperative AKI as well as in predicting the 6 months renal outcome after hepatobiliary surgery [66]. Sanjeevani et al. have recently published results of extensive multicenter study performed in order to examine correlation between biomarkers and final outcome such as need for renal replacement therapy (RRT), cardiovascular events, hospital stay, and death, independent of serum creatinine concentrations. They concluded that the use of NGAL urine levels along with panel of other renal biomarkers (such as KIM-1, IL-18, L-FABP, NHE-3) can improve the rate of early detection of AKI [67]. However, the largest study conducted among healthy children indicated significant gender and age differences in urinary NGAL and IL-18 values. In this study, Bennett et al. aimed to determine reference
6 Current Medicinal Chemistry, 2016, Vol. 23, No. 8
levels of the most promising novel biomarkers of AKI (including NGAL, KIM-1, IL-18, L-FABP) in a healthy pediatric population. That was the first study for the evaluation of the normal values of these markers in children, so that data could be essential in better understanding of some future results regarding this issue [68]. 3.3.2. NGAL in Cardiac Surgery-Associated AKI Data from animal and human heart tissues indicate a prognostic value for NGAL in a variety of cardiovascular diseases (CVDs), including heart failure, coronary disease and stroke [65]. Connection between NGAL and CVDs for the first time, was disclosed after cardiopulmonary bypass (CPB) in pediatric population. Mishra et al. reported that NGAL was a powerful and independent predictor of AKI after cardiac surgery [58]. Several studies investigated cardiac surgery patients and most of them showed increased levels of NGAL both in the blood and urine early (1-3h) after surgery [69, 70]. Another study measured KIM-1, NAG and NGAL in patients undergoing cardiac surgery in order to examine predictive power of these biomarker. Combining all three of them enhanced the sensitivity of early detection of postoperative AKI compared with individual biomarkers [71]. In chronic heart failure patients, both urine and serum NGAL levels were found to correlate with standard biomarkers of renal function (serum creatinine, cystatin C, and albuminuria) [72, 73]. Alvelos et al. [74] showed that higher plasma NGAL levels predict 3-year mortality independently of GFR in acute heart failure patients. Similar work by Damman et al. [29] pointed out the correlation between increased urinary NGAL expression and higher incidence of cardiovascular hospitalisation and mortality. AKI requiring dialysis represents the strongest independent risk factor for death in these patients. Beside that, it is assumed that NGAL could play a role in the prediction of exacerbation of renal function and the development of cardiorenal syndrome [75]. More recently, Daniels et al. [76] have provided further facts indicating that NGAL is indeed an independent marker of CVD. In neonates/children or adults with normal baseline renal function. Cruz et al. [65] demonstrated that systematic NGAL levels were higher in CVD patients than in non-CVD patients.
Medić et al.
Despite all previous studies, the recent metaanylysis in adults showed modest utility of NGAL to predict development of AKI after cardiac surgery. The best results were obtained after assesing this biomarker within 24 hours of cardiac surgery [77]. 3.3.3. NGAL in AKI after Kidney Transplantation AKI due to ischemia-reperfusion leads to DGF and complicates 4-10% of live donor and 5–50% of deceased donor kidney transplants. DGF represents an independent risk for chronic allograft nephropathy and graft loss [11]. A significant number of studies have identified significant relation of NGAL levels with poor clinical outcomes, including deterioration of AKI, need of renal replacement therapy, and mortality [78-81]. In this way it was possible to start earlier with an adequate and individual therapy, and thus to significantly reduce the consequent complications and costs of treatment. Cantaluppi showed that, in the first 24h following transplantation, patients with DGF demonstrated higher concentrations of plasma NGAL compared to non-DGF patients (delayed graft function) [82]. Similar findings were observed in the study conducted by RamírezSandoval et al. [83]. Conversely, in recently conducted prospective, multicenter study serum NGAL levels were not shown as indicator of delayed graft function in kidney recipients [84]. Nisula et al. demonstrated prognostic value of urine NGAL for renal replacement therapy, but not acute kidney injury and mortality in critically ill adult patients [85]. 3.3.4. NGAL in AKI in the Critical Care Setting Many of clinical studies in critically ill children and adults demonstrated NGAL as superior biomarker, because it revealed the occurence of complications approximately two days prior to the rise in serum creatinine [86, 87]. It is important to point out that the clinical symptomatology of AKI in critically ill septic patients was considerably less clear. This is reasonable considering the values of urine and blood NGAL in sepsis increased even without the existence of kidney damage. One explanation for this phenomenon is the fact that in sepsis, NGAL evolves not only from the injured kidney but also from leucocytes and liver. This fact may limit the diagnostic utility of NGAL in septic patients. For example, the study conducted by Yilmaz et al. detected increased NGAL levels in children with urinary tract infections in the absence of AKI [88].
Evaluation of Novel Biomarkers of Acute Kidney Injury
However, Di Somma et al. have recently established NGAL as a early risk marker of AKI development in the emergency department [89]. 4. INTERLEUKIN-18 (IL-18) 4.1. IL-18: Molecular Structure Interleukin-18 (IL-18) is a proinflammatory cytokine from the IL-1 family of cytokines which regulates innate and adaptive immunity [90]. His inactive, precursor form is synthesized by several tissues including monocytes, macrophages, and proximal tubular epithelial cells, and is processed into an active form by caspase-1 [91]. The levels of this biomarker are increased in numerous endogenous inflammatory processes (such as sepsis) and his role is detected in numerous renal diseases including ischemia/reperfusion, allograft rejection, autoimmune conditions, and malignancy [92]. Beside that, recent research has indicated that IL18 represents both mediator and biomarker of ischemic AKI. Its levels are increased about 6 hours after the ischemic injury and peaks approximately 12 hours later at values up to 25 times normal levels [93].
Current Medicinal Chemistry, 2016, Vol. 23, No. 8
7
a heterogenic group of critically ill children. Also, a cross-sectional study conducted in patients with acute respiratory distress syndrome who developed AKI, showed urine IL-18 levels significantly upregulated prior to the increase in serum creatinine. Contrary to this finding, IL-18 levels in subjects with urinary tract infection, chronic kidney disease, nephrotic syndrome, or prerenal azotemia were normal [100]. Liu et al. found that increased level of IL-18 in serume suggested poor outcome in hemodialysis patients independently of dysfunction of left ventriculi [101]. Recently published work concluded that plasma IL-18 concentrations taken 1 hour after reperfusion were predictive of AKI development after liver transplantation. On the other hand, other study proved evidence that IL-18 as a early biomarker had poor-tomoderate ability to predict AKI, RRT or 90-day mortality in the large cohort of critically ill patients [102]. The recent meta-analysis pointed out that these contradictory results may be due to fact that there is no clear consensus about the appropriate cutoff level of IL-18 to predict AKI and different thresholds have been reported by different studies [103].
4.2. IL-18 in Preclinical Studies
4.3.2. IL-18 in Cardiac Surgery-Associated AKI
Some of preclinical studies led to conclusion that the caspase-1-mediated production of IL-18 plays a deleterious role in AKI [94]. In addition, ischemic animal model in mice has been displayed IL-18 as possible candidate for an early marker of AKI. In these experiments, IL-18 was induced and cleaved in the proximal tubule, and subsequently easily detected in the urine [95].
One study in children undergoing cardiac surgery demonstrated increasing in urinary IL-18 levels 2 days before diagnosis by creatinine criteria [104]. In addition, early urine IL-18 measurements correlated with the severity of AKI as well as mortality. In contrast, study by Haase et al. did not find IL-18 to be a useful early predictor of AKI in adult patients underwent to cardiac surgery [105].
These preclinical observation showed that IL-18 in urine has a potential to be a marker of AKI in humans, as well. Recent studies have further evaluated IL-18 as a mediator of renal ischemia–reperfusion injury, inducing acute tubular necrosis and neutrophil and monocyte infiltration of the renal parenchyma [96].
In adults undergoing CPB, the early data on urinary IL-18 are less clear; one study has demonstrated a good predictive value for urinary IL-18, while a larger study did not [106].
4.3. IL-18 in Clinical Studies 4.3.1. IL-18 in Prediction of AKI More recently, numerous clinical studies have focused on the diagnostic accuracy of IL-18 level in predicting AKI [97-99]. Studies in human showed that IL-18 concentration increased in 24-48 hours prior to AKI based on RIFLE criteria. For example, the IL-18 urine level was predictor of development of AKI and correlated with its severity in
4.3.3. IL-18 in Critically Ill Patients In non-septic critically ill children IL-18 was shown as an independently predictive factor of outcome within 28 days. 64 In additional, it has been shown that urinary IL-18 levels increase within 2h after kidney injury in tandem with NGAL and continue to increase after NGAL levels begin to fall [107]. Later studies conducted on adults confirmed urinary IL-18 as a predictive biomarker which levels increased 2 days prior to a significant rise in serum creatinine [108].
