Metab Brain Dis DOI 10.1007/s11011-017-0050-0
REVIEW ARTICLE
Insulin resistance in ischemic stroke Xiao-Ling Deng 1 & Zhou Liu 2 & Chuanling Wang 3 & Yanfeng Li 4 & Zhiyou Cai 5
Received: 29 March 2017 / Accepted: 6 June 2017 # Springer Science+Business Media, LLC 2017
Abstract Insulin resistance often refers to a pathological condition in which cells fail to respond to the normal actions of insulin. Increasing literature has noted a critical role of insulin resistance in the pathogenesis of ischemic stroke. Insulin resistance plays an important role in the pathogenesis of ischemic stroke via enhancing advanced changes of atherosclerosis. A variety of literature indicates that insulin resistance enhances platelet adhesion, activation and aggregation which are conducive to the occurrence of ischemic stroke. Insulin resistance also induces hemodynamic disturbances and contributes to the onset of ischemic stroke. In addition, insulin resistance may augment the role of the modifiable risk factors in ischemic stroke and induce the occurrence of ischemic stroke. Xiao-Ling Deng and Zhou Liu contributed equally to this work. * Yanfeng Li
[email protected] * Zhiyou Cai
[email protected] 1
Department of Neurology, Renmin Hospital, Hubei University of Medicine, Shiyan Renmin Hospital, Shiyan 442000, Hubei Province, People’s Republic of China
2
Department of Neurology, The Affiliated Hospital of Guangdong Medical University, and Institute of Neurology, Guangdong Medical University, Zhanjiang, Guangdong Province, People’s Republic of China
3
Department of Pathology, Chongqing Medical University, Chongqing 400016, People’s Republic of China
4
Department of Neurology, Peking Union Medical College Hospital, No.1 Shuaifuyuan Wangfujing, Dongcheng District, Beijing 100730, People’s Republic of China
5
Department of Neurology, Chongqing General Hospital, No. 312 Zhongshan First Road, Yuzhong District, Chongqing 400013, People’s Republic of China
Preclinical and clinical studies have supported that improving insulin resistance may be an effective measure to prevent or delay ischemic stroke. Keywords Ischemic stroke . Insulin resistance . Atherosclerosis . Risk factor
Introduction Stroke is known as acute cerebrovascular accident when poor blood flow to the brain results in cell death, including ischemic stroke (due to lack of blood flow) and hemorrhagic stroke (due to bleeding). Stroke is the leading cause of death and the leading cause of chronic disability in China, and the second leading cause of long-term disability and death worldwide (Snarska et al. 2017). A high burden of stroke worldwide is largely due to failed management and prevention of modifiable risk factors, especially the ischemic stroke which accounts for more that 70% of total stroke. The identification and prevention of modifiable risk factors can decrease the likelihood of ischemic stroke, and reduce long-term morbidity and mortality after stroke or transient ischemic attack, and lower health care expenditure (Flemming and Brown 2004). Several well-established and modifiable risk factors for ischemic stroke include hypertension (Sarfo et al. 2014), atrial fibrillation (Jimenez-Caballero et al. 2013; Kwon et al. 2016), hyperlipidemia (Pikija et al. 2015), diabetes (Danaei et al. 2009; Lv et al. 2013), cigarette smoking and alcohol abuse (Kwon et al. 2016), physical inactivity (Sarfo et al. 2014), obesity (Sarfo et al. 2014), acute stress (Mandic and Rancic 2011), poor diet and other lifestyle risk factors (Goldstein et al. 2006; Pikija et al. 2015; von Sarnowski et al. 2013). Insulin resistance includes both physiological and pathological metabolic changes (Rendschmidt et al. 2000).
