Increased Risk of Pneumonia and Bronchiolitis after Bacterial Colonization of the Airways as Neonates Nadja H. Vissing1, Bo L. K. Chawes1, and Hans Bisgaard1 1 Copenhagen Prospective Studies on Asthma in Childhood, Health Sciences, University of Copenhagen and Copenhagen University Hospital, Gentofte, Copenhagen, Denmark
Rationale: The frequency of pneumonia and bronchiolitis exhibits considerable variation in otherwise healthy children, and suspected risk factors explain only a minor proportion of the variation. We hypothesized that alterations in the airway microbiome in early life may be associated with susceptibility to pneumonia and bronchiolitis in young children. Objectives: To investigate the relation between neonatal airway colonization and pneumonia and bronchiolitis during the first 3 years of life. Methods: Participants comprised children of the Copenhagen Prospective Studies on Asthma in Childhood2000 (COPSAC2000) cohort, a prospective birth cohort study of 411 children born to mothers with asthma. Aspirates from the hypopharynx at age 4 weeks were cultured for Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, and Staphylococcus aureus. Clinical information on pneumonia and bronchiolitis within the first 3 years of life was prospectively collected by the research physicians at the center. Analyses were adjusted for covariates associated with pneumonia and bronchiolitis and bacterial airway colonization. Measurements and Main Results: Hypopharyngeal aspirates and full clinical follow-up until 3 years of age were available for 265 children. Of these, 56 (21%) neonates were colonized with S. pneumoniae, H. influenzae, and/or M. catarrhalis at 4 weeks of age. Colonization with at least one of these microorganisms (but not S. aureus) was significantly associated with increased incidence of pneumonia and bronchiolitis (adjusted incidence rate ratio, 1.79 [1.29–2.48]; P , 0.005) independently of concurrent or later asthma. Conclusions: Neonatal airway colonization with S. pneumoniae, H. influenzae, or M. catarrhalis is associated with increased risk of pneumonia and bronchiolitis in early life independently of asthma. This suggests a role of pathogenic bacterial colonization of the airways in neonates for subsequent susceptibly to pneumonia and bronchiolitis. Keywords: bacterial colonization; airways; neonatal; pneumonia; bronchiolitis
(Received in original form February 4, 2013; accepted in final form September 4, 2013) Supported by the Lundbeck Foundation, the Danish Strategic Research Council, the Pharmacy Foundation of 1991, the Augustinus Foundation, the Danish Medical Research Council, and the Danish Pediatric Asthma Centre. The funding sources had no involvement in study design; collection, analysis, or interpretation of data; the writing of this report; or the decision to submit the paper for publication. Author Contributions: The guarantor of the study is H.B., who has been responsible for the integrity of the work as a whole, from conception and design to acquisition of data, analysis and interpretation of data, and writing of the manuscript. N.H.V. was responsible for acquisition of data, data analyses, and interpretation and writing of the manuscript. B.L.K.C. contributed to data interpretation and writing of the manuscript. All authors made important intellectual contributions and critical final revision of the manuscript. Correspondence and requests for reprints should be addressed to Hans Bisgaard, M.D., D.M.Sci., Copenhagen Prospective Studies on Asthma in Childhood, Copenhagen University Hospital, Gentofte, Ledreborg Alle´ 34, DK-2820 Gentofte, Copenhagen, Denmark. E-mail:
[email protected] This article has an online supplement, which is accessible from this issue’s table of contents at www.atsjournals.org Am J Respir Crit Care Med Vol 188, Iss. 10, pp 1246–1252, Nov 15, 2013 Copyright ª 2013 by the American Thoracic Society Originally Published in Press as DOI: 10.1164/rccm.201302-0215OC on October 3, 2013 Internet address: www.atsjournals.org
AT A GLANCE COMMENTARY Scientific Knowledge on the Subject
A growing body of evidence suggests that early microbial colonization may influence infant immunity, and thus impose important consequences for disease susceptibility. Our previous studies showed that early airway colonization with pathogenic bacteria increases risk of recurrent wheeze and asthma during preschool age. What This Study Adds to the Field
This report identifies an association between bacterial colonization of the airways in neonates and increased risk of pneumonia and bronchiolitis in early childhood independently of concurrent asthma.
Frequency of pneumonia and bronchiolitis in young children exhibits a considerable variation in otherwise healthy individuals. Daycare attendance (1, 2), duration of breastfeeding (3, 4), crowding (5), siblings (6, 7), environmental tobacco smoke exposure (8), low socioeconomic status (9), and male sex (10) have all been associated with the risk of pneumonia and bronchiolitis in young children, but they only explain a minor proportion of the variation. Microbial exposure during early life seems to play an important role for innate immune functioning and maturation of the adaptive immune system (11, 12). We previously demonstrated that neonates colonized in the hypopharynx with Streptococcus pneumoniae, Haemophilus influenzae, or Moraxella catarrhalis have an increased risk of childhood asthma and recurrent wheeze in at-risk children (13) and in unselected children (14). Recently we showed that colonized neonates react with increased levels of cytokines and chemokines in the airway mucosal lining fluid (15). Therefore, we hypothesized that bacterial colonization of the neonatal airway could also affect susceptibility to pneumonia and bronchiolitis during early childhood. In this study, we investigated a possible relation between bacterial airway colonization of neonates and risk of pneumonia and bronchiolitis during the first 3 years of life in the Copenhagen Prospective Studies on Asthma in Childhood2000 (COPSAC) longitudinal birth cohort study. Some of the results of this study have been previously reported in the form of an abstract (16).