8 Current Medicinal Chemistry, 2016, Vol. 23, No. 8
Althought recent study demonstratd IL-18 to be able to predict AKI in a cohort of 62 critically ill neonates, it should be pointed out that only non-septic patients were included and that the performance of IL-18 was inferior to urinary cystatin C [109]. 4.3.4. IL-18 in AKI After Kidney Transplantation It is well known that tubule cell injury frequently complicates deceased donor kidney transplants and in these patients urinary IL-18 has been examined as a biomarker for DGF [110]. Parikh, for example, showed that urinary NGAL and IL-18 were elevated in the first day after transplant in patients with DGF [110]. Also, he reported increased levels of IL-18 in patients with AKI of varying etiology, especially those with delayed renal allograft function and ischemic ATN [111]. In patients with acute rejection immunohistochemical studies showed strongly positive IL-18 staining, especially in proximal tubules. Beside that, even serum concentrations of IL18 showed significantly higher values in comparasion with patients with uncomplicated outcome of kidney transplantation and subjects with acute tubulointerstitial nephropathy [112]. The recent study provided evidence for both urinary IL-18 and clusterin 2 as useful biomarkers in screening patients with DGF within 4h of transplantation [113]. 5. CYSTATIN C (CYS-C) 5.1. Cys –C: Molecular Structure Cystatin C is a polypeptide chain with 120 amino acid residues and molecular weight of 13-kDa. It is produced by all nucleated cells at a constant rate. Also, it is considered to be one of the most important extracellular inhibitors of cysteine proteases [114]. Its pharmacokinetic properties make it easy to measure. Catabolism of cystatin C is mostly done in the kidneys; it is freely filtered by the glomerulus, completely reabsorbed by the proximal tubules, and is not secreted by the renal tubules [115]. Cystatin C may be determined in the serum, plasma, capillary blood and urine. Further, cystatin c as a marker of glomerular filtration rate is superior than serum creatinine because it is not affected by factors such as muscle mass, diet, sex, tubular secretion etc.
Medić et al.
Therefore, it has been suggested that Cys-C can be utilized in clinical situations where it is difficult to rely on creatinine measurements, such as the elderly, cachectic patients or those with numerous comorbidities [116]. Some investigations suggest that Cys-C could be a marker of inflammation because levels of C-reactive protein may increase its levels [117]. All these features promote cystatin C as a one of the most interesting biomarkers in preclinical and clinical research concerning kidney diseases. 5.2. Cys-C: Clinical Studies Clinical studies found that serum Cystatin C is more specific predictor than serum creatinine, especially in elders [118]. Urinary Cys-C levels have been found to be elevated in patients with tubular dysfunction known etiology [119]. In acute non–ST-elevation myocardial infarction, cystatin C was independently associated with mortality but not with the risk of subsequent myocardial infarction [120]. Recent studies have provided evidence that Cystatin C is an early marker of contrast-induced nephropathy in patients with sepsis in the intensive care unit, as well as moderate predictor of acute kidney injury in the early stage of traumatic hemorrhagic shock [121, 122]. Beside, it is shown that Cys-C is one of the markers that could can be used as diagnostic and predictive biomarkers for AKI in critically ill patients with sepsis [123]. Zappitelli et al. have shown that CysC-based definition of AKI is more strongly associated with urine interleukin 18 and kidney injury molecule 1 in children undergoing cardiac surgery [124]. They concluded that it is important to take in consideration defining AKI based on Cys-C in clinical care and future studies. On the other hand, recent studies by other author do not support replacing SCr by Cys-C to define AKI. They suggested that combined SCr-CysC-AKI definition could be a powerful tool and the best solution for the prediction of AKI in future studies [125, 126]. 6. LIVER-TYPE PROTEIN (L-FABP)
FATTY
ACID-BINDING
6.1. L-FABP: Molecular Structure 2
Clusterin (apolipoprotein J) is a 75 - 80 kDa disulfide-linked heterodimeric protein which is involved in many diseases related to oxidative stress, including neurodegenerative diseases, cancers, inflammatory diseases, aging etc. Some previous studies indicated urinary clusterin as a biomarker of kidney injury but its utility for prediction of graft dysfunction is unknown.
Fatty acid binding protein (FABP) is one of nine known cytosolic proteins ranging in size from 14-15 kDa Some studies suggest that FABPs are involved in numerous processesthe such as metabolism of fatty
Evaluation of Novel Biomarkers of Acute Kidney Injury
acids, intracellular trafficking of some substrates, modulation of specific enzymes of lipid metabolic pathwa and cell growth and differentiation [127]. FABP family members have highly conserved three dimensional structures and 22-73% amino acid sequence similarity. Fatty acid-binding protein 1 (FABP1), also known as liver-type fatty acid-binding protein (L-FABP) is a protein that is encoded by the FABP1 gene in humans. It belongs to family of carrier proteins for fatty acids and facilitates their transfer between extracellular and intracellular membranes [128]. FABP expression and urinary excretion have been described in several animal models of AKI, including ischemia-reperfusion-induced and cisplatin-induced AKI [129, 130]. These experiments showed that urine L-FABP levels increased before the increase in serum creatinine. 6.2. L-FABP: Clinical Studies Urine L-FABP was examined in clinical trials, where it was proven as a sensitive and predictive early biomarker of AKI in pediatric patients after cardiopulmonary bypass surgery [131]. KamijoIkemori et al. showed that the measurement of urinary L-FABP before cardiac catheterization procedure (CCP) and at 24 hours after CCP in patients with mild to moderate renal dysfunction may be an important indicator for risk stratification of onset of cardiovascular events [132]. It is shown that higher urinary L-FABP levels suggested poor outcome or the need for renal replacement therapy in patients with a rapid deterioration of renal function [133]. Other study measured urinary and serum levels of L-FABP in patients with sepsis. Urinary L-FABP levels were significantly higher in patients with septic shock than in those with severe sepsis without shock. Neverthless, serum L-FABP has not shown the ability to distinguish healthy patients with those one with septic shock or severe sepsis [134]. Moreover, the role of L-FABP was assessed in human kidney transplant patients. This research promoted urinary NGAL as a superior and more specific early biomarker of AKI in liver transplant recipients than L-FABP [135]. Recently conducted meta-analysis by Susantitaphong et al. assessed the performance of urinary L-FABP in AKI. The estimated sensitivity of urinary L-FABP for the diagnosis of AKI was 74.5%, for predicting dialysis requirement was
Current Medicinal Chemistry, 2016, Vol. 23, No. 8
9
69.1%, for in-hospital mortality 93.2%, while estimated values regarding specifity in the same conditions were 77.6%, 42.7% and 78.8%, respectively. They concluded that potential value of urinary L-FABP needs to be validated in larger studies and across a broader spectrum of clinical settings [136]. Urinary L-FABP seems to be promising both for the diagnosis of AKI and for the prediction of prognosis in critically ill patients [137]. Recently published paper indicated NGAL and L-FABP as a promising combination that may improve the diagnostic performance of AKI [138]. On the other hand, they presumed these biomarkers as potentially poor predictors for renal recovery after AKI [139]. In their recent study, Okazaki et al. concluded that other member from FABP family - urinary FABP4 could be a novel biomarker of glomerular damage, because its level was independently correlated with level of albuminuria and possibly predicted yearly decline of GFR population-based cohort design [140]. Predictive time course of novel renal biomarkers after AKI as well as their role in differential diagnosis, early detection and prognosis of AKI are shown in Fig. (2) and Table 1. 7. OTHER POTENTIAL BIOMARKERS Other potential biomarkers include urinary tubular enzymes (such as N-acetyl-β-glucosa-minidase (NAG), α-glutathione S-transferase, π-glutathione S-transferase, γ-glutamyltranspeptidase, alanine aminopeptidase, lactate dehydrogenase, alkaline phosphatase et al.) and urinary low-molecular-weight proteins (which include α1-microglobulin, β2-mic-roglobulin, retinol binding protein et al.) Although some of these biomarkers seem promising, preclinical and clinical evaluations are limited [141]. 8. LIMITATIONS OF NOVEL BIOMARKERS It should be noted that it is unlikely that a determination of the one single marker may be sufficient in many clinical entities with very complex pathogenesis and diverse etiology. For such complicated processes it is more appropriate creating so called “AKI Biomarker Panel”, to combine biomarkers to maximize the features and to minimize disadvantages of each of one [142]. It is important to note that most of these markers are not only associated with kidney damage, but also with the numerous conditions causing AKI (such as sepsis, diabetic nephropathy, systemic lupus erythematosus
10 Current Medicinal Chemistry, 2016, Vol. 23, No. 8
Medić et al.