Metab Brain Dis
However, insulin resistance is often identified as a pathological condition in which cells fail to respond to the normal actions of the hormone insulin (Dali-Youcef et al. 2013). Cells resistant to insulin are unable to utilize it as effectively, leading to elevated blood sugar. Mounting results have noted that insulin resistance is an independent risk factor in ischemic stroke. Insulin resistance facilitates the onset of ischemic stroke since it accelerates atherosclerosis (Dandona et al. 2003; Fitzgibbons and Czech 2016; Gast et al. 2013; Park et al. 2008; Slyper et al. 2014), induces hemodynamic disturbances in ischemic stroke (Hilsted et al. 1984; Kain et al. 2003), promotes platelet adhesion, activation and aggregation which are all associated with ischemic stroke (Kain et al. 2003; Perez et al. 2012; Vazzana et al. 2012), and magnifies the role of risk factors in ischemic stroke (Tanne et al. 2009). This review focuses on the role of insulin resistance in ischemic stroke. The discussion has been made that insulin resistance is conducive to the pathogenesis of ischemic stroke via atherosclerosis. An overview has been provided for the proposed general pathogenic mechanism of insulin resistance in ischemic stroke via inducing hemodynamic disturbances in ischemic stroke. It has been also discussed that insulin resistance may promote platelet adhesion, activation and aggregation which are associated with ischemic stroke, and amplify the role of risk factors in ischemic stroke. Finally, we have also looked into the future that it is possibly an effective measure to improve insulin resistance state as an attractive target for the prevention and treatment of ischemic stroke.
Insulin resistance Insulin (from the Latin, insula meaning island), a peptide hormone (51 amino acids in an insulin molecule), is produced by the beta cells of the pancreas which are scattered throughout the pancreas in small clusters known as the islets of Langerhans. Insulin provides the cells to uptake glucose from blood and transport glucose into glycogen that can be stored in the liver and muscles. Insulin can prevent the fat utilization as an energy source. The most important role of insulin among several functions is controlling blood sugar. It helps the cells of your body remove glucose from your bloodstream. This glucose fuels cells and offers the energy to work properly for cells (Fedorova et al. 2007; Gebel 2011; Teesalu et al. 1981). Insulin resistance is an abnormal condition in which cells have a decreased ability to respond to insulin. Insulin resistance is a state that a given amount of insulin brings forth a less than corresponding biological consequence. When human cells fail to respond accurately and adequately to circulating insulin, hyperglycemia will occur in people with insulin resistance. Insulin resistance individuals require higher than normal amounts of insulin (hyperinsulinemia) to maintain normal blood glucose concentrations. If the hyperinsulinemia is efficient to surmount
the insulin resistance, glucose metabolism is maintained within normal range; otherwise, type 2 diabetes mellitus ensues (Lebovitz and Banerji 2001). Insulin resistance comes about furtively and silently. Once insulin resistance is established, additional resistance develops over time. Compelling literature has displayed that insulin resistance has been identified as a risk factor for diabetes (Luchsinger 2010; Pires et al. 2015; Tangvarasittichai 2015), hypertension (Ma et al. 2015; Manucha et al. 2015; Soleimani 2015; Zhi et al. 2015), dyslipidemia (Kishida et al. 2015; Tangvarasittichai 2015), metabolic Syndrome (Ebron et al. 2015), cardiovascular diseases (Saitoh 2006; Tack et al. 1992; Zethelius and Cederholm 2015), cerebrovascular diseases (Luchsinger 2010; Rodriguez-Flores et al. 2014; Tanne et al. 2009), neurodegenerative diseases (Luchsinger 2010; Morris et al. 2014; Schubert et al. 2004) and other disorders (Kain et al. 2001). Available studies have revealed that ischemic stroke shares several pathogenic backgrounds with diabetes, including impaired insulin signaling, chronic hyperinsulinemia and insulin resistance, as well as insulin resistance-related inflammation and oxidative stress (Luchsinger 2010; Manucha et al. 2015; Victor 2013).
The detrimental role of hyperglycemia in ischemic stroke Inceasing available evidence has shown that hyperglycemia is detrimental in acute ischemic stroke (Gofir et al. 2017; Ntaios et al. 2011; Snarska et al. 2017). Hyperglycemia may predict a larger infarct size, poor clinical outcome and a higher risk of mortality in the patients of ischemic stroke (Luitse et al. 2017; Snarska et al. 2017; Zonneveld et al. 2017). Various pathophysiological mechanisms have been proposed to account for the detrimental role of hyperglycemia in ischemic stroke. Hyperglycemia facilitates a pro-oxidative and proinflammatory state that can cause mitochondrial dysfunction and direct neuronal toxicity (Bevers et al. 2016; Khan et al. 2016; Zhang et al. 2013; Zhou et al. 2015). Hyperglycemia may destroy the normal structure of blood-brain barrier (BBB), and cause neuronal damage by an increase in cerebral edema (Zhang et al. 2016). Hyperglycemia can impair micro- and macro-vascular structures, thereby contributing to ischemic stroke (Coucha et al. 2015). In addition, hyperglycemia may promote a procoagulant state that can further compromise blood supply to the penumbral areas in ischemic stroke (Els et al. 1997; Gentile et al. 2007; Rosso et al. 2015).