METHODS Study Cohort COPSAC2000 is a longitudinal clinical birth cohort study of 411 children recruited in Denmark during 1998–2001 among pregnant mothers with a history of asthma. A key feature of the study is the intense clinical surveillance of the cohort by the COPSAC doctors with scheduled 6-monthly clinical investigations and clinic visits for any acute airway symptom. The cohort has previously been thoroughly described
Vissing, Chawes, and Bisgaard: Neonatal Airway Colonization and Pneumonia and Bronchiolitis
1247
(13, 17–22). Data were collected according to Good Clinical Practice guidelines. The study was conducted in accordance with the Declaration of Helsinki and approved by the Copenhagen Ethics Committee (KF01-289/96) and the Danish Data Protection Agency (2008-41-1754). Written informed consent was obtained from both parents.
on daycare attendance, socioeconomic status described by yearly household income, mother’s education and occupation, and father’s history of asthma. Postnatal tobacco exposure was assessed by measuring nicotine concentration in hair samples at 1 and 3 years of age (27). See the online supplement for details.
Airway Bacterial Colonization
Statistics
Airway bacterial colonization was investigated in the infants at 4 weeks of age before any respiratory symptoms. When the infant was sedated during lung function testing (23), the doctor at the COPSAC clinical research unit performed a hypopharyngeal aspiration with a soft suction catheter passed through the nose. The sample was transported to the microbiology laboratory within 2 hours and cultured for bacteria with the use of standard culture techniques for identification of S. pneumoniae, H. influenzae, M. catarrhalis, and Staphylococcus aureus. Infants colonized with these bacteria were not prescribed antibiotic treatment because they were asymptomatic.
Neonatal colonization with S. pneumoniae, H. influenzae, and M. catarrhalis was investigated as coculture and as monoculture using children without any colonization of the three lung bacteria as control subjects. We performed survival statistics analyzing time to first episode of pneumonia or bronchiolitis with Cox regression estimating crude hazard ratios and obtained survival curves with Kaplan-Meier estimator. The association between bacterial colonization, covariates, and cumulative incidence of pneumonia and bronchiolitis was assessed by quasi-Poisson regression estimating incidence rate ratios (IRR). Crude IRR for each covariate was computed using univariate analyses. Significant covariates were included as possible confounders in a multivariate analysis estimating adjusted IRR (aIRR). We performed three stratified analyses of pneumonia and bronchiolitis to investigate potential confounding by underlying asthmatic disease. The first stratification was based on whether the child had or had not been diagnosed with asthma within the study period, the second was whether the child had asthma at 7 years of age, and third we stratified based on whether the child had experienced recurrent wheezy symptoms (defined as five episodes of TROLS within 6 months) at any point before 7 years of age. The frequency of bacterial or viral pathogen detection during pneumonia or bronchiolitis in children who were colonized versus noncolonized as neonates was assessed by chi-square tests. Analyses were performed in SAS version 9.3. (SAS Institute Inc., Cary, NC). Additional details are given in the online supplement.
Pneumonia and Bronchiolitis Diagnoses The children routinely visited the research clinic every 6 months and for acute visits for respiratory symptoms. In addition, the parents kept a calendar-based diary on the presence or absence of troublesome lung symptoms (TROLS), explained to the parents as wheeze or whistling sounds, breathlessness, or recurrent troublesome cough severely affecting the well-being of the infant (18, 24). The parents were encouraged to bring their child to the research clinic instead of the family doctor for any respiratory symptom. The children were examined, diagnosed, and treated for pneumonia and bronchiolitis by the COPSAC pediatricians in accordance with predefined standard procedures. Clinical pneumonia was defined by troublesome cough accompanied by tachypnea, fever, and abnormal auscultation (20), whereas bronchiolitis was defined by symptoms of coryza progressing over a few days to cough, tachypnea, chest retractions, and auscultative widespread crepitation and/or rhonchi in a child younger than 2 years of age (25). Hypopharyngeal aspirates were obtained during each acute visit for routine bacterial cultures and nasopharyngeal aspirates were performed for virus identification by polymerase chain reaction (20). A diagnosis of pneumonia or bronchiolitis was based on clinical appearance before and independent of identified pathogens. At each 6-monthly scheduled visit the research physicians interviewed the parents about their child’s illnesses and use of medication during the previous 6 months. The diaries were reviewed by the doctor as a part of the interview. Parents were asked (1) if their child had been ill since their last visit, (2) duration of any illness, (3) whether the child had been seen by a doctor outside the COPSAC clinic, (4) if the child was given medication (prescribed and over-the-counter medications), and (5) if the child was hospitalized or had any additional investigations performed during the illness. If the child had been seen elsewhere suspected for pneumonia or bronchiolitis (i.e., at the general practitioner or in a pediatric emergency department) details on clinical findings, diagnosis, and treatment were obtained from the source. We previously validated these external data on infectious episodes, which showed our records to be of high sensitivity for pneumonia and bronchiolitis (26). Children who missed two or more successive interview sessions were excluded from the analysis.
