International Journal of Adolescence and Youth
ISSN: 0267-3843 (Print) 2164-4527 (Online) Journal homepage: http://www.tandfonline.com/loi/rady20
Knowledge and Attitudes Towards HIV/STD Among Indian Adolescents Syed N. Khalil , Michael W. Ross , Mathai Rabia & Subhash Hira To cite this article: Syed N. Khalil , Michael W. Ross , Mathai Rabia & Subhash Hira (2005) Knowledge and Attitudes Towards HIV/STD Among Indian Adolescents, International Journal of Adolescence and Youth, 12:1-2, 149-168, DOI: 10.1080/02673843.2005.9747948 To link to this article: http://dx.doi.org/10.1080/02673843.2005.9747948
Copyright Taylor and Francis Group, LLC
Published online: 27 Mar 2012.
Submit your article to this journal
Article views: 115
View related articles
Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=rady20 Download by: [192.30.84.32]
Date: 19 December 2016, At: 09:05
International Journal of Adolescence and Youth, 2005, Volume 12, pp. 149-168 0267-3843/05 $10 © 2005 A B Academic Publishers Printed in Great Britain
Knowledge and Attitudes Towards HIV/STD Among Indian Adolescents Syed N. Khalil,* Michael W. Ross,** Mathai Rabia,t Subhash Hira* ABSTRACT This is a secondary data set of a study conducted in 1996 among 1230 Indian students in the 11th and 12th grades in Bombay. The aim of the study is to examine the relationship of knowledge, health beliefs, attitudes, and risk behaviors to HIV /STD risk intentions among Indian adolescents and also to examine predictive utility of the Health Belief Model (HBM). Correlations, multiple regression, and logit regression were applied to predict the variables related to the HBM dimensions. The overall explanatory power of the models for either dimension of the HBM or preventive intention with knowledge about HIV /STD was modest. These results suggest that either the models are lacking some important variables or the measurement of key variables is inadequate. Another limitation is that the data collection tool was a secondary subset, and only some relevant questions were chosen to examine the aim of the study. The HBM is partially, but significantly, related to the likelihood of recommendation of preventive intention changes. Individual perception of a disease is more likely to depend upon the language spoken at home because Indian adolescents may assimilate health messages more completely when those messages are conveyed in the local language. Parent education levels do not influence preventive intention changes. However, it was observed that a low level of maternal education encouraged children's preventive intention. Girls especially have shown a higher intention to practice safer sex behaviors. Knowledge about HIV I STD appears to influence preventive intention to practice safer sex behaviors. It is very important to teach Indian adolescents the proper use of condoms, and such education should be given in the local language. Indian male adolescents are more likely to report that they engage in risky behavior than female adolescents. Indian adolescents need greater access to relevant health education. "University of Texas, School of Public Health; Project Coordinator, Houston Tuberculosis Initiative project at Baylor College of Medicine, Houston, TX. Email:
[email protected] ""Professor, WHO, Center for Health Promotion and Prevention Research, University of Texas School of Public Health, Houston, TX. tproject Director, International Red Cross, Washington, DC. *Professor, University of Texas School of Public Health,Houston, TX and Director, AIDS Research and Control Center, Mumbai, India.