Insulin resistance facilitates ischemic stroke via atherosclerosis Increasing data from clinical and basic results has evidenced that atherosclerosis is the leading cause of ischemic stroke
Metab Brain Dis
despite the management of critical risk factors from significant progress. It has been well clarified that roles of atherosclerosis in ischemic stroke have been associated with insulin resistance itself and insulin resistance-related diseases, including diabetes (Kostiuk and Zubkova 1993), coronary heart disease (Laakso et al. 1991; Posadas-Romero et al. 2014), and stroke (Dearborn et al. 2015). Furthermore, compelling evidence in both animal and human studies have displayed that insulin resistance contributes to the pathogenesis of ischemic stroke via enhancing the formation of atherogenesis and advanced plaque in the progression of atherosclerosis (Park et al. 2008). Atherosclerosis is a patho-physiological progress of hardening and narrowing of the arteries which are blood vessels that carry oxygen-rich blood to your brain and other parts of your body. This progressive process silently and slowly leads to stenosis of arteries and gradually induces blood flow at risk. It is well known that atherosclerosis is the usual cause of heart attacks, strokes, and peripheral vascular disease, which can lead to serious problems, including heart attack, stroke, or even death (Dearborn et al. 2015; Gaggini et al. 2013). An increasing number of studies have demonstrated that atherosclerosis is a pathological change and patho-physiological course of cerebral ischemic diseases in which plaque builds up inside cerebral arteries (Calleja et al. 2011; Hankey and Feng 2010; Hishinuma et al. 2009; Katsumata et al. 2010; Park et al. 2008; Shinozaki et al. 1996; Urabe et al. 2009). Abundant evidence in the past few decades has supported a striking relation between insulin resistance and atherosclerosis where insulin resistance has been proposed to contribute to the pathogenesis of atherosclerosis (Kostiuk and Zubkova 1993; Sowers et al. 1993; Tian et al. 2016). Epidemiological investigations indicated the role of hyperinsulinaemia as an independent risk factor in the development of atherosclerosis (Spustova 1992). Insulin resistance can accelerate the formation of atherogenesis and advanced plaque in the progression of atherosclerosis (Bansilal et al. 2007; Yang et al. 2005), involving a proinflammatory state (Yang et al. 2011) and perturbed insulin signaling at the level of the intimal cells that participate in atherosclerosis, including endothelial cells, vascular smooth muscle cells, and macrophages (Bornfeldt and Tabas 2011; Oh et al. 2015). It has been represented that the inflammatory response triggered by insulin resistance contributes to the progression of atherosclerosis. Insulin resistance can enhance chronic systemic inflammation (Stohr and Federici 2013), low insulin sensitivity, increase foam cell formation, and accelerate atherosclerosis (Oh et al. 2015). It has been evidenced that insulin resistance increases the pathologic process of vascular endothelia dysfunction, macrophages and smooth muscle cells in the development of atherosclerosis via inflammation (Ning et al. 2015). Multivariate analysis illustrated that insulin resistance was an independent predictor of intracranial atherosclerosis and insulin resistance enhances the formation of intracranial
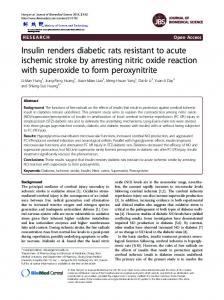
atherosclerosis in patients with acute ischemic stroke without diabetes (Park et al. 2008). Impaired glucose tolerance and insulin resistance could play an important pathogenic role in the development of atherothrombotic infarction (Urabe et al. 2009). Insulin resistance in combination with decreased insulin secretion may be associated with ischemic stroke recurrence on the basis of further increase of atherosclerosis and atherosclerotic stenosis (Hishinuma et al. 2009). A basic data indicated that insulin resistance elevated concentrations of very-low density lipoproteins (VLDL) which was related with the development of atherosclerotic disease and ischemic stroke (Russell et al. 1987). Available epidemiological study has implicated that insulin resistance is related to low high-density lipoprotein (HDL) cholesterol and high VLDL triglyceride levels which accelerate the progress of atherosclerosis (Laakso 1992). Insulin resistance may directly enhance the process of atherosclerosis by facilitating LDL-cholesterol accumulation in vessel walls, migration and proliferation of vascular smooth muscle cells, and amplifying connective tissue synthesis in the vascular wall, and finally bringing about the onset of cerebral ischemic diseases (Sowers 1992). A pilot clinical trial supports that insulin resistance might exert their atherogenic impact through the impaired fibrinolysis (Jotic et al. 2015). The main possible mechanisms of insulin resistance in ischemic stroke via atherosclerosis may include the following (Fig. 1): &