RESULTS Baseline
Hypopharyngeal samples were collected from 321 (78%) of the 411 newborns included in the COPSAC2000 birth cohort at age 4 weeks (87 infants had been enrolled before hypopharyngeal sampling was included in the study protocol and three samples were lost for technical reasons). Of the 321 children with valid samples, 56 children (17%) were excluded for missing two or more of the 6-monthly visits, leaving 265 children for this nested analysis. Table E1 in the online supplement shows baseline characteristics of the study group and excluded children. Children in the study group were born in families with higher household incomes than children excluded from analysis (mean income was 21% higher in the study group; P , 0.001) and attended daycare with significantly more crowding (mean number of children in the daycare center was 35% higher in the study group; P ¼ 0.001). Among the included children, 42 (16%) had been diagnosed with asthma before age 3. Information on asthma status at age 7 was available for 237 children. At that time, 33 (14%) had an asthma diagnosis and 63 (27%) had experienced recurrent wheezy symptoms.
Asthma Diagnosis Asthma was diagnosed as previously described in detail (18, 24) according to quantitative symptom burden focusing on persistent TROLS and response to antiasthmatic medication (see the online supplement for details).
Covariates Based on the literature (3–10) 20 covariates were chosen a priori for suspected relevance to either airway colonization or incidence of pneumonia and bronchiolitis: sex, birth weight, mode of delivery, siblings, duration of breastfeeding, maternal smoking and use of antibiotics during third trimester of pregnancy, cats or dogs in the home, details
Airway Bacterial Colonization
At 4 weeks of age, 24 (9%) of the 265 neonates were colonized with S. pneumoniae, 25 (9%) with H. influenzae, 22 (8%) with M. catarrhalis, and 56 (21%) were colonized with one or more of these species. Neonates with older siblings at home were more likely to be colonized (relative risk, 2.6 [2.01–3.40]; P , 0.005). Apart from this, colonized and noncolonized children did not differ with respect to baseline characteristics. S. aureus colonization was present in 164 (62%) and there were no differences in baseline characteristics between colonized and noncolonized children.
1248
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Pneumonia and Bronchiolitis
Pneumonia was diagnosed on 285 occasions and bronchiolitis on 40 occasions, yielding a total of 325 episodes of pneumonia and bronchiolitis. A total of 154 children (58%) experienced at least one episode of pneumonia or bronchiolitis, and mean incidence was 1.2 episodes per child (SD, 1.6) throughout the 3 years. In most cases (64%) the child was diagnosed by the COPSAC physicians at the COPSAC clinic during the infectious episode. Incidence of pneumonia and bronchiolitis was significantly associated with male sex, delivery by cesarean section, older siblings, mother’s use of antibiotics in third trimester, maternal smoking during third trimester, nicotine level in the child’s hair at age 3 years, and mother’s unemployment. Birth weight, prolonged breastfeeding, and age at introduction to daycare were inversely associated with incidence of pneumonia and bronchiolitis (Table 1). After including these covariates in the multivariate analysis, the remaining significant covariates were cesarean section (aIRR, 1.43 [1.04–1.96]; P ¼ 0.03), male sex (aIRR, 1.43 [1.08–1.90]; P ¼ 0.01), maternal smoking during third trimester (aIRR, 1.80, [1.27–2.56]; P , 0.005), age at introduction to daycare (aIRR per interquartile range [days], 0.80 [95% confidence interval, 0.67– 1.95]; P ¼ 0.01), and mother’s employment (aIRR compared with professional: student, 1.75 [1.11–2.76], P ¼ 0.02; unemployed, 1.78 [ 1.13–2.81], P ¼ 0.01). Pneumonia and bronchiolitis occurred more frequently among children with asthma: in 90% of children with asthma before age 3 versus 43% of children without asthma before age 3 (P , 0.005) (Table E2), and in 81% of children with asthma at age 7 versus 45% of children without asthma at age 7 (P , 0.005) (Table E3). Bacterial Colonization versus Pneumonia and Bronchiolitis