Fig. (2). Predictive time course of novel renal biomarkers after AKI (adapted from reference [7]). Table 1. The role of novel biomarkers in differential diagnosis, early detection and prognosis of AKI (adapted from reference [6, 7]).
Evaluation of Novel Biomarkers of Acute Kidney Injury
Current Medicinal Chemistry, 2016, Vol. 23, No. 8
11
Table 2. Advantages and disadvantages of renal biomarkers (adapted from references [104, 137-141]).
etc.) and some chronic kidney disease (CKD). Beside that, another problem represents translating preclinical results to clinical practice [143]. At this point it seems that KIM-1 and NGAL represent a promising candidates for inclusion in the urinary “AKI Biomarker Panel”. One advantage of KIM-1 as a urinary biomarker is the fact that its expression seems to be limited to the injured or diseased kidney, although its value may affect number of other confounding variables [144]. KIM-1 in the kidney and urine is also induced in a variety of chronic proteinuric, inflammatory, and fibrotic disease states in humans [145]. NGAL is also one of the most promising novel biomarkers, because it is fast and powerful marker of active tubular pathology. Additionally, it is accurate marker of kidney disease progression. On the other hand, non-renal NGAL might adversely affect the diagnostic accuracy. Beside that, the lack of specific cut-off values for NGAL represents additional limitations to the widespread use of NGAL in clinical practice at the present time. It will be important in future studies to validate the sensitivity and specificity of urine and plasma NGAL in clinical samples.
Previous studies have shown IL-18 as marker that is more specific to ischemic AKI than other, but significantly influenced by numerous variables (endotoxemia, immunologic injury, cisplatin toxicity) and other pathophysiologic states, such as inflammatory arthritis, inflammatory bowel disease, and systemic lupus erythematosus. Generally, IL-18 represents marker with high specificity but low sensitivity for AKI diagnosis and correlated weakly with AKI duration or severity. Standardized platforms for the clinical measurement of urinary IL-18 remain to be developed and validated [146]. The most important advantages and disadvantages of each of described biomarker are indicated in above Table 2. CONCLUSION Numerous animal and human studies promoted some of novel biomarkers as a promising, new parameters for early diagnosis, monitoring of therapeutic effects and prediction of clinical outcome in kidney diseases, especially in AKI. Also, it should be pointed out that precise assessments of validity and establishing standards for the evaluation of these markers in pre-
12 Current Medicinal Chemistry, 2016, Vol. 23, No. 8
clinical and clinical studies are highly required. Finally, larger trials are necessary before a strong endorsement for the establishment of some of them in broader clinical use. LIST OF ABBREVIATIONS ADQI
=
acute Dialysis Quality Initiative
AKI
=
acute kidney injury
AKIN
=
acute Kidney Injury Network
ASN
=
American Society of Nephrology
ATN
=
acute tubular necrosis
CABG
=
coronary artery bypass grafting
CCP
=
cardiac catheterization procedure
CKD
=
chronic kidney disease
CPB
=
cardiopulmonary bypass
Medić et al.
CONFLICT OF INTEREST The authors confirm that this article content has no conflict of interest. ACKNOWLEDGEMENTS This work was supported by the Ministry of Education, Science and Technological Development of the Republic of Serbia (Project No. 175023). REFERENCES [1]
[2]
CSA-AKI =
cardiac surgery-associated acute kidney injury
CVD
=
cardiovascular disease
Cys-C
=
cystatin C
DGF
=
delayed graft function
GFR
=
glomerular filtration rate
HF
=
heart failure
HHAV
=
human hepatitis A virus
IL
=
interleukin
I/R
=
ischemia/reperfusion
kDa
=
kilodalton
KIM-1
=
kidney injury molecule-1
L-FABP
=
liver-type fatty acid-binding proteinas NHE3
NAG
=
N-acetyl-β-D-glucosaminidase
NGAL
=
neutrophil gelatinase-associated lipocalin
[9]
NHE -3
=
Na+/H+ exchanger isoform 3
[10]
NHI
=
National Health Institute
RACHS
=
risk adjustment for congenital heart surgery score
RIFLE
=
Risk-Injury-Failure-Loss-End-stage kidney disease (ESKD)
RRT
=
renal replacement therapy
SCr
=
serum creatinine
[3]
[4]
[5] [6] [7]
[8]
[11] [12]
[13]
Bellomo, R.; Ronco, C.; Kellum, J.A. The ADQI Workgroup: Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care., 2004, 8, R204- R212. Uchino, S.; Kellum, J.A.; Bellomo, R.; Doig, G.S.; Morimatsu, H.; Morgera, S.; Schetz, M.; Tan, I.; Bouman, C.; Macedo, E.; Gibney, N.; Tolwani, A.; Ronco, C. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA, 2005, 294, 813-818. Hoste, E.A.; Clermont, G.; Kersten, A.; Venkataraman, R.; Angus, D.C.; De Bacquer, D.; Kellum, J.A. RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis. Crit. Care., 2006, 10, R73. Ali, T.; Khan, I.; Simpson, W.; Prescott, G.; Townend, J.; Smith, W.; Macleod, A. Incidence and outcomes in acute kidney injury: a comprehensive population-based study. J. Am. Soc. Nephrol., 2007, 18, 1292-1298. Bellomo, R.; Kellum, J.A.; Ronco, C. Defining acute renal failure: physiological principles. Intens. Care. Med., 2004, 30, 33-37. Coca, S.G.; Parikh, C.R. Urinary biomarkers for acute kidney injury: perspectives on translation. Clin. J. Am. Soc. Nephrol., 2008, 3, 481-490. Taub, P.R.; Borden, K.C.; Fard, A.; Maisel, A. Role of biomarkers in the diagnosis and prognosis of acute kidney injury in patients with cardiorenal syndrome. Expert. Rev. Cardiovasc. Ther., 2012, 10(5), 657-667. Dent, C.; Ma, Q.; Dastrala, S.; Bennett, M.; Mitsnefes, M.M.; Barasch, J.; Devarajan, P. Plasma neutrophil gelatinase-associated lipocalin predicts acute kidney injury, morbidity and mortality after pediatric cardiac surgery: A prospective uncontrolled cohort study. Crit. Care., 2007, 11, R127. Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther., 2001, 69, 89-95. Singhal, N,.; Saha, A. Bedside biomarkers in pediatric cardio renal injuries in emergency. Int. J. Crit. Illn. Inj. Sci., 2014, 4(3), 238-246. Soni, S.; Ronco, C.; Katz, N.; Cruz, D.N. Early diagnosis of acute kidney injury: the promise of novel biomarkers. Blood. Purif ., 2009, 28, 165-174. Bailly, V.; Zhang, Z.; Meier, W.; Cate, R.; Sanicola, M.; Bonventre, J.V. Shedding of kidney injury molecule-1, a putative adhesion protein involved in renal regeneration. J. Biol. Chem., 2002, 277, 39739-39748. Ichimura, T.; Bonventre, J.V.; Bailly, V.; Wei, H.; Hession, C.A,.; Cate, R.L.; Sanicola, M. Kidney injury molecule-1 (KIM-1), a putative epithelial cell adhesion molecule containing a novel immunoglobulin domain, is up-regulated in
Evaluation of Novel Biomarkers of Acute Kidney Injury
[14] [15] [16]
[17]
[18] [19]
[20]
[21]
[22]
[23]
[24]
[25]