&
&
Insulin resistance contributes to the endothelium dysfunction and the formation of foam cells via enhancing the process from monocyte to macrophage in the initiation of atherosclerosis which is closely related with ischemic stroke (Busija and Katakam 2014; Dorrance et al. 2014; Muniyappa and Quon 2007; Roitberg et al. 2005). Insulin resistance facilitates the formation of fatty streak (more foam cells), and migration and proliferation of vascular smooth muscle cells in the early lesion of atherosclerosis which is closely related with ischemic stroke (Busija and Katakam 2014; Kernan and Inzucchi 2004). Insulin resistance promotes the formation of vulnerable plaque and replication of vascular smooth muscle cells in the late lesion of atherosclerosis which is closely related with ischemic stroke. Finally, insulin resistance leads to vascular surface defect, apoptosis of vascular smooth muscle cells, necrosis of plaque, the ruputure of fibrous cap, and thrombosis (Beckman et al. 2002; Dentali et al. 2009; Park et al. 2008; Shinozaki et al. 1996).
Platelet aggregation from insulin resistance Strong data has emerged to support that platelet adhesion, activation and aggregation are conducive to the occurrence
Metab Brain Dis
Fig. 1 The possible mechanisms of insulin resistance (IR) in ischemic stroke via atherosclerosis. a IR contributes to the endothelium dysfunction and the formation of foam cells via enhancing the process from monocyte to macrophage in the initiation of atherosclerosis which is closely related with ischemic stroke. b IR facilitates the formation of fatty streak (more foam cells) and migration and proliferation of vascular smooth muscle cells in the early lesion of atherosclerosis which is
closely related with ischemic stroke. c IR promotes the formation of vulnerable plaque and replication of vascular smooth muscle cells, and leads to vascular surface defect, apoptosis of vascular smooth muscle cells, necrosis of plaque, the ruputure of fibrous cap and thrombosis in the late lesion of atherosclerosis which is closely related with ischemic stroke
of ischemic stroke (Das 2010). Generally, ischemic stroke is believed to come into being associated with one of two processes: the activation of platelets leading to thromboembolic events, and plaque rupture in the cerebral arterial circulation resulting in the clot formation. Interventions that arrest the activation of platelets and the formation of thrombi from ruptured plaques have been proposed to decrease the incidence and severity of acute ischemic stroke. It has been well evidenced that platelet aggregation from insulin resistance is associated thrombotic complications (Das 2010; Paneni et al. 2013; Singh et al. 2015; Vazzana et al. 2012). A number of research results have demonstrated that insulin resistance plays an important role in platelet adhesion, activation and aggregation which are associated with occlusion of diseased vessels and involved in ischemic cardiovascular events and ischemic stroke incidence (Fig. 2) (De Vecchis et al. 2016; Ferreiro et al. 2010; Moore et al. 2015; Santilli et al. 2012; Ueno et al. 2015). A number of mechanisms involved in platelet dysfunction and affect the adhesion, activation and, aggregation phases of platelet-mediated thrombosis has been done (Ferreiro and Angiolillo 2012). Further mechanism research implicates that insulin resistance may increase platelet count and volume, and promote the action
of insulin on platelet signaling and function through inducing insulin-like growth factor-1 (IGF-1)- and insulin-like growth factor-2 (IGF-2)-mediated phosphorylation of IRS-1, Akt, and GSK3beta and priming of CRP-mediated platelet activation (Moore et al. 2015), and cGMP- and NO-dependent mechanisms in the insulin-mediated platelet aggregation (Randriamboavonjy and Fleming 2009; Suslova et al. 2014; Vignini et al. 2008). Insulin resistance is associated with the abnormalities of vascular endothelium which play an important role in increased platelet adhesion and aggregation in patients with ischemic stroke (Saboor et al. 2014). Several research studies have found that ischemic stroke is related to platelet aggregation caused from insulin resistance (Bondarenko et al. 2014; Lundstrom et al. 2014). A cohort study found that glucose intolerance and/or high level of insulin resistance was a pre-requisite for high on-treatment platelet reactivity (HPR), indicating that glucose intolerance and/or high level of insulin resistance may be identified as predictors of low platelet response to inhibitors of platelet aggregation in patients with minor ischemic stroke or transient ischemic attack (Lundstrom et al. 2014). Increasing data has shown that insulin resistance is a thrombogenic risk that causes platelet hyperaggregation, hypercoagulation, and