Neonates colonized in the airways with S. pneumoniae, H. influenzae, M. catarrhalis, or a combination of these species had increased risk of experiencing pneumonia or bronchiolitis within the first
VOL 188
2013
3 years (hazard ratio, 1.79 [1.3–2.6]; P ¼ 0.002). Figure 1 presents the Kaplan-Meier plot for time to first pneumonia or bronchiolitis stratified by bacterial colonization. aIRR was 1.79 (1.29–2.48), P , 0.005, for neonates colonized with any of the three lung pathogenic bacteria and the direction of association was similar for all three bacteria (Table 2). Colonization with S. aureus was not associated with incidence of pneumonia and bronchiolitis, neither separately nor in combination with other species. Stratified analyses based on asthma diagnosis at the ages 3 and 7 years and recurrent asthmatic symptoms were performed to investigate possible effect modification of asthma status (Figure 2). The association between pneumonia and bronchiolitis and colonization with at least one of the three airway pathogens compared with no colonization was strengthened after excluding the children diagnosed with asthma by age 3 (n ¼ 223; aIRR, 1.93 [1.27–2.92]; P , 0.005), whereas we did not detect an association within the stratum of children with asthma by age 3 (n ¼ 42; aIRR, 0.83 [0.45–1.53]; P ¼ 0.55). Stratifying based on the child’s asthma status at age 7 showed similar results with a significant association in the subjects without asthma (n ¼ 204; aIRR, 1.90 [1.23–2.92]; P , 0.005), but no statistical evidence of association among subjects with asthma (n ¼ 33; aIRR, 0.96 [0.48–1.90]; P ¼ 0.89). Stratifying based on recurrent wheeze before age 7 confirmed a significant association among children without recurrent wheeze (n ¼ 174; aIRR, 1.85 [1.10–3.12]; P , 0.005), but no significant association among children with a history of recurrent wheeze (n ¼ 63; aIRR, 1.28 [0.76–2.18]; P ¼ 0.35). Bacterial versus Viral Pathogen
Microbiological sampling including bacterial cultures and virus detection by polymerase chain reaction was performed in 126 (39%) of 325 episodes of pneumonia and bronchiolitis (see Table E4). A total of 115 (91%) were positive for bacteria, 95 (75%) were positive for virus, and 86 (68%) were positive for
TABLE 1. ASSOCIATION BETWEEN COVARIATES AND INCIDENCE OF PNEUMONIA AND BRONCHIOLITIS Unadjusted IRR (95% CI) Boys Birth weight, kg Delivery by cesarean section Antibiotics in third trimester Maternal smoking in third trimester Older children in household at 1 yr Duration of breastfeeding (ref ¼ 0–3 mo) 3–6 mo More than 6 mo Nicotine, hair, 1 yr (in quartiles) Nicotine, hair, 3 yr (in quartiles) Cat at home at birth Dog at home at birth Father with asthma Daycare Age at start, d† Number of children in daycare† m2 per child† Household annual income, 100.000 dkr† Mother’s education (step 1–3) Mother’s employment (ref ¼ professional) Nonprofessional Student Unemployed
Adjusted* P Value
IRR (95% CI)
P Value
1.36 0.83 1.42 1.50 2.15 1.58
(1.01–1.83) (0.70–0.99) (1.03–1.97) (1.03–2.19) (1.54–2.99) (1.18–2.11)
0.05 0.04 0.03 0.03 ,0.005 ,0.005
1.43 0.82 1.43 1.24 1.80 1.55
(1.08–1.90) (0.63–1.08) (1.04–1.96) (0.86–1.78) (1.27–2.56) (1.17–2.06)
0.01 0.16 0.03 0.25 ,0.005 ,0.005
0.82 0.59 1.13 1.27 0.96 1.07 1.21
(0.50–1.32) (0.38–0.92) (0.98–1.29) (1.11–1.45) (0.62–1.49) (0.69–1.66) (0.84–1.74)
0.41 0.02 0.09 ,0.005 0.85 0.77 0.32
0.94 0.79 0.87 1.00 0.93 0.94 1.14
(0.59–1.51) (0.51–1.23) (0.74–1.02) (0.85–1.16) (0.61–1.42) (0.61–1.43) (0.80–1.61)
0.80 0.30 0.08 0.95 0.74 0.76 0.47
0.82 0.90 0.99 0.89 0.85
(0.68–0.99) (0.72–1.12) (0.91–1.07) (0.73–1.07) (0.68–1.06)
0.04 0.34 0.76 0.22 0.15
0.80 0.99 0.97 1.00 1.08
(0.67–0.95) (0.81–1.22) (0.90–1.06) (0.82–1.22) (0.84–1.39)
0.01 0.74 0.76 1.00 0.54
1.27 (0.90–1.78) 1.76 (1.09–2.82) 1.64 (1.02–2.65)
0.18 0.02 0.04
1.05 (0.74–1.47) 1.75 (1.11–2.76) 1.78 (1.13–2.81)
0.80 0.02 0.01
Definition of abbreviations: CI ¼ confidence interval; IRR ¼ incidence rate ratios. Significant values in bold. * Confounding variables: sex, birth weight, delivery by cesarean section, antibiotics in third trimester, smoking in third trimester, older siblings, breastfeeding, daycare attendance, and mother’s occupation. y IRR per interquartile range.