renal cells after injury. J. Biol. Chem., 1998, 273, 41354142. Ichimura, T.; Brooks, C.R., Bonventre, J.V. Kim-1/Tim-1 and immune cells: shifting sands. Kidney. Int., 2012, 81, 809-811. Bonventre, J.V. Kidney injury molecule-1 (KIM-1): A urinary biomarker and much more. Nephrol. Dial. Transplant., 2009, 24, 3265-8. Ichimura, T.; Asseldonk, E.J.; Humphreys, B.D.; Gunaratnam, L.; Duffield, J.S.; Bonventre, J.V. Kidney injury molecule-1 is a phosphatidylserine receptor that confers a phagocytic phenotype on epithelial cells. J. Clin. Invest., 2008, 118, 1657-1668. Kramer, A.B,; van Timmeren, M.M.; Schuurs, T.A.; Vaidya, V.S.; Bonventre, J.V.; van Goor, H.; Navis, G. Reduction of proteinuria in adriamycin-induced nephropathy is associated with reduction of renal kidney injury molecule (Kim-1) over time. Am. J. Physiol. Renal. Physiol., 2009, 296(5), F1136-45. Martensson, J.; Martling, C.R.; Bell, M. Novel biomarkers of acute kidney injury and failure: clinical applicability. Br. J. Anaesth., 2012, 109 (6), 843-50. Todorović. Z.; Medić, B.; Basta-Jovanović, G.; Radojević, Š.S.; Stojanović, R.; Rovčanin, B.; Prostran, M. Acute pretreatment with chloroquine attenuates renal I/R injury in rats. PloS One 2014, 9(3), e92673. Dieterle, F.; Sistare, F.; Goodsaid, F.; Papaluca, M.; Ozer, J.S.; Webb, C.P.; Baer, W.; Senagore, A.; Schipper, M.J.; Vonderscher, J.; Sultana, S.; Gerhold, D.L.; Phillips, J.A.; Maurer, G.; Carl, K.; Laurie, D.; Harpur, E.; Sonee, M.; Ennulat, D.; Holder, D.; Andrews-Cleavenger, D.; Gu, Y.Z.; Thompson, K.L.; Goering, P.L.; Vidal, J.M.; Abadie, E.; Maciulaitis, R.; Jacobson-Kram, D.; Defelice, A.F.; Hausner, E.A.; Blank, M.; Thompson, A.; Harlow, P.; Throckmorton, D.; Xiao, S.; Xu, N.; Taylor, W.; Vamvakas, S.; Flamion, B.; Lima, B.S.; Kasper, P.; Pasanen, M.; Prasad, K.; Troth, S.; Bounous, D.; Robinson-Gravatt, D.; Betton, G.; Davis, M.A.; Akunda, J.; McDuffie, J.E.; Suter, L.; Obert, L.; Guffroy, M.; Pinches, M.; Jayadev, S.; Blomme, E.A.; Beushausen, S.A.; Barlow, V.G.; Collins, N.; Waring, J.; Honor, D.; Snook, S.; Lee, J.; Rossi, P.; Walker, E.; Mattes, W. Renal biomarker qualification submission: a dialog between the FDA-EMEA and Predictive Safety Testing Consortium. Nat. Biotechnol., 2010, 28, 455462. van Timmeren, M.M.; van den Heuvel, M.C.; Bailly, V.; Bakker, S.J.; van Goor, H.; Stegeman, C.A. Tubular kidney injury molecule-1 (KIM-1) in human renal disease.. J. Pathol., 2009, 212, 209-17. Liangos, O.; Perianayagam, M.C.; Vaidya, V.S.; Han, W.K.; Wald, R.; Tighiouart, H.; MacKinnon, R.W.; Li, L.; Balakrishnan, V.S.; Pereira, B.J.; Bonventre, J.V.; Jaber, B.L. Urinary N-acetyl-beta-(D)-glucosaminidase activity and kidney injury molecule-1 level are associated with adverse outcomes in acute renal failure. J. Am. Soc. Nephrol., 2007, 18, 904-12. Coca, S.G.; Yalavarthy, R.; Concato, J.; Parikh, C.R. Biomarkers for the diagnosis and risk stratification of acute kidney injury: a systemic review. Kidney. Int., 2008, 73, 1008-1016. Vaidya, V.S.; Ford, G.M.; Waikar, S.S.; Wang, Y.; Clement, M.B.; Ramirez, V.; Glaab, W.E.; Troth, S.P.; Sistare, F.D.; Prozialeck, W.C.; Edwards, J.R.; Bobadilla, N.A.; Mefferd, S.C.; Bonventre, J.V. A rapid urine test for early detection of kidney injury. Kidney. Int., 2009, 76, 108-114. Todorović, Z.; Prostran, M.; Nešić, Z.; Stojanović, R.; Stojanov, M. The influence of drugs on biochemical markers of ischemia-reperfusion injury. In: The. Analysis. of. Pharma-
Current Medicinal Chemistry, 2016, Vol. 23, No. 8
[26]
[27]
[28]
[29]
[30]
[31] [32]
[33]
[34]
[35]
[36]
[37]
[38]
[39]
[40]
13
cologically. Active. Compounds. and. Biomolecules. in. Real. Samples; Injac, ed. ; Transworld Research Network: Kerala (India), 2009, pp. 217-238. Lucarelli, G.; Mancini, V.; Galleggiante, V.; Rutigliano, M.; Vavallo, A.; Battaglia, M.; Ditonno, P. Emerging urinary markers of renal injury in obstructive nephropathy. Biomed. Res. Int., 2014, 2014, 303298. Ichimura, T.; Hung, C.C.; Yang, S.A.; Stevens, J.L.; Bonventre, J.V. Kidney injury molecule-1: a tissue and urinary biomarker for nephrotoxicant-induced renal injury. Am. J. Physiol. Renal. Physiol., 2004, 286, 552-563. Lucarelli, G.; Ditonno, P.; Bettocchi, C.; Vavallo, A.; Rutigliano, M.; Galleggiante, V.; Larocca, A.M.; Castellano,G.; Gesualdo, L.; Grandaliano, G.; Selvaggi, F.P.; Battaglia, M. Diagnostic and prognostic role of preoperative circulating CA 15-3, CA 125, and beta-2 microglobulin in renal cell carcinoma. Dis. Markers, 2014, 2014, 689795. Damman, K.; Masson, S.; Hillege, H.L.; Maggioni, A.P.; Voors, A.A.; Opasich, C.; van Veldhuisen, D.J.; Montagna, L.; Cosmi, F.; Tognoni, G.; Tavazzi, L.; Latini, R. Clinical outcome of renal tubular damage in chronic heart failure. Eur. Heart. J ., 2011, 32(21), 2705-12. Ghatanatti, R.; Teli, A.; Tirkey, S.S.; Bhattacharya, S.; Sengupta, G.; Mondal, A. Role of renal biomarkers as predictors of acute kidney injury in cardiac surgery. Asian. Cardiovasc. Thorac. Ann.,. 2014, 22(2), 234-41. Bellomo, R.; Auriemma, S.; Fabbri, A.; The pathophysiology of cardiac surgery-associated acute kidney injury (CSA-AKI). Int. J. Artif. Organs., 2008: 166-178. Karkouti, K.; Wijeysundera, D.N.; Yau, T.M.; Callum, J.L.; Cheng, D.C.; Crowther, M.; Dupuis, J.Y.; Fremes, S.E.; Kent, B.; Laflamme, C.; Lamy, A.; Legare, J.F.; Mazer, C.D.; McCluskey, S.A.; Rubens, F.D.; Sawchuk, C.; Beattie, W.S. Acute kidney injury after cardiac surgery: focus on modifiable risk factors. Circulation 2009, 119, 495-502. Mao, H.; Katz, N.; Ariyanon, W.; Blanca-Martos, L.; Adýbelli, Z.; Giuliani, A.; Danesi, T.H.; Kim, J.C.; Nayak, A.; Neri, M.; Virzi, G.M.; Brocca, A.; Scalzotto, E.; Salvador, L.; Ronco, C. Cardiac Surgery-Associated Acute Kidney Injury. Cardiorenal. Med., 2013, 3, 178-199. Haase, M.; Bellomo, R.; Haase-Fielitz, A. Novel Biomarkers, Oxidative Stress, and the Role of Labile Iron Toxicity in Cardiopulmonary Bypass-Associated Acute Kidney Injury. J. Am. Coll. Cardiol 2010, 55(19), 2024-33. Han, W.K.; Waikar, S.S.; Johnson, A.; Curhan, G.C.; Devarajan, P.; Bonventre, J.V. Urinary biomarkers for early detection of acute kidney injury. J. Am. Soc. Nephrol., 2006, 17, 403A. Koyner, J.L.; Vaidya, V.S.; Bennett, M.R.; Ma, Q.; Worcester, E.; Akhter, S.A.; Raman, J.; Jeevanandam, V.; O'Connor, M.F.; Devarajan, P.; Bonventre, J.V.; Murray, P.T. Urinary biomarkers in the clinical prognosis and early detection of acute kidney injury. Clin. J. Am. Soc. Nephrol., 2010, 5, 2154-2165. Hall, I.E,; Coca, S.G.; Perazella, M.A. Risk of Poor Outcomes with Novel and Traditional Biomarkers at Clinical AKI Diagnosis. Clin. J. Am. Soc. Nephrol., 2011, 6, 27402749. Abdallah, E.; Waked, E.; Al-Helalm, B.; Asad, R.; Nabil, M.; Harba, T. Novel Troponin-Like Biomarkers of Acute Kidney Injury. Saudi. J. Kidney. Dis. Transpl., 2013, 24(6), 1111-1124. Han, W.K.; Waikar, S.S.; Johnson, A.; Betensky, R.A.; Dent, C.L.; Devarajan, P.; Bonventre, J.V. Urinary biomarkers in the early diagnosis of acute kidney injury. Kidney. Int., 2008, 73, 863-869. Krawczeski, C.D.; Woo, J.G,.; Wang, Y.; Bennett, M.R.; Ma, Q.; Devarajan, P. Neutrophil gelatinase-associated
14 Current Medicinal Chemistry, 2016, Vol. 23, No. 8
[41]
[42] [43]
[44]
[45]
[46]
[47] [48]
[49]
[50]
[51]
[52]
[53]
