Ultrasound Obstet Gynecol 2007; 29: 368–371 Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.3961
Opinion Levator trauma in labor: a challenge for obstetricians, surgeons and sonologists
Recent advances in pelvic floor assessment have led to the rediscovery of a form of maternal birth trauma that was first described in 19071 but is absent from modern textbooks. Avulsion of the pubovisceral muscle from the pelvic sidewall seems to occur in 15–30% of vaginally parous women. Its prevalence is probably on the rise, as the likelihood of trauma seems to increase with higher maternal age at first delivery. Levator avulsion appears to be a significant part of the missing link between vaginal childbirth and prolapse and is likely to be the root cause of many cases of recurrence after prolapse surgery. At present, no techniques exist for the surgical repair of resulting defects. However, it is fortuitous that, hot on the heels of the rediscovery of levator avulsion and its significance, we seem to have chanced upon a means of dealing with anterior compartment prolapse in the presence of such trauma. Transobturator fixation of anterior compartment mesh, featured in this issue by Ralf Tunn of Berlin2 , appears to cross the hiatus at the site of the defect and to provide support precisely where it is most needed. As shown by Dr Tunn, the meshes used for transobturator repair are identified easily by ultrasound, and imaging has already provided some surprising insights into the nature and mechanism of action of this new surgical technique. Over the last three decades, we have learned a lot about the epidemiological link between vaginal childbirth and pelvic floor dysfunction. Vaginal delivery is associated with a relative risk of 2–3 for fecal incontinence3 , and we think we know how to explain this. Trauma to the pudendal nerve was investigated extensively in the 1980s and 90s4,5 . Obstetric tears of the external and internal anal sphincters are familiar to every resident in obstetrics and gynecology after their first few weeks in training, and there is a lot of ongoing work to optimize detection and postpartum repair6,7 . As regards stress urinary incontinence, the relative risk is about the same3 , despite the fact that we do not really know which structures are responsible. The epidemiological link between childbirth and pelvic organ prolapse is stronger and particularly well established, with a relative risk of between 4 and 108 . Despite all these research data, there really are no prospects yet for preventative intervention. Elective Cesarean section, the one potentially prophylactic intervention, may well be associated with so much shortand longterm morbidity and costs to the taxpayer as to defeat the purpose. This is an unfortunate state of affairs, as demographic change in virtually all societies, especially delayed childbearing and increasing obesity, may well be leading
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd.
to increased pelvic floor morbidity9,10 . The ageing population and altered perceptions of health needs will also impact on the workload of medical and paramedical practitioners dealing with pelvic floor dysfunction. There is an obvious need for research into the mitigation of pelvic floor morbidity, which results in over 200 000 surgical procedures per year in the United States alone3 . It now appears that we may have missed the forest for the trees. We have overlooked a form of maternal birth trauma that occurs commonly during crowning of the fetal head, about once a day in an obstetric unit catering for a few thousand deliveries per year. Occasionally, it can be detected visually if it is combined with a vaginal tear, or, if occult, it can be detected by palpation and imaging (Figure 1). I acknowledge that this seems hard to believe. The problem should have been solved in the late 1900s, rather than being left to us. Why did it take obstetricians so long to detect a problem that must have been there forever – that is, ever since hominids assumed an upright posture and developed this peculiar compromise that is the levator ani muscle complex of Homo sapiens? In fact, delivery-related levator trauma was detected a long time ago. In 1907, Halban and Tandler published a monograph in Vienna1 that is still regarded as the finest achievement in pelvic floor anatomy by many working in this field. In this monograph on pelvic organ prolapse they describe, on Page 191, almost complete loss of the anteromedial aspects of the levator ani muscle in women with prolapse, and they put the blame squarely on childbirth, implying intrapartum trauma. In 1943, Howard Gainey, a general obstetrician from Kansas City, published data on a series of 1000 women who he had examined for pelvic floor trauma after vaginal delivery11 . He confirmed his observation in another paper 12 years later12 . Gainey described an incidence of trauma to the pubococcygeus muscle of approximately 20–30% in primiparous women, with a preponderance of rightsided trauma – exactly as we are observing today with the help of modern imaging methods13 – 16 . Gainey used his fingers – but it is obvious that the digital detection of pelvic floor trauma, while possible, is not easy and requires significant training17,18 . This may be one of the reasons that his publications had little, if any, impact. Another may be that he ended up advocating universal forceps and episiotomy, which is difficult to understand when, on biomechanical grounds, both may be risk factors for levator trauma, rather than being protective; forceps delivery definitely seems to be associated with increased levator trauma10,15 . So Gainey probably drew the wrong conclusions, but his clinical findings are vindicated now, over
OPINION
Opinion
369
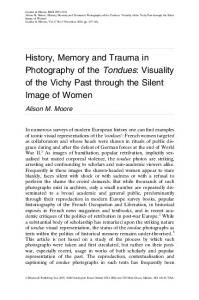
Figure 1 Levator avulsion injury as seen in a labor ward in a patient with a large vaginal tear (a) and on translabial three-dimensional imaging (b, rendered volume, axial plane). The pathognomonic features are a slit-like gap between the vaginal wall and pelvic sidewall (a, arrow), and, on ultrasound, the vagina reaching the pelvic sidewall (b, arrow) with no intervening muscle, unlike the healthy contralateral side.