150 INTRODUCTION India is a major epicenter of the AIDS pandemic (UNAIDS, & WHO, 1996). This epidemic has exploded since the discovery of the first case in 1986 (Ambati et al., 1997; Bollinger et al., 1995; Jain et al., 1994). Heterosexual transmission is the major mode of HIV I STD transmission in India. However, injection drug user (IDU)-related HIV is concentrated in certain pockets in the Northeastern part of India· (Mathai et al., 1997). In India the epidemic may ultimately be more damaging than elsewhere because of the overcrowding, poverty, lack of sanitation, and other factors common to developing countries (Brown and Xenos, 1994). It is, therefore, essential to examine the knowledge and attitudes of vulnerable groups in order to formulate effective strategies to combat HIV ISTDs transmission. Adolescents have been identified as an elevated risk group for HIV infection based on their lack of knowledge about HIVprevention practices (DiClemente et al., 1988; DiClemente et al., 1986, 1987a; Strunin and Hingson, 1987) and high-risk sexual and drug-related behaviors (Bell and Hein, 1984; Bell and Holmes, 1984; DiClemente, 1990). Recent data suggests that many adolescents do not engage in self-protective sexual practices (Kegeles et al., 1988; Strunin and Hingson, 1987), and have multiple sexual partners (Baldwin and Baldwin, 1988; Earle and Perricone, 1986; Kipnis et al., 1988). The prevalence of HIV ISTD infection among Indian adolescents is undetermined: a review of literature on the epidemiology of AIDSIHIV sero-prevalence and HIV incidence among Indian adolescents reveals that there is very limited data available for this group. According to available surveillance data the HIV seropositive rate in India is 21.05 per 1000. A major focus of infection is the India's financial capital Bombay, (now Mumbai, Maharastra), where the present study was conducted. An HIV prevalence rate of 11.74 per 1000-blood units was recorded in 1995 (Directorate of Health Service, Maharastra), but recent reports suggest that there has been a rapid rise in HIV prevalence since then (UNAIDS and WHO, 1996). Thus, there is little reliable or accurate information about the demographics of HIV ISTD seroprevalence in India and even less about adolescents' awareness of the disease. This is alarming since an understanding of the distribution, knowledge, behavior, and attitudes of the populace is a prerequisite to inhibiting the spread of the disease. Much of the available literature related to adolescents and HIV I AIDS is based on the USA and Europe. Little work has been based
151
on the Health Belief Model in south Asian adolescents. However, a study conducted (Yep, 1993) among Asian-American college students in Los Angeles on HIV prevention reveals that "perceived severity" and "perceived barriers" were significant predictors of the adoption of HIV-preventive behavior in this group. "Perceived severity" was a significant predictor of becoming more careful about the selection of intimate partners, reducing the number of sexual partners, and making a positive change toward safer sexual behaviors whereas "perceived barriers" was a significant predictor of becoming more careful about selection of intimate partners, reducing number of sexual partners, and ensuring that sexual partners were not HIV infected. There are a few published, and some unpublished, studies that have assessed the knowledge, attitude, and risk practice for HIV I STD among Indian adolescents which indicate the need for education programs to help these adolescents acquire the knowledge and skills to adopt and maintain behaviors that diminish the risk of HIV ISTD infection. Various studies have found that a limited knowledge of HIV ISTD does not significantly affect the attitude and behavior of adolescents (Mkumba, et al., 1993; Brown and Fritz, 1998; Weisman et al., 1989). Indian adolescents have a lot of misconceptions about HIV ISTD (Varma et al., 1989; Bhatlavande et. al., 1994; Sharma et al., 1994; Kumar et al., 1996). In a study of second year Indian medical students, Purohit (1994) reveals that a majority of the students had some misconceptions and lacked knowledge regarding the relationship of semen infected with HIV and transmission of the virus through sexual intercourse. Indian adolescents have very limited knowledge about human sexuality and AIDS; however, males have more knowledge about AIDS than females (Tikoo et al., 1995). A study showing differences in knowledge and attitudes toward HIV I AIDS between university students of urban and of rural settings around Delhi (Lal et al., 1994) indicates that the majority of urban students has some knowledge of HIV I AIDS; however, they also have misconceptions about its modes of transmission. Electronic media such as TV, radio, and movies have a paramount role to play in communicating information about HIV transmission to adolescent students (Poddar et al., 1996; Sharma et al., 1994; Heramani, 1992;). Schools in less developed countries represent one of the few structures where large numbers of students are provided the health education that plays a critical role in the effort to reduce the risk of HIV ISTDs infection (Barthles et al., 1994; Sharma et al., 1994). School-based HIV prevention efforts have been strongly recommended as a major strategy toward