lipocalin concentrations predict development of acute kidney injury in neonates and children after cardiopulmonary bypass. J. Pediatr., 2011, 158, 1009-1015. Hazle, M.A.; Gajarski, R.J.; Aiyagari, R.; Yu, S.; Abraham, A.; Donohue, J.; Blatt. N.B. Urinary biomarkers and renal near-infrared spectroscopy predict intensive care unit outcomes after cardiac surgery in infants younger than 6 months of age. J. Thorac. Cardiovasc. Surg., 2013, 146(4), 861-867. Cruz, D.N.; de Geus, H.R.; Bagshaw, S.M. Biomarker strategies to predict need for renal replacement therapy in acute kidney injury. Semin. Dial., 2011, 24(2), 124-132. Nijboer, W.N.; Schuurs, T.A.; Damman, J.; van Goor, H.; Vaidya, V.S.; van der Heide, J.J.; Leuvenink, H.G.; Bonventre, J.V.; Ploeg, R.J. Kidney injury molecule-1 is an early noninvasive indicator for donor brain death-induced injury prior to kidney transplantation. Am. J. Transplant., 2009, 9, 1752-1759. Schröppel, B.; Krüger, B.; Walsh, L.; Yeung, M.; Harris, S.; Garrison, K.; Himmelfarb, J.; Lerner, S.M.; Bromberg, J.S.; Zhang, P.L.; Bonventre, J.V.; Wang, Z.; Farris, A.B.; Colvin, R.B.; Murphy, B.T.; Vella, J.P. Tubular expression of KIM-1 does not predict delayed function after transplantation. J. Am. Soc. Nephrol., 2010, 21(3), 536-42. Szeto, C.C.; Kwan, B.C.; Lai, K.B.; Lai, F.M.; Chow, K.M.; Wang, G.; Luk, C.C.; Li, P.K. Urinary expression of kidney injury markers in renal transplant recipients. Clin. J. Am. Soc. Nephrol., 2010, 5, 2329-37. Endre, Z.H.; Pickering, J.W.; Walker, R.J.; Devarajan, P.; Edelstein, C.L.; Bonventre, J.V.; Frampton, C.M.; Bennett, M.R.; Ma, Q.; Sabbisetti, V.S.; Vaidya, V.S.; Walcher, A.M.; Shaw, G.M.; Henderson, S.J.; Nejat, M.; Schollum, J.B.; George, P.M. Improved performance of urinary biomarkers of acute kidney injury in the critically ill by stratification for injury duration and baseline renal function. Kidney. Int., 2011, 79, 1119-30. Gonzalez, F.; Vincent, F. Biomarkers for acute kidney injury in critically ill patients. Minerva. Anestesiol., 2012, 78, 1394-1403. Noto, A.; Cibecchini, F.; Fanos, V.; Mussap, M. NGAL and Metabolomics: The Single Biomarker to Reveal the Metabolome Alterations in Kidney Injury. Biomed. Res. Int., 2013, 2013, 612032. Mishra, J.; Qing, M.A.; Prada, A.; Mitsnefes, M.; Zahedi, K.; Yang, J.; Barasch, J.; Devarajan, P. Identification of neutrophil gelatinase-associated lipocalin as a novel early urinary biomarker for ischemic renal injury. J. Am. Soc. Nephrol., 2003, 14(10), 2534-2543. Wheeler, D.S.; Devarajan, P.; Ma, Q.; Harmon, K.; Monaco, M.; Cvijanovich, N.; Wong, H.R. Serum neutrophil gelatinase-associated lipocalin (NGAL) as a marker of acute kidney injury in critically ill children with septic shock. Crit. Care. Med., 2008, 36, 1297-1303. Zappitelli, M.; Washburn, K.K.; Arikan, A.A.; Loftis, L.; Ma, Q.; Devarajan, P.; Parikh, C.R.; Goldstein, .SL. Urine neutrophil gelatinase-associated lipocalin is an early marker of acute kidney injury in critically ill children: a prospective cohort study. Crit. Care., 2007, 11, R84. Supavekin S.; Zhang, W.; Kucherlapati, R.; Kaskel, F.J,.; Moore, L.C.; Devarajan, P. Differential gene expression following early renal ischemia/reperfusion. Kidney. Int., 2003, 63(5), 1714-1724. Yuen, P.S.; Jo, S.K.; Holly, M.K.; Hu, X.; Star, R.A. Ischemic and nephrotoxic acute renal failure are distinguished by their broad transcriptomic responses. Physiol. Genomics, 2006, 25(3), 375-386.
Medić et al. [54] [55]
[56]
[57]
[58]
[59]
[60] [61]
[62]
[63] [64] [65]
[66]
[67]
Jennifer, R.C.; Didier, Portilla.; Mark, D.O. A basic science view of acute kidney injury biomarkers. Nephrol. Dial. Transplant., 2014, 29, 1301-1311. Paragas, N.; Qiu, A.; Zhang, Q.; Samstein, B.; Deng, S.X.; Schmidt-Ott, K.M.; Viltard, M.; Yu, W.; Forster, C.S.; Gong, G.; Liu, Y.; Kulkarni, R.; Mori, K.; Kalandadze, A.; Ratner, A.J.; Devarajan, P.; Landry, D.W.; D'Agati, V.; Lin, C.S.; Barasch, J. The Ngal reporter mouse detects the response of the kidney to injury in real time. Nat. Med., 2011, 17(2), 216-222. Kuwabara, T.; Mori, K.; Mukoyama, M.; Kasahara, M.; Yokoi, H.; Saito, Y.; Yoshioka, T.; Ogaw,a Y.; Imamaki, H,.; Kusakabe, T.; Ebihara, K.; Omata, M.; Satoh, N.; Sugawara, A.; Barasch, J.; Nakao, K. Urinary neutrophil gelatinase-associated lipocalin levels reflect damage to glomeruli, proximal tubules, and distal nephrons. Kidney. Int., 2009, 75(3), 285-294. Nickolas, T.L.; O’Rourke, M.J.; Yang, J.; Sise, M.E.; Canetta, P.A.; Barasch, N.; Buchen, C.; Khan, F,.; Mori, K.; Giglio, J.; Devarajan, P.; Barasch, J. Sensitivity and specificity of a single emergency department measurement of urinary neutrophil gelatinase-associated lipocalin for diagnosing acute kidney injury. Ann. Intern. Med., 2008, 148(11), 810-819. Mishra J, Dent C, Tarabishi R, Mitsnefes MM, Ma Q, Kelly C, Ruff SM, Zahedi K, Shao M, Bean J, Mori K, Barasch J, Devarajan P:Neutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renal injury after cardiac surgery. Lancet, 2005, 365, 1231-1238. Mori, K.; Lee, H.T.; Rapoport, D.; Drexler, I.R.; Foster, K.; Yang, J.; Schmidt-Ott. K.M,.; Chen, X.; Li, J.Y,.; Weiss, S.; Mishra, J.; Cheema, F.H.; Markowitz, G.; Suganami, T.; Sawai, K.; Mukoyama, M.; Kunis, C.; D'Agati, V.; Devarajan, P.; Barasch, J.; Endocytic delivery of lipocalinsiderophore-iron complex rescues the kidney from ischemia-reperfusion injury. J. Clin. Invest., 2005, 115, 610-21. Devarajan, P.Neutrophil gelatinase-associated lipocalin (NGAL): A new marker of kidney disease. Scand. J. Clin. Lab. Invest. Suppl., 2008, 241, 89-94. Hoffmann, D.; Fuchs, T.C.; Henzler, T.; Matheis, K.A.; Herget, T.; Dekant, W.; Hewitt, P.; Mally, A. Evaluation of a urinary kidney biomarker panel in rat models of acute and subchronic nephrotoxicity. Toxicology. 2010, 277, 49-58. Entin-Meer, M.; Ben-Shoshan, J.; Maysel-Auslender, S.; Levy, R.; Goryainov, P.; Schwartz, I.; Barshack, I.; Avivi, C.; Sharir, R.; Keren, G. Accelerated renal fibrosis in cardiorenal syndrome is associated with long-term increase in urine neutrophil gelatinase-associated lipocalin levels.. Am. J. Nephrol., 2012, 36(2), 190-200. Sushrut, S.: Waikar, J.V. Bonventre. Biomarkers for the Diagnosis of Acute Kidney Injury. Nephron. Clin. Pract., 2008, 109, c192-c197. Adiyanti, S.I.; Loho, T. Acute Kidney Injury (AKI) Biomarker. Med. Indones-Indones. J. Intern. Med., 2012, 44 (3), 246-255. Cruz, D.N.; Gaiao, S.; Maisel, A.; Ronco, C.; Devarajan, P. Neutrophil gelatinase-associated lipocalin as a biomarker of cardiovascular disease: a systematic review. Clin. Chem. Lab. Med., 2012, 50, 1533-1545. Cho, E.; Kim, S.C.; Kim, M.G.; Jo, S.K.; Cho, W.Y.; Kim, H.K. The incidence and risk factors of acute kidney injury after hepatobiliary surgery: a prospective observational study. BMC. Nephrol., 2014, 15, 169-176. Sanjeevani, S.; Pruthi, S.; Kalra, S.; Goel, A.; Kalra, O.P. Role of neutrophil gelatinase-associated lipocalin for early detection of acute kidney injury. Int. J. Crit. Illn. Inj. Sci., 2014, 4(3), 223-8.