60 years later, by investigators using three-dimensional (3D) ultrasound and magnetic resonance imgaing (MRI). Vaginal childbirth commonly results in major trauma to the inferomedial aspects of the levator ani muscle. Most commonly this seems to take the shape of ‘levator avulsion’: the muscle is detached from its insertion on the inferior pubic ramus and the arcus tendineus of the levator ani. As to be expected from similar injuries to the bone–muscle interface elsewhere, it is the interface that suffers, not the belly of the muscle, even though remnants of muscle may be found on the line of insertion. The muscle retracts pararectally, just as the external anal sphincter does after a third- or fourth-degree perineal tear. It is astounding that this form of trauma is absent from our obstetric textbooks. Until very recently, the clinical relevance of such trauma was uncertain. Undoubtedly, there are many women who have suffered an avulsion injury without being in any way symptomatic of pelvic floor dysfunction. The latency between the occurrence of trauma and the development of symptoms may be several decades. However, there is sufficient evidence now to state that delivery-related levator trauma is associated with prolapse, especially of the anterior and central compartments10,13,14,16 , with Margulies et al. recently describing an odds ratio of 6.6 for major levator trauma in women with objective prolapse on clinical assessment16 . My own data confirm this, with an odds ratio of 5.7 (95% CI, 3.5–9.1) in a series of 789 women (unpubl. data). Incidentally, the likelihood of trauma in symptomatic prolapse should be higher still, as women with congenitally increased pelvic organ mobility are less likely to perceive symptoms, having lived with, for example, a second-degree cystocele throughout their lives. While levator trauma is clearly not the only etiological factor in the development of pelvic floor dysfunction, it
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd.
seems to play a major role, at least in the pathogenesis of prolapse. As we were using the latest in laboratory technology to investigate collagen metabolism and gene expression, the solution to the problem was right under our noses: in every delivery suite or birthing unit on the planet. One fortunate consequence of this rediscovery is that we may not have to wait for 20 years in order to assess the effect of preventative intervention: levator avulsion probably is a valid intermediate outcome parameter. Since we now have a rough idea as to the nature of the missing link between childbirth and prolapse, we should look into the biomechanical properties of this muscle–bone interface and establish in-vitro models for such trauma. We need to create levator trauma in vitro, define the biomechanical circumstances of ‘catastrophic failure’ of the muscle–bone interface, and look into ways to modify its elastic limit, or to reduce the likelihood of failure by alternative means. It is apparent that the likelihood of trauma varies from one first-time mother to the next; the relationship between maternal age at first delivery and trauma is sufficient prima-facie evidence for this hypothesis (Figure 2). We need to define personal and obstetric risk factors for trauma and to start work on modifying them. Ultimately, one may even consider targeted elective Cesarean section in those women at high risk of trauma. Even more importantly, the recent realization that, in some women, levator trauma is apparent clinically at birth (Figure 1), opens up entirely new possibilities. We need to start identifying levator trauma postpartum, at least in those women in whom vaginal tears have converted an occult avulsion defect into overt trauma. Once identified, it seems ethical to attempt closure of the defect and to follow up the patient, preferably by 3D
Ultrasound Obstet Gynecol 2007; 29: 368–371.
Dietz
370
Defects (%)
50
0
20
30
40
Maternal age at P1 (years)
Figure 2 Relationship between age at first delivery (P1) and the prevalence of levator avulsion injury (n = 478; data from Dietz and Lekskulchai22 ). The regression line and 95% CI are indicated.
pelvic floor ultrasound, as this method is inexpensive and is becoming generally available in obstetric imaging units, or by MRI or at the very least palpation. At last, we have the opportunity to make a real difference: with primary prevention by modifying biomechanics and/or obstetric intervention, with secondary prevention in the sense of postpartum repair, and in the medium term probably even with entirely new forms of surgical treatment of symptomatic prolapse.
It is possible that increasing awareness of the nature and relevance of pelvic floor trauma will have unwanted effects on the Cesarean section rate. However, it is to be hoped that efforts at prediction, prevention and mitigation of permanent trauma will ultimately have the opposite result. Currently, more and more women opt for an elective Cesarean section in order to avoid pelvic floor trauma. Once we understand the etiology and pathophysiology of such trauma better, many of these women will in fact be shown to be at low risk of such trauma. Hopefully, their decisions will become much more informed in the near future, and some may well become more likely to choose vaginal delivery. So, what do we tell women presenting with prolapse on the basis of an avulsion injury, particularly a bilateral one, now – in 2007? Do we just tell them that, unfortunately, something drastic happened when their first child was born, that it can’t be fixed by today’s surgical techniques (as they say in Australia, ‘Tough bikkies mate’) and to come back in another decade or so? By pure chance, and very fortunately from the pelvic reconstructive surgeons’ and their patients’ points of view, a urogynecologist from Townsville, Australia, was developing a new surgical technique precisely while we were convincing ourselves that we had discovered an incurable form of pelvic organ prolapse. In March 2003, he adapted the transobturator
Figure 3 Transobturator mesh repair (PerigeeTM ) in a patient with bilateral levator avulsion 4 years after a rotational forceps delivery (tomographic ultrasound in the axial plane, with slices from 5 mm below to 12.5 mm above the plane of minimal hiatal dimensions). The mesh traverses the hiatus at the site of injury (asterisks).