152 increasing adolescents' HIV-related knowledge, promoting preventive behavior (DiClemente, 1991}. A comparative study of awareness and attitudes about HIV I AIDS among students living in India and migrants to the U.S. reveals that 74% of the Indian group and 53% of the U.S. group felt that their knowledge of this disease is not adequate: 90% of Indian group and 79% of U.S. group felt that people in India do not have adequate knowledge about AIDS (Chakraborty et al, 1996). In the U.S., HIV I AIDS prevention among adolescents is a national public health priority. In India, State and local governments funded by UNICEF have started various school-based sex education sponsor programs. However, those programs may not impart the required skills that help students develop safer sex behavior or delay sexual debut. The Health Belief Model (HBM) is a theoretical and conceptual framework, which addresses behavior issues or intention to change behavior. The HBM depends mainly upon two values: (1) the value placed by an individual on a particular goal, and (2) the individual's estimate of the likelihood that a given action will achieve that goal. When these values are conceptualized in the context of health-related behavior, the results are (i) a desire to avoid illness (or if ill, to get well) and (ii) a belief that a specific health action will prevent illness Ganz and Becker, 1984). The model consists of four dimensions: perceived susceptibility, subjective perception of risk relative to health threat; perceived severity, personal evaluation of the probable biochemical and social consequences posed by the health threat which varies from individual to individual; perceived benefit and barriers, assessment of the relative efficacy of, and feeling about difficulties and potential negative consequences of, the proposed action; and cues to action, a trigger that helps the decision-making process. In addition, self-reporting also assesses the perceived severity of the disease. Further, there are some modifying influences: a set of socio-demographic variables or socio-psychological factors related to those dimensions. Yep (1993} indicates that perceived severity and barriers are significant predictors for safer sex behaviors among Asian-American students. METHODS AND DESIGN The study The present study will examine the relationship of knowledge, health beliefs, attitudes, and risk behaviors t~ HIV ISTDs among
153
Indian adolescents, including whether dimensions of HBM are capable of predicting Indian adolescents' behavior. The Indian school system used to be based on the old traditional British system; however, a new system introduced a few years ago is a 10-plus-2 system. Plus 2 are equivalent to the 11th and 12th grades of American schools. There are two types of Indian schools: public schools (funds received from the state government) and private schools (controlled and owned by individuals or religious, philanthropic, or social organizations). Bombay (Mumbai) is the financial capital of India, so there are a large number of private schools. To avoid selection bias, this study covers schools located across Bombay irrespective of their being private or public. There is no information on the population characteristics of the areas in which these schools are located; however, they all cater to an upper middle class population. Students in the Indian equivalent of American 11th and 12th grades were interviewed. The three schools where the study was administered are located in north, central, and south Bombay, a city with a population in excess of 12.5 million. While any student could refuse to fill out the questionnaire and choose to read a schoolbook instead, none chose this option. In total, 1230 usable responses were submitted. Responses from 60 students of the New Bombay school were discarded; the questionnaire had been erroneously administered to students who spoke Marathi by the teacher who verbally translated the questions. All students who answered the questionnaire, with the exception of this group, had had all their education with English as the medium of instruction. In addition, due to missing data there are disparities in total numbers; however, these have been accounted for by explanations within individual tables, as necessary. Data collection tool The data collection instrument was comprised of the CDC questionnaire (The Safer Choices Project: Coyle et al., 1996) extensively used with high school populations in the United States and which has acceptable reliability and validity in that population. It was modified for Indian use by being circulated to a number of educators in Bombay who advised on the changes in colloquial terms to make it more culturally and linguistically appropriate.
154 Study group This is a secondary data analysis of a previously collected data set
of 1230 respondent students. Table 2. illustrates the sodademographic traits that characterize the study participants. The data consists of responses from 711 female and 519 male students. The majority of students (861) were 16 years and younger; 369 were aged 17-20 years. Most of them (921) were in the 11th grade, 303 students were in the 12th grade. Students came from mostly well-educated backgrounds, with a usual education of both mothers and fathers at the college level The majority of them (725) lived in a nuclear family and 256 in a joint/ extended family [data not shown]. Most students reported passing grades for Scholastic Achievement. Most commonly, a mixture of English and the Mother tongue, usually Marathi, was spoken at home.