Evaluation of Novel Biomarkers of Acute Kidney Injury [68] [69]
[70]
[71]
[72]
[73]
[74]
[75]
[76]
[77]
[78]
[79]
[80]
Bennett, M.R.; Nehus, E.; Haffner, C.; Ma, Q.; Devarajan P. Pediatric reference ranges for acute kidney injury biomarkers. Pediatr. Nephrol., 2015, 30(4), 677-85. Singer, E.; Markó, L.; Paragas, N.; Barasch, J.; Dragun, D.; Müller, D,.; Budde1, K.; Schmidt-Ott, K. Neutrophil gelatinase-associated lipocalin: pathophysiology and clinical applications. Acta. Physiol., 2013, 207(4), 663-672. Koyner, J.L.; Garg, A.X.; Coca, S.G.; Sint, K.; ThiessenPhilbrook, H.; Patel, U.D.; Shlipak, M.G.; Parikh, C.R. Biomarkers predict progression of acute kidney injury after cardiac surgery. J. Am. Soc. Nephrol., 2012, 23, 905-914. Han, W.K.; Wagener, G.; Zhu, Y.; Wang, S.; Lee, H.T. Urinary biomarkers in the early detection of acute kidney injury after cardiac surgery. Clin. J. Am. Soc. Nephrol., 2009, 4, 873-82. Damman, K.; van Veldhuisen, D.J.; Navis, G.; Voors, A.A.; Hillege, H.L. Urinary neutrophil gelatinase associated lipocalin (NGAL), a marker of tubular damage, is increased in patients with chronic heart failure. Eur. J. Heart. Fail., 2008, 10, 997-1000. Yndestad, A.; Landro, L.; Ueland, T.; Dahl, C.P.; Flo, T.H.; Vinge, L.E.; Espevik, T.; Frøland, S.S.; Husberg, C.; Christensen, G.; Dickstein, K.; Kjekshus, J.; Øie, E.; Gullestad, L.; Aukrust P.Increased systemic and myocardial expression of neutrophil gelatinase-associated lipocalin in clinical and experimental heart failure. Eur. Heart. J., 2009, 30, 1229-1236. Alvelos, M.; Lourenço, P.; Dias, C.; Amorim, M.; Rema, J.; Leite, A.B.; Guimarães, J.T.; Almeida, P.; Bettencourt, P. Prognostic value of neutrophil gelatinase-associated lipocalin in acute heart failure. Int. J. Cardiol., 2013, 165, 51-55. Bolignano, D.; Basile, G.; Parisi, P.; Coppolino, G.; Nicocia, G.; Buemi, M. Increased plasma neutrophil gelatinaseassociated lipocalin levels predict mortality in elderly patients with chronic heart failure. Rejuvenation. Res., 2009, 12(1), 7-14. Daniels, L.B.; Barrett-Connor, E.; Clopton, P.; Laughlin, G.A.; Ix, J.H.; Maisel, A.S. Plasma neutrophil gelatinaseassociated lipocalin is independently associated with cardiovascular disease and mortality in community-dwelling older adults: The Rancho Bernardo Study. J. Am. Coll. Cardiol., 2012, 59, 1101-1109. Ho, J.; Tangri, N.; Komenda, P.; Kaushal, A.; Sood, M.; Brar, R.; Gill, K.; Walker, S.; MacDonald, K.; Hiebert, B.M.; Arora, R.C.; Rigatto, C. Urinary, Plasma, and Serum Biomarkers' Utility for Predicting Acute Kidney Injury Associated With Cardiac Surgery in Adults: A Meta-analysis. Am. J. Kidney. Dis., 2015. doi: 10.1053/j.ajkd.2015.06.018 Nickolas, T.L.; Schmidt-Ott, K.M.; Canetta, P.; Forster, C.; Singer, E.; Sise, M.; Elger, A.; Maarouf, O.; Sola-Del Valle, D.A.; O'Rourke, M.; Sherman, E.; Lee, P.; Geara, A.; Imus, P.; Guddati, A.; Polland, A.; Rahman, W.; Elitok, S.; Malik, N.; Giglio, J.; El-Sayegh, S.; Devarajan, P.; Hebbar, S.; Saggi, S.J.; Hahn, B.; Kettritz, R.; Luft, F.C.; Barasch, J. Diagnostic and prognostic stratification in the emergency department using urinary biomarkers of nephron damage: a multicenter prospective cohort study.. J. Am. Coll. Cardiol., 2012, 59, 246-255. Singer, E.; Elger, A.; Elitok, S.; Kettritz, R.; Nickolas, T.L.; Barasch, J.; Luft, F.C.; Schmidt-Ott, K.M. Urinary neutrophil gelatinase-associated lipocalin distinguishes pre-renal from intrinsic renal failure and predicts outcomes. Kidney. Int., 2011, 80, 405-414. Hall, I.E.; Coca, S.G.; Perazella, M.A.; Eko, U.U.; Luciano, R.L.; Peter, P.R.; Han, W.K.; Parikh, C.R. Risk of poor outcomes with novel and traditional biomarkers at clinical AKI diagnosis. Clin. J. Am. Soc. Nephrol., 2011, 6, 2740-2749.
Current Medicinal Chemistry, 2016, Vol. 23, No. 8 [81]
[82]
[83]
[84]
[85]
[86]
[87]
[88]
[89]
[90] [91] [92] [93] [94]
[95]
15
Chen, T.H.; Chang, C.H.; Lin, C.Y.; Jenq, C.C.; Chang, M.Y.; Tian, Y.C.; Hung, C.C.; Fang, J.T.; Yang, C.W.; Wen, M.S.; Lin, F.C.; Chen, Y.C. Acute kidney injury biomarkers for patients in a coronary care unit: a prospective cohort study. PLoS. One. 2012, 7, e32328. Cantaluppi, V. Plasma NGAL is an early biomarker of delayed graft function and CNI nephrotoxicity in kidney transplantation from extended criteria donors. In: Presentation in A. Lewington (Chair), NGAL: Ready for Routine Clinical Use? An International Perspective. Symposium at 31st International Vicenza Course on Critical Care Nephrology, Vicenza, 2013. Ramírez-Sandoval, J.C.; Barrera-Chimal, J.; Simancas, P.E.; Rojas-Montaño, A.; Correa-Rotter, R.; Bobadilla, N.A.; Morales-Buenrostro, L.E. Urinary neutrophil gelatinase-associated lipocalin predicts graft loss after acute kidney injury in kidney transplant. Biomarkers., 2014, 19(1), 63-9. Muller, L.; Nicolas-Robin, A,.; Bastide, S.; Martinez, O.; Louart, G,.; Colavolpe, J.C.; Vachiery, F.; Alonso, S.; Lefrant, J.Y.; Riou, B. Assessment of neutrophil gelatinaseassociated lipocalin in the brain-dead organ donor to predict immediate graft function in kidney recipients: a prospective, multicenter study. Anesthesiology., 2015, 122(1), 96-105. Nisula, S.; Yang, R.; Kaukonen, K.M.; Vaara, S.T.; Kuitunen, A.; Tenhunen, J.; Pettilä, V.; Korhonen, A.M. The urine protein NGAL predicts renal replacement therapy, but not acute kidney injury or 90-day mortality in critically ill adult patients. Anesth. Analg., 2014, 119(1), 95-102. De Geus, H.RH.; Bakker, J.; Lesaffre, E.M.E.H.; Le Noble, J.L.M.L. Neutrophil gelatinase-associated lipocalin at ICU admission predicts for acute kidney