Vissing, Chawes, and Bisgaard: Neonatal Airway Colonization and Pneumonia and Bronchiolitis
1249
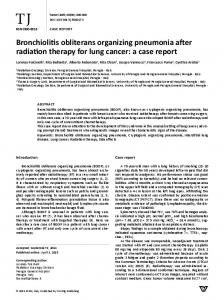
Figure 1. Cumulative risk of pneumonia and bronchiolitis during the first 3 years of life for children with and without neonatal airway colonization. HR ¼ hazard ratio.
virus and bacteria. Twenty-three (23%) were only positive for bacteria and nine (7%) were only positive for virus; only two samples (2%) were not positive for either virus or bacteria. Positive identification of bacteria and virus during episodes of pneumonia or bronchiolitis was equally frequent in samples from children with and without neonatal colonization, indicating that the increased risk of pneumonia and bronchiolitis is independent of pathogen (Table E4).
DISCUSSION Principal Findings
A disturbed airway microbiome in healthy neonates, as reflected by colonization with S. pneumoniae, H. influenzae, or M. catarrhalis, is associated with a twofold increased incidence of pneumonia and bronchiolitis during the first 3 years of life independently of current or later childhood asthma. Strengths and Limitations of the Study
The longitudinal design with comprehensive prospective data collection, clinical evaluations by doctors with pediatric training
at the single research site following standardized operating procedures, and symptom assessment supported by daily diaries enhanced the validity of data and allowed adjusting for a multitude of covariates relevant to incidence of pneumonia and bronchiolitis. This is particularly valuable when dealing with childhood respiratory infections that are assumed to have a multifactorial etiology and where diagnosis may require particular training. Likewise, diagnosing asthma in children can be difficult and there is gross inconsistency among community doctors in their diagnostic and treatment practice. Our single-center study design with a fixed algorithm for asthma diagnosis reduces this risk of misclassification. It is further a strength that we were able to stratify for asthma at two time points, before age 3 and at age 7, thereby diminishing the risk of our results being confounded by underlying asthmatic disease. It is a strength that variation in the neonatal microbiome was assessed in the target organ before occurrence of any respiratory symptoms was assessed. It is a limitation that we only cultured a limited number of bacterial species screening for common pathogenic bacteria. Unfortunately, DNA sequencing for the full
TABLE 2. BACTERIAL COLONIZATION AT FOUR WEEKS AND INCIDENCE OF PNEUMONIA AND BRONCHIOLITIS STRATIFIED BY ASTHMA DIAGNOSIS
One or more bacteria Analysis by species Haemophilus influenzae Moraxella catarrhalis Streptococcus pneumoniae Staphylococcus aureus Stratifying by asthma status Asthma before 3 yr Yes (n ¼ 42) No (n ¼ 223) Asthma at 7 yr Yes (n ¼ 33) No (n ¼ 204) Recurrent wheeze before 7 yr Yes (n ¼ 63) No (n ¼ 174)
Adjusted†
Unadjusted
No. of Cases/Control Subjects*
IRR
P Value
CI
IRR
P Value
CI
56 (21%)/209
1.94
,0.005
1.43–2.63
1.79
,0.005
1.29–2.48
(9%)/209 (8%)/209 (9%)/209 (62%)/101
2.31 1.91 1.71 1.04
,0.005 ,0.005 0.02 0.81
1.58–3.35 1.25–2.91 1.10–2.65 0.76–1.41
2.01 1.94 1.72 0.98
,0.005 0.01 0.02 0.88
1.41–3.13 1.20–3.12 1.07–2.75 0.73–1.31
18 (43%)/24 38 (17%)/185
1.10 1.83
0.69 ,0.005
0.69–1.75 1.26–2.66
0.83 1.93
0.55 ,0.005
0.45–1.53 1.27–2.92
12 (36%)/21 37 (18%)/167
1.39 1.82
0.29 ,0.005
0.76–2.67 1.24–2.57
0.96 1.90
0.89 ,0.005
0.48–1.90 1.23–2.92
41 (65%)/22 27 (17%)/147
1.46 1.59
0.12 0.048
0.91–2.33 1.00–2.53
1.28 1.85
0.35 0.02
0.76–2.18 1.10–3.12
25 22 24 164
Definition of abbreviations: CI ¼ confidence interval; IRR ¼ incidence rate ratios. Significant values in bold. * Control subjects: children without any colonization of the three species, H. influenzae, M. catarrhalis, or S. pneumoniae. y Included covariates: sex, birth weight, delivery by section, antibiotics in third trimester, smoking in third trimester, older siblings, breastfeeding, daycare attendance, and mother’s occupation.