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd.
Ultrasound Obstet Gynecol 2007; 29: 368–371.
Opinion
371
sling of Delorme et al.19 , which was itself a derivate of the tension-free vaginal tape (TVT) of Ulmsten et al.20 , in order to anchor an anterior compartment mesh patch with a total of four anchoring tapes placed via the transobturator route. The idea was taken up by several medical supply companies, without him profiting financially to any significant degree, and now his invention TM has been popularized all over the world as the Perigee TM and Anterior Prolift devices. We have been following Ajay Rane’s patients in a surgical audit21 and intend to continue doing so for several years. Others have been similarly interested in the new technique. In this issue, Tunn and colleagues report on sonographic appearances after transobturator mesh repair2 , showing that both Anterior Prolift and Perigee are easily visible on ultrasound and clearly cover a much smaller area in the anteroposterior direction than anticipated. This is an important finding, which agrees fully with our own observations. It seems that frequently we are using too much mesh (which then folds and overlaps), rather than too little. Regardless, transobturator mesh seems to be effective in correcting anterior vaginal wall prolapse. While Tunn does not report axial plane imaging data, our own data demonstrate that this effectiveness does extend to women with levator avulsion. In fact, the mesh traverses the hiatus precisely at the locus of injury (Figure 3): it seems we may have found a partial or indirect ‘cure’ for what was thought ‘incurable’. The technique is not always successful, as shown by instances of pull-through of the superior anchoring arms21 , but, on anatomical grounds, transobturator mesh anchoring is highly likely to be more successful than is conventional anterior repair in women with major levator trauma. The use of mesh in pelvic reconstructive surgery is not without problems, so much so that many surgeons reject its use altogether. Mesh erosion, infection, pain syndromes and dyspareunia are all potentially more common compared with after native tissue repair. However, clearly some women are at high risk of recurrence, and we are now learning how to identify them. Without doubt, ultrasound imaging will be very useful in this regard, allowing us to determine who will require mesh techniques in order to reduce the risk of recurrence. At the same time, ultrasound will help us to optimize surgical techniques and devices, while we are learning how to predict, prevent and surgically treat the underlying trauma itself. We are entering an entirely new phase in pelvic floor medicine, characterized by rapid progress that has become possible largely due to modern imaging. H. P. Dietz Western Clinical School, Nepean Campus, University of Sydney, Nepean Hospital, Penrith, NSW 2750, Australia (e-mail:
[email protected])
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd.
REFERENCES 1. Halban J, Tandler J. Anatomie und Aetiologie der Genitalprolapse beim Weibe. Braumueller: Vienna, 1907. 2. Tunn R, Picot A, Marschke J, Gauruder-Burmester A. Sonomorphological evaluation of polypropylene mesh implants after vaginal mesh repair in women with cystocele or rectocele. Ultrasound Obstet Gynecol 2007; 29: 449–452. 3. Patel D, Xu X, Thomason AD, Ransom SB, Ivy JS, DeLancey JO. Childbirth and pelvic floor dysfunction: an epidemiologic approach to the assessment of prevention opportunities at delivery. Am J Obstet Gynecol 2006; 195: 23–28. 4. Smith AR, Hosker GL, Warrell DW. The role of pudendal nerve damage in the aetiology of genuine stress incontinence in women. Br J Obstet Gynaecol 1989; 96: 29–32. 5. Allen RE, Hosker GL, Smith AR, Warrell DW. Pelvic floor damage and childbirth: a neurophysiological study. Br J Obstet Gynaecol 1990; 97: 770–779. 6. Sultan AH, Thakar R. Lower genital tract and anal sphincter trauma. [Review] Best Pract Res Clin Obstet Gynaecol 2002; 16: 99–115. 7. Andrews A, Sultan AH, Thakar R, Jones PW. Occult anal sphincter injuries – myth or reality? BJOG 2006; 113: 195–200. 8. DeLancey J. The hidden epidemic of pelvic floor dysfunction: achievable goals for improved prevention and treatment. Am J Obstet Gynecol 2005; 192: 1488–1495. 9. Rortveit G, Hunskaar S. The association between the age at the first and last delivery and urinary incontinence. Neurourol Urodyn 2004; 23: 562–563. 10. Dietz HP, Lanzarone V. Levator trauma after vaginal delivery. Obstet Gynecol 2005; 106: 707–712. 11. Gainey HL