injury in adult patients. Am. J. Respir. Crit. Care. Med., 2011, 183, 907-914. Cruz, D.N.; De Cal, M.; Garzotto, F.; Perazella, M.A.; Lentini, P.; Corradi, V.; Piccinni, P.; Ronco, C. Plasma neutrophil gelatinase-associated lipocalin is an early biomarker for acute kidney injury in an adult ICU population. Intensive. Care. Med., 2010, 36, 444-451. Yilmaz, A.; Sevketoglu, E.; Gedikbasi, A.; Karyagar, S.; Kiyak, A.; Mulazimoglu, M.; Aydogan, G.; Ozpacaci, T.; Hatipoglu, S. Early prediction of urinary tract infection with urinary neutrophil gelatinase associated lipocalin. Pediatr. Nephrol., 2009, 24, 2387-2392. Di Somma, S.; Magrin,i L.; De Berardinis, B.; Marino, R.; Ferri, E.; Moscatelli, P.; Ballarino, P.; Carpinteri, G.; Noto, P.; Gliozzo, B.; Paladino, L.; Di Stasio, E. Additive value of blood neutrophil gelatinase-associated lipocalin to clinical judgement in acute kidney injury diagnosis and mortality prediction in patients hospitalized from the emergency department. Crit. Care., 2013, 17, R29. Gracie, J.A.; Robertson, S.E.; McInnes, I.B. Interleukin-18. J. Leukoc. Biol., 2003, 73, 213-224. Dinarello, C.A. Interleukin-18 and the pathogenesis of inflammatory diseases. Semin. Nephron., 2007, 27(1), 98-114. Lochner, M.; Forster, I. Anti-interleukin-18 therapy in murine models of inflammatory bowel disease. Pathobiology., 2002, 70, 164-169. Gonzalez, F.; Vincent, F. Biomarkers for acute kidney injury in critically ill patients. Minerva. Anestesiol., 2012, 78, 1394-1403. Edelstein, C.L.; Hoke, T.S.; Somerset, H.; Fang, W.; Klein, C.L.; Dinarello, C.A.; Faubel S. Proximal tubules from caspase-1-deficient mice are protected against hypoxiainduced membrane injury. Nephrol. Dial. Transplant., 2007, 22(4), 1052-1061. Melnikov, V.Y.; Faubel, S.; Siegmund, B.; Lucia, M.S.; Ljubanovic, D.; Edelstein, C.L. Neutrophil-independent mechanisms of caspase-1- and IL-18-mediated ischemic
16 Current Medicinal Chemistry, 2016, Vol. 23, No. 8
[96]
[97]
[98]
[99]
[100]
[101]
[102]
[103] [104]
[105]
[106]
[107]
[108]
[109]
[110]
acute tubular necrosis in mice. J. Clin. Invest., 2002, 110(8), 1083-1091. Award, A.S.; El-sharif, AA. Curcumin immune-mediated and anti-apoptotic mechanisms protect against renal ischemia/reperfusion and distant organ induced injuries. Int. Immunopharmacol., 2011, 11(8), 992-996. Luo, Q.; Zhou, F.; Dong, H.; Wu, L.; Chai, L.; Lan, K.; Wu, M. Implication of combined urinary biomarkers in early diagnosis of acute kidney injury following percutaneous coronary intervention. Clin. Nephrol., 2013, 79(2), 85-92. Zheng, J.; Xiao, Y.; Yao, Y.; Xu, G.; Li, C.; Zhang, Q.; Li, H.; Han, L. Comparison of urinary biomarkers for early detection of acute kidney injury after cardiopulmonary bypass surgery in infants and young children. Pediatr. Cardiol., 2013, 34(4), 880-886. Sirota, J.C.; Walcher, A.; Faubel, S.; Jani, A.; McFann, K.; Devarajan, P.; Davis, C.L.; Edelstein, C.L. Urine IL-18, NGAL, IL-8 and serum IL-8 are biomarkers of acute kidney injury following liver transplantation. BMC. Nephrol., 2013, 14, 17. Parikh, C.R.; Abraham, E.; Ancukiewicz, M.; Edelstein, C.L.Urine IL-18 is an early diagnostic marker for acute kidney injury and predicts mortality in the intensive care unit. J. Am. Soc. Nephrol., 2005, 16, 3046-3052. Liu, Y.W.; Su, C.T.; Chang, Y.T.; Tsai, W.C.; Su, Y.R.; Wang, S.P.; Yang, C.S.; Tsai, L.M.; Chen, J.H.; Sung, J.M. Elevated serum interleukin-18 level is associated with allcause mortality in stable hemodialysis patients independently of cardiac dysfunction. PLoS. One., 2014, 9(3), e89457. Nisula, S.; Yang, R.; Poukkanen, M.; Vaara, S.T.; Kaukonen, K.M.; Tallgren, M.; Haapio, M.; Tenhunen, J.; Korhonen, A.M.; Pettilä, V. Predictive value of urine interleukin-18 in the evolution and outcome of acute kidney injury in critically ill adult patients. Br. J. Anaesth., 2015, 114(3), 460-8. Lin, X.; Yuan, J.; Zhao, Y.; Zha, Y. Urine interleukin-18 in prediction of acute kidney injury: a systemic review and meta-analysis. J. Nephrol., 2015, 28, 7-16. Parikh, C.R.; Mishra, J.; Thiessen-Philbrook, H.; Dursun, B.; Ma, Q.; Kelly, C.; Dent, C.; Devarajan, P.; Edelstein, C.L. Urinary IL-18 is an early predictive biomarker of acute kidney injury after cardiac surgery. Kidney. Int., 2006, 70, 199- 203. Haase, M.; Bellomo, R.; Story, D.; Davenport, P.; HaaseFielitz, A. Urinary interleukin-18 does not predict acute kidney injury after adult cardiac surgery: a prospective observational cohort study. Crit. Care., 2008; 12: R96. Xin, C.; Yulong, X.; Yu, C.; Changchun, C.; Feng, Z.; Xinwei, M. Urine neutrophil gelatinase-associated lipocalin and interleukin-18 predict acute kidney injury after cardiac surgery. Renal. Fail., 2008; 30: 904-13. Coca, S.G.; Yalavarthy, R.; Concato, J.; Parikh, C.R. Biomarkers for the diagnosis and risk stratification of acute kidney injury: a systematic review. Kidney. Int., 2008, 73(9), 1008-1016. Siew, E.D.; Ikizler, T.A.; Gebretsadik, T.; Shintani, A.; Wickersham, N.; Bossert, F.; Peterson, J.F.; Parikh, C.R.; May, A.K.; Ware, L.B. Elevated urinary IL-18 levels at the time of ICU admission predict adverse clinical outcomes. Clin. J. Am. Soc. Nephrol., 2010, 5(8), 1497-1505. Li, Y.; Fu, C.; Z hou, X.; Xiao, Z.; Z hu, X.; Jin, M.; Li, X.; Feng, X. Urine interleukin- 18 and cystatin-C as biomarkers of acute kidney injury in critically ill neonates. Pediatr. Nephrol., 2012, 27(5), 851-60. Parikh, C.R.; Jani, A.; Mishra, J.; Ma, Q.; Kelly, C.; Barasch, J.; Edelstein, C.L.; Devarajan, P. Urine NGAL and IL-18 are predictive biomarkers for delayed graft function
Medić et al.