Metab Brain Dis Fig. 2 Platelet aggregation from insulin resistance in ischemic stroke
hyperfibrinolysis, leading to thromboembolic events (Suslova et al. 2014). It has been found that insulin resistance leads to platelet activation in the patients with metabolic syndrome and type 2 diabetes mellitus, relating with hyperglycemia, nonenzymatic glycosylation, oxidative stress, and inflammation (NO-mediated signaling pathway in the effects of cytokines on platelet aggregation) (Prakash et al. 2014; Suslova et al. 2014). A recent multivariable logistic regression analysis showed that patients with impaired glucose tolerance (IGT) and insulin resistance status are the strongest predictor of platelet aggregation. In this investigation, profiles of platelet reactivity were proportional to insulin resistance status while there was a significant reduction in the non-IR patients. These findings implicate that the presence of platelet dysfunction in patients with IGT may be attributed to the presence of insulin resistance (Ueno et al. 2015). Moreover, insulin resistance helps forward the interact between activated platelets with endothelial cells and leukocytes in the genesis of atherosclerosis which is the most obvious mechanism in ischemic stroke (Saboor et al. 2014). A cross-sectional study performed in 159 obese Chinese adolescents pointed to the notion that insulin resistance is a major determinant of platelet activation in Chinese obese adolescents via engaging in research into platelet activity using anthropometrics and biochemical parameters, oral glucose tolerance test and platelet testing (Lu et al. 2014). It has a well interpretation that platelet hyperreactivity is a major relevance in ischemic stroke as a key role in the development of atherosclerosis and its atherothrombotic
complications (Rao 2011). It has been evidenced that several intervention agents of platelet hyperreactivity are favourable towards a reduction in cardiovascular events and strokes through improving insulin resistance, decreasing lipid oxidation and inflammation, and limiting platelet aggregation (Paillard 2014), such as clopidogrel (Hillegass et al. 2011; Lundstrom et al. 2014; Ueno et al. 2015), aspirin (Hillegass et al. 2011; Kaplon-Cieslicka et al. 2013; Rao 2011), metformin (Randriamboavonjy et al. 2015), pioglitazone (Chen et al. 2013), methotrexate (at low doses) (De Vecchis et al. 2015), epinephrine (Perez-Campos-Mayoral et al. 2014), and even improvement of lifestyle, blood pressure and dyslipidemia control (Cosmi and Cosmi 2010), and some drinking and food (chocolate consumption, omega-3 fatty acids, grape products) (El-Gendy and Abbas 2014; Ferri et al. 2015; Paillard 2014; Perez-Jimenez and Saura-Calixto 2008).
Insulin resistance induces hemodynamic disturbances It has been recognized that the hemodynamic disturbances of cerebral perfusion is a primary cause of stroke. Moreover, the hemodynamic disturbances can cause a more severe course and worse stroke outcome during acute ischemic stroke (Bas et al. 2016). A growing number of results provide feedback that the cerebral hypotension brings out hemodynamic changes and finally results in the occurrence of ischemic stroke beyond the autoregulation of cerebral blood flow (Chantler
Metab Brain Dis
et al. 2015; Chazova et al. 2005; Reikeras and Gunnes 1986). It is an essential neuro-protective mechanism against cerebral ischemic that the capacity of regulating cerebral blood flow is to meet brain metabolic demands and to compensate for acute and chronic changes in cerebral perfusion (Kang et al. 2014; Kolbitsch et al. 2002; Ohashi et al. 2005). A large number of evidence-based research materials have pointed to the knowledge that IR is associated with cerebrovascular reserve (CVR) as an important index of evaluating cerebral blood flow and the capacity of regulating cerebral blood flow. CVR indicates the capacity of the brain to increase cerebral blood volume (CBV) to safeguard a constant regional cerebral blood flow (rCBF) in the face of low cerebral perfusion pressure (CPP) while rCBF is determined by the ratio of CPP to cerebrovascular resistance. Cerebral ischemic occurs when rCBF values fall below 20 ml/100 g/min, and cerebral infarction develops at rCBF levels