1250
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Figure 2. Adjusted incidence risk ratio (aIRR) with confidence limits for pneumonia and bronchiolitis after neonatal colonization with Haemophilus influenzae, Moraxella catarrhalis, or Streptococcus pneumoniae as monoculture or coculture compared with no colonization with any of the species.
microbiome was not available at the time of birth of this cohort and no material was stored. Parents were primarily using our research center for diagnosis and treatment between regular visits and not the community doctor. However, some episodes of pneumonia and bronchiolitis were diagnosed outside COPSAC in pediatric emergency departments or by the families’ general practitioner. The validity of this part of the data was confirmed in a previous validation study (25), finding less than 4% missed diagnoses in the record of the families’ general practitioner. The reported incidence rates of pneumonia and bronchiolitis in young children vary greatly (13–64%) depending on study design and case definitions (10, 28–33). Our finding of 58% of children having at least one incidence of pneumonia or bronchiolitis corresponds well with two other community-based studies on pneumonia and bronchiolitis in birth cohorts with similar case definitions (10, 34). The generalizability of our findings is limited from the highrisk of asthma in the cohort. Children born of mothers with asthma and allergy have been shown to exhibit different innate immunity compared with children born of mothers without such disorders (35), and these infants may be more susceptible to the influence of early microbial exposures. Still, considering the high prevalence of asthma among adults of reproductive age in industrialized countries (36), our results are relevant to a substantial proportion of the population. Importantly, the association between the neonatal airway microbiome and the risk of pneumonia and bronchiolitis was stronger in the segment of children without asthma than in the segment with asthma. Interpretation
Our studies suggest that a disturbed microbiome in the neonatal airway increases risk of bronchiolitis and pneumonia and the risk
VOL 188
2013
of childhood asthma (13). The mechanism behind this shared association of the neonatal microbiome and later lung diseases is unknown. Bacterial colonization may have a direct causal effect. In line with this, we recently observed a perturbation of the cytokines and chemokines in the mucosal lining fluid in neonates colonized with pathogenic bacteria suggesting that the local microbiome activates an immune response and possibly affects the maturation of the adaptive immune system (15). Alternatively, such altered immune activity in colonized neonates may reflect a genetic predisposition for an inefficient mucosal immune defense of the airway increasing the risk for developing childhood asthma and bronchiolitis and pneumonia, in which case bacterial colonization of the neonatal airway is an epiphenomenon. Children on a trajectory to develop asthma may present with recurrent pneumonia and bronchiolitis (34), and particularly bronchiolitis has been associated with asthma (37). Thus, our findings could be caused by a common pathogenesis to asthma, and pneumonia and bronchiolitis or simply reflect a phenotypic characteristic of children with asthma that are known to have an altered airway microbiome (38). It is therefore important that the stratified analyses showed the association between pathogenic colonization and incidence of pneumonia and bronchiolitis was strengthened in the nonasthmatic strata. This shows that the effect from bacterial colonization on incidence of pneumonia and bronchiolitis is independent of asthma. The stratified analyses showed that the association between neonatal colonization and pneumonia and bronchiolitis was only evident among nonasthmatic children with no signal in the asthmatic strata. However, the majority of children with asthma experienced pneumonia or bronchiolitis within the first 3 years of life (Tables E2 and E3). Therefore, the numbers of children in the asthmatic strata without pneumonia and bronchiolitis are quite small (four children with asthma by age 3 and six children with asthma at age 7), and these numbers are most likely too low to detect an association between neonatal colonization and incidence of pneumonia and bronchiolitis. The lack of association between colonization with S. aureus and pneumonia and bronchiolitis suggests a species-specific effect from S. pneumoniae, H. influenzae, and M. catarrhalis. The effect of these pathogenic bacteria may act indirectly by competing with nonpathogenic bacteria, such as lactobacilli, which have been shown to be beneficial in mouse models for the development of appropriate immune responses toward respiratory pathogens (37, 39). Cesarean section was associated with a 1.5-fold increased incidence of pneumonia and bronchiolitis, supporting the hypothesis that alterations in the microbiome in early life affect pneumonia and bronchiolitis susceptibility. Similarly, an association between caesarean section and respiratory symptoms in early life has been reported (40), and infants born by cesarean section are colonized differently than children born naturally (41). Further studies are needed to pursue this link between the role of the human microbiome, immune maturation, and disease development. Conclusions
Healthy neonates colonized with S. pneumoniae, H. influenzae, or M. catarrhalis in the hypopharynx are at increased risk of pneumonia and bronchiolitis in the first 3 years of life independently of asthma. These findings support the possible role of the neonatal airway microbiome on immune maturation, and suggest that a disturbed microbiome may affect the immune maturation with increased risk of pneumonia and bronchiolitis. Author disclosures are available with the text of this article at www.atsjournals.org.
Vissing, Chawes, and Bisgaard: Neonatal Airway Colonization and Pneumonia and Bronchiolitis Acknowledgment: The authors thank the children and families of the Copenhagen Prospective Study on Asthma in Childhood2000 cohort study for all their support and commitment. They also acknowledge and appreciate the unique efforts of the Copenhagen Prospective Study on Asthma in Childhood research team.