[111]
[112]
[113]
[114]
[115] [116] [117]
[118]
[119]
[120]
[121]
[122]
[123]
[124]
[125]
following kidney transplantation. Am. J. Transplant., 2006, 6, 1639-1645. Parikh, C.R.; Jani, A.; Melnikov, V.Y.; Faubel, S.; Edelstein, C.L. Urinary interleukin-18 is a marker of human acute tubular necrosis. Am. J. Kidney. Dis., 2004, 43(3), 405-414. Striz, I.; Eliska, K.; Honsova, E.; Lacha, J.; Petrickova, K.; Jaresova, M.; Lodererova, A.; Bohmova, R.; Valhova, S.; Slavcev, A.; Vitko, S. Interleukin 18 (IL-18) upregulation in acute rejection of kidney allograft. Immunol. Lett., 2005, 99(1), 30-35. Pianta, T.J.; Peake, P.W.; Pickering, J.W.; Kelleher, M.; Buckley, N.A.; Endre, Z.H. Clusterin in kidney transplantation: novel biomarkers versus serum creatinine for early prediction of delayed graft function Transplantation., 2015, 99(1), 171-9. Dharnidharka, V.R.; Kwon, C.; Stevens, G. Serum cystatin C is superior to serum creatinine as a marker of kidney function: a meta-analysis. Am. J. Kidney. Dis., 2002, 40(2), 221-226. Westhuyzen, J. Cystatin C: A promising marker and predictor of impaired renal function. Ann. Clin. Lab. Sci., 2006, 36, 387-394. Lassus, J.; Harjola, V.P. Cystatin C: a step forward in assessing kidney function and cardiovascular risk. Heart. Fail. Rev., 2012, 17(2), 251-261. Knight, E.L.; Verhave, J.C.; Spiegelman, D.; Hillege, H.L.; de Zeeuw, D.; Curhan, G.C.; de Jong, P.E. Factors influencing serum cystatin C levels other than renal function and the impact on renal function measurement. Kidney. Int., 2004, 65, 1416-1421. Shlipak, M.G.; Sarnak, M.J.; Katz R, Fried, L.F.; Seliger, S.L.; Newman, A.B.; Siscovick, D.S.; Stehman-Breen, C. Cystatin C and the risk of death and cardiovascular events among elderly persons. N. Engl. J. Med., 2005, 352, 20492060. Conti, M.; Moutereau, S.; Zater, M.; Lallali, K.; Durrbach, A.; Manivet, P.; Eschwege, P.; Loric, S. Urinary cystatin C as a specific marker of tubular dysfunction. Clin. Chem. Lab. Med., 2006, 44, 288-291. Jernberg, T.; Lindahl, B.; James, S.; Larsson, A.; Hansson, L.O.; Wallentin, L. Cystatin C: A novel predictor of outcome in suspected or confirmed non-ST-elevation acute coronary syndrome. Circulation., 2004, 110, 2342-2348. Al-Beladi, F.I. Cystatin C is an early marker of contrastinduced nephropathy in patients with sepsis in the intensive care unit. Saudi. J. Kidney. Dis. Transpl., 2015, 26(4), 71824. Chen, S.; Shi, J.S.; Yibulayin, X.; Wu, T.S.; Yang, X.W.; Zhang, J.; Baiheti, P. Cystatin C is a moderate predictor of acute kidney injury in the early stage of traumatic hemorrhagic shock. Exp. Ther. Med., 2015, 10(1), 237-240. Dai, X.; Zeng, Z.; Fu, C.; Zhang, S.; Cai, Y.; Chen, Z. Diagnostic value of neutrophil gelatinase-associated lipocalin, cystatin C, and soluble triggering receptor expressed on myeloid cells-1 in critically ill patients with sepsisassociated acute kidney injury. Crit. Care., 2015, 19, 223. Zappitelli, M.; Greenberg, J.H.; Coca, S.G.; Krawczeski, C.D.; Li, S.; Thiessen-Philbrook, H.R.; Bennett, M.R.; Devarajan, P.; Parikh, C.R. Association of definition of acute kidney injury by cystatin C rise with biomarkers and clinical outcomes in children undergoing cardiac surgery. JAMA. Pediatr., 2015, 169(6), 583-91. Lagos-Arevalo, P.; Palijan, A.; Vertullo, L.; Devarajan, P.; Bennett, M.R.; Sabbisetti, V.; Bonventre, J.V.; Ma, Q.; Gottesman, R.D.; Zappitelli, M. Cystatin C in acute kidney injury diagnosis: early biomarker or alternative to serum creatinine? Pediatr. Nephrol., 2015, 30(4), 665-76.
Evaluation of Novel Biomarkers of Acute Kidney Injury [126] Bongiovanni, C.; Magrini, L.; Salerno, G.; Gori, C.S.; Cardelli, P.; Hur, M.; Buggi, M.; Di Somma, S. Serum cystatin c for the diagnosis of acute kidney injury in patients admitted in the emergency department. Dis. Markers., 2015, 2015, 416059. [127] Zimmerman, A.W., and Veerkamp, J.H. New insights into the structure and function of fatty acid-binding proteins. Cell. Mol. Life. Sci., 2002, 59, 1096-1116. [128] Massolini, G., and Calleri, E. Survey of binding properties of fatty acid-binding proteins chromatographic methods. J. Chromatogr., 2003, B797, 255-268. [129] Yokoyama, T.; Kamijo-Ikemori, A.; Sugaya, T.; Hoshino, S.; Yasuda, T.; Kimura, K. Urinary excretion of liver type fatty acid binding protein accurately reflects the degree of tubulointerstitial damage. Am. J. Pathol., 2009, 174(6), 2096-2106. [130] Noiri, E.; Doi, K.; Negishi, K.; Tanaka, T.; Hamasaki, Y.; Fujita, T.; Portilla, D. Sugaya TUrinary fatty acid-binding protein 1: an early predictive biomarker of kidney injury. Am. J. Physiol. Renal. Physiol., 2009, 296(4), F669-F679. [131] Portilla, D.; Dent, C.; Sugaya, T.; Nagothu, K.K.; Kundi, I.; Moore, P.; Noiri, E.; Devarajan, P. Liver fatty acid-binding protein as a biomarker of acute kidney injury after cardiac surgery. Kidney. Int., 2008, 73(4), 465-472. [132] Kamijo-Ikemori, A.; Hashimoto, N.; Sugaya, T.; Matsui, K.; Hisamichi, M.; Shibagaki, Y.; Miyake, F.; Kimura, K. Elevation of urinary liver-type fatty acid binding protein after cardiac catheterization related to cardiovascular events. Int. J. Nephrol. Renovasc. Dis., 2015; 8: 91-99. [133] Ferguson, M.A.; Vaidya, V.S.; Waikar, S.S.; Collings, F.B.; Sunderland, K.E.; Gioules, C.J.: Bonventre, J.V. Urinary liver-type fatty acid-binding protein predicts adverse outcomes in acute kidney injury. Kidney. Int., 2010, 77, 708714. [134] Nakamura, T.; Sugaya, T.; Koide, H. Urinary liver-type fatty acid-binding protein in septic shock: effect of polymyxin B-immobilized fiber hemoperfusion. Shock, 2009, 31(5), 454-459. [135] Li, Y.; Zhu, M.; Xia, Q.; Wang, S.; Qian, J.; Lu, R.; Che, M.; Dai, H.; Wu, Q.; Ni, Z.; Lindholm, B.; Axelsson, J.; Yan, Y. Urinary neutrophil gelatinase-associated lipocalin and L-type fatty acid binding protein as diagnostic markers of early acute kidney injury after liver transplantation. Biomarkers, 2012, 17(4), 336-342. [136] Susantitaphong, P.; Siribamrungwong, M.; Doi, K.; Noiri, E.; Terrin, N.; Jabe, B. Performance of urinary liver-type
Received: November 19, 2015
Revised: February 09, 2016
Accepted: February 09, 2016
Current Medicinal Chemistry, 2016, Vol. 23, No. 8
[137] [138]
[139]
[140]
[141] [142] [143]
[144]
[145]
[146]
17
fatty acid-binding protein in acute kidney injury: a metaanalysis. Am. J. Kidney. Dis., 2013, 61(3), 430-439. Cho, E.; Yang, H.N.; Jo, S.K.; Cho, W.Y.; Kim, H.K. The role of urinary liver-type fatty acid-binding protein in critically ill patients. J. Korean. Med. Sci., 2013, 28(1), 100-5. Parr, S.K.; Clark, A.J.; Bian, A.; Shintani, A.K.; Wickersham, N.E.; Ware, L.B.; Ikizler, T.A.; Siew, E.D. Urinary L-FABP predicts poor outcomes in critically ill patients with early acute kidney injury. Kidney. Int., 2015, 87(3), 640-8. Zeng, X.F.; Li, J.M.; Tan, Y.; Wang, Z.F.; He, Y.; Chang, J.; Zhang, H.; Zhao, H.; Bai, X.; Xie, F.; Sun, J.; Zhang, Y. Performance of urinary NGAL and L-FABP in predicting acute kidney injury and subsequent renal recovery: a cohort study based on major surgeries. Clin. Chem. Lab. Med., 2014, 52(5), 671-8. Okazaki, Y.; Furuhashi, M.; Tanaka, M.; Mita, T.; Fuseya, T.; Ishimura S.; Watanabe, Y.; Hoshina, K.; Akasaka, H.; Ohnishi, H.; Yoshida, H.; Saitoh, S.; Shimamoto, K.; Miura, T. Urinary excretion of fatty acid-binding protein 4 is associated with albuminuria and renal dysfunction. PLoS. One., 2014, 9(12), e115429. Hawkins R. New Biomarkers of Acute Kidney Injury and the Cardio-renal Syndrome. Korean. J. Lab. Med., 2011, 31, 72-80. Devarajan P. The future of pediatric AKI management biomarkers. Semin. Nephrol., 2008, 28(5), 493-498. Haase-Fielitz, A.; Haase, M.; Devarajan, P. Neutrophil gelatinase-associated lipocalin as a biomarker of acute kidney injury: a critical evaluation of current status. Ann. Clin. Biochem., 2014, 51(3), 335-351. Hillege, H.L.; Nitsch, D.; Pfeffer, M.A.; Swedberg, K.; McMurray, J.J.; Yusuf, S.; Granger, C.B.; Michelson, E.L.; Ostergren, J.; Cornel, J.H.; de Zeeuw, D.; Pocock, S.; van Veldhuisen, D.J. Renal function as a predictor of outcome in a broad spectrum of patients with heart failure. Circulation, 2006, 113, 671-8. Smith, G.L.; Lichtman, J.H.; Bracken, M.B.; Shlipak, M.G.; Phillips, C.O.; DiCapua, P.; Krumholz, H.M. Renal impairment and outcomes in heart failure: systematic review and meta-analysis. J. Am. Coll. Cardiol., 2006, 47, 1987-96. Devarajan P. Biomarkers for the early detection of acute kidney injury. Curr. Opin. Pediatr., 2011, 23(2), 194-200.