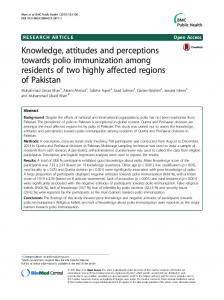
Study variables Figure 1 shows the following variables were obtained for analysis: (1) Sododemographic variables: age, gender, class grade, level of parents' education, languages spoken at home; (2) psychostructural variables as modifying factors: knowledge or awareness about HIV /STDs, prior contact with HIV /STD-infected patients. The role of demographic, soda-psychological and structural characteristics is that they serve to condition both individual perception and perceived benefit of preventive action. Perceived barriers refer to expensive, inconvenient, and unpleasant actions; the variable selected for analysis is: REASONS FOR NOT USING A CONDOM. Perceived susceptibility and seriousness refers to subjective risk of contacting HIV /STD infection, fear of getting HIV /STDs -will you hug and/or help an AIDS/HIV-infected patient. In addition to these dimensions, a factor that served as a cue or trigger to appropriate action was exposure to AIDS or HIV I STD-infected patients. The variables relating to the HBM dimensions of perceived susceptibility, perceived seriousness, cue to action, intention of safer sex were developed as scales by adding together all of the responses which make up each variable respectively.
Statistical analysis As a first step in the analysis, the soda-demographic and predictive variables were summarized and described using tables, correlation, and other descriptive statistics. The outcome intention
155 Analysis Plan based on Health Belief Model Individual Perception
. .
•
•
Likelihood of Action
Modifying Factors
Soclo-Demogrsphlc variables; age, gender, class grade, level of parents' education, language spoken In home, will use variables. Psycho-Structural variables; knowledge about disease, prior contact with HIV/STD patients.
Perceived Susceptibility to HIV/STD; chancas of getting HIV/STD lnlectlon Perceived IBJ'Iousnesal or severity; hug /help AID or HIV patients
•
r+
t ~
•
Cue to Action Exposure to patients
• •
--+
•
Perceived benefH of preventive action Minus Perceived barrier: reason not using condom
•
self -Reporting Likelihood of taking or recommended preventive Intention to safer sex behavior.
Figure 1. The "Health Belief Model" as predictor of preventive intention of safe sex behavior of Indian adolescents.
to safer sex behavior was regressed upon the available demographic, education, and language variables to obtain the best fit to the model. While retaining these variables, the predictor of interest, intention to practice safer sex behaviors, was introduced. This allows assessment of the additional explanatory power of the last variable. Appropriate statistical models were applied to the data to examine the estimated coefficients of the predictors of interest. All tests were carried out at the 0.05 levels, and no adjustment for multiple testing was made. The analyses are described in Tabl~ 1. below: In each model of Table 1 the effect of a study variable may be determined by testing the hypothesis that the estimated regression coefficient is equal to zero.
RESULTS Descriptive Statistics Table 2 previously described, illustrates the socio-demographic traits that characterize the study participants.
Co relational Analysis Pearson correlation between predictors and the HBM dimensions with covariates revealed {Table 3), that the pattern of relationships
156 TABLE 1 Outcome variables, and test for statistical analyses Outcome variables
Study variables
Covariates
Test
Dimensions of HBM: Perceived susceptibility Perceived severity Perceived barriers Cue to action Self-reporting
Intention Multiple Age Sex to change reg. model sex behavior Class outcome. Grade Language used Parent education
Intention to change sex behavior
Knowledge aboutHIV/ STDs
Age Sex Clss Parent education Class grade Language used
Logitmodel for probability of "yes" outcomes
was not very strong with the study variable, intention to safer sex behavior. However, perceived susceptibility had a negative relationship with Gender (P:S;O.Ol) and the Language Spoken at Home (Marathi) (P:S;O.Ol). Perceived severity/seriousness was significantly associated with intention to practice safer sex behaviors (P:S;O.Ol), Language Spoken at Home (P:S;O.Ol), but negatively related to the study years of college and Level of Parent's Education (father-P:S;O.OS, and mother-P:S;O.Ol). Selfreporting was significantly associated with intention to practice safer sex behavior (P