References 1. Zutavern A, Rzehak P, Brockow I, Schaaf B, Bollrath C, von Berg A, Link E, Kraemer U, Borte M, Herbarth O, et al.; LISA Study Group. Day care in relation to respiratory-tract and gastrointestinal infections in a German birth cohort study. Acta Paediatr 2007; 96:1494–1499. 2. Nafstad P, Hagen JA, Botten G, Jaakkola JJ. Lower respiratory tract infections among Norwegian infants with siblings in day care. Am J Public Health 1996;86:1456–1459. 3. Cushing AH, Samet JM, Lambert WE, Skipper BJ, Hunt WC, Young SA, McLaren LC. Breastfeeding reduces risk of respiratory illness in infants. Am J Epidemiol 1998;147:863–870. 4. Nafstad P, Jaakkola JJ, Hagen JA, Botten G, Kongerud J. Breastfeeding, maternal smoking and lower respiratory tract infections. Eur Respir J 1996;9:2623–2629. 5. Koch A, Sørensen P, Homøe P, Mølbak K, Pedersen FK, Mortensen T, Elberling H, Eriksen AM, Olsen OR, Melbye M. Population-based study of acute respiratory infections in children, Greenland. Emerg Infect Dis 2002;8:586–593. 6. Ball TM, Castro-Rodriguez JA, Griffith KA, Holberg CJ, Martinez FD, Wright AL. Siblings, day-care attendance, and the risk of asthma and wheezing during childhood. N Engl J Med 2000;343:538–543. 7. Koopman LP, Smit HA, Heijnen ML, Wijga A, van Strien RT, Kerkhof M, Gerritsen J, Brunekreef B, de Jongste JC, Neijens HJ. Respiratory infections in infants: interaction of parental allergy, child care, and siblings. The PIAMA study. Pediatrics 2001;108:943–948. 8. Strachan DP, Cook DG. Health effects of passive smoking. 1. Parental smoking and lower respiratory illness in infancy and early childhood. Thorax 1997;52:905–914. 9. Thörn LKAM, Minamisava R, Nouer SS, Ribeiro LH, Andrade AL. Pneumonia and poverty: a prospective population-based study among children in Brazil. BMC Infect Dis 2011;11:180. 10. Kusel MM, de Klerk N, Holt PG, Landau LI, Sly PD. Occurrence and management of acute respiratory illnesses in early childhood. J Paediatr Child Health 2007;43:139–146. 11. Wegienka G, Havstad S, Zoratti EM, Woodcroft KJ, Bobbitt KR, Ownby DR, Johnson CC. Regulatory T cells in prenatal blood samples: variability with pet exposure and sensitization. J Reprod Immunol 2009;81:74–81. 12. Ege MJ, Bieli C, Frei R, van Strien RT, Riedler J, Üblagger E, SchramBijkerk D, Brunekreef B, van Hage M, Scheynius A, et al.; Parsifal Study team. Prenatal farm exposure is related to the expression of receptors of the innate immunity and to atopic sensitization in schoolage children. J Allergy Clin Immunol 2006;117:817–823. 13. Bisgaard H, Hermansen MN, Buchvald F, Loland L, Halkjaer LB, Bønnelykke K, Brasholt M, Heltberg A, Vissing NH, Thorsen SV, et al. Childhood asthma after bacterial colonization of the airway in neonates. N Engl J Med 2007;357:1487–1495. 14. Von Linstow M-L, Schønning K, Hoegh AM, Sevelsted A, Vissing NH, Bisgaard H. Neonatal airway colonization is associated with troublesome lung symptoms in infants. Am J Respir Crit Care Med 2013;188:1041–1042. 15. Følsgaard NV, Schjørring S, Chawes BL, Rasmussen MA, Krogfelt KA, Brix S, Bisgaard H. Pathogenic bacteria colonizing the airways in asymptomatic neonates stimulates topical inflammatory mediator release. Am J Respir Crit Care Med 2013;187:589–595. 16. Vissing NH, Chawes BLK, Bisgaard H. Increased risk of lower respiratory tract infections after bacterial colonization of the airways in neonates. Presented at the Danish Society for Paediatric Infectious Diseases annual meeting. October 5, 2012, Korsør, Denmark. Poster presentation. 17. Bisgaard H. The Copenhagen Prospective Study on Asthma in Childhood (COPSAC): design, rationale, and baseline data from a longitudinal birth cohort study. Ann Allergy Asthma Immunol 2004;93:381–389.
1251
18. Bisgaard H, Pipper CB, Bønnelykke K. Endotyping early childhood asthma by quantitative symptom assessment. J Allergy Clin Immunol 2011;127:1155–1164.e2. 19. Halkjaer LB, Loland L, Buchvald FF, Agner T, Skov L, Strand M, Bisgaard H. Development of atopic dermatitis during the first 3 years of life: the Copenhagen Prospective Study on Asthma in Childhood cohort study in high-risk children. Arch Dermatol 2006; 142:561–566. 20. Bisgaard H, Hermansen MN, Bønnelykke K, Stokholm J, Baty F, Skytt NL, Aniscenko J, Kebadze T, Johnston SL. Association of bacteria and viruses with wheezy episodes in young children: prospective birth cohort study. BMJ 2010;341:c4978. 21. Bisgaard H, Bønnelykke K, Sleiman PMA, Brasholt M, Chawes B, Kreiner-Møller E, Stage M, Kim C, Tavendale R, Baty F, et al. Chromosome 17q21 gene variants are associated with asthma and exacerbations but not atopy in early childhood. Am J Respir Crit Care Med 2009;179:179–185. 22. Bønnelykke K, Pipper CB, Tavendale R, Palmer CNA, Bisgaard H. Filaggrin gene variants and atopic diseases in early childhood assessed longitudinally from birth. Pediatr Allergy Immunol 2010;21: 954–961. 23. Loland L, Buchvald FF, Halkjaer LB, Anhøj J, Hall GL, Persson T, Krause TG, Bisgaard H. Sensitivity of bronchial responsiveness measurements in young infants. Chest 2006;129:669–675. 24. Bisgaard H, Hermansen MN, Loland L, Halkjaer LB, Buchvald F. Intermittent inhaled corticosteroids in infants with episodic wheezing. N Engl J Med 2006;354:1998–2005. 25. Chawes BLK, Poorisrisak P, Johnston SL, Bisgaard H. Neonatal bronchial hyperresponsiveness precedes acute severe viral bronchiolitis in infants. J Allergy Clin Immunol 2012;130:354–361.e3. 26. Vissing NH, Jensen SM, Bisgaard H. Validity of information on atopic disease and other illness in young children reported by parents in a prospective birth cohort study. BMC Med Res Methodol 2012;12: 160. 27. Al-Delaimy WK, Crane J, Woodward A. Is the hair nicotine level a more accurate biomarker of environmental tobacco smoke exposure than urine cotinine? J Epidemiol Community Health 2002;56:66–71. 28. Celedon JC, Litonjua AA, Weiss ST, Gold DR. Day care attendance in the first year of life and illnesses of the upper and lower respiratory tract in children with a familial history of atopy. Pediatrics 1999;104: 495–500. 29. Holberg CJ, Wright AL, Martinez FD, Morgan WJ, Taussig LM; Group Health Medical Associates. Child day care, smoking by caregivers, and lower respiratory tract illness in the first 3 years of life. Pediatrics 1993;91:885–892. 30. Schwartz B, Giebink GS, Henderson FW, Reichler MR, Jereb J, Collet JP. Respiratory infections in day care. Pediatrics 1994;94:1018–1020. 31. Ramsey CD, Gold DR, Litonjua AA, Sredl DL, Ryan L, Celedón JC. Respiratory illnesses in early life and asthma and atopy in childhood. J Allergy Clin Immunol 2007;119:150–156. 32. Horwood LJ, Fergusson DM, Shannon FT. Social and familial factors in the development of early childhood asthma. Pediatrics 1985;75:859– 868. 33. Wright AL, Taussig LM, Ray CG, Harrison HR, Holberg CJ. The Tucson Children’s Respiratory Study. II. Lower respiratory tract illness in the first year of life. Am J Epidemiol 1989;129:1232– 1246. 34. Illi S, von Mutius E, Lau S, Bergmann R, Niggemann B, Sommerfeld C, Wahn U; MAS Group. Early childhood infectious diseases and the development of asthma up to school age: a birth cohort study. BMJ 2001;322:390–395. 35. Følsgaard NV, Chawes BL, Rasmussen MA, Bischoff AL, Carson CG, Stokholm J, Pedersen L, Hansel TT, Bønnelykke K, Brix S, et al. Neonatal cytokine profile in the airway mucosal lining fluid is skewed by maternal atopy. Am J Respir Crit Care Med 2012;185: 275–280. 36. Svanes C, Jarvis D, Chinn S, Burney P. Childhood environment and adult atopy: results from the European Community Respiratory Health Survey. J Allergy Clin Immunol 1999;103:415–420. 37. Gabryszewski SJ, Bachar O, Dyer KD, Percopo CM, Killoran KE, Domachowske JB, Rosenberg HF. Lactobacillus-mediated priming
1252
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
of the respiratory mucosa protects against lethal pneumovirus infection. J Immunol 2011;186:1151–1161. 38. Hilty M, Burke C, Pedro H, Cardenas P, Bush A, Bossley C, Davies J, Ervine A, Poulter L, Pachter L, et al. Disordered microbial communities in asthmatic airways. PLoS ONE 2010;5:e8578. 39. Villena J, Oliveira MLS, Ferreira PCD, Salva S, Alvarez S. Lactic acid bacteria in the prevention of pneumococcal respiratory infection: future opportunities and challenges. Int Immunopharmacol 2011;11:1633–1645.
VOL 188
2013
40. Magnus MC, Håberg SE, Stigum H, Nafstad P, London SJ, Vangen S, Nystad W. Delivery by cesarean section and early childhood respiratory symptoms and disorders: the Norwegian Mother and Child cohort study. Am J Epidemiol 2011;174:1275–1285. 41. Dominguez-Bello MG, Costello EK, Contreras M, Magris M, Hidalgo G, Fierer N, Knight R. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns. Proc Natl Acad Sci USA 2010;107:11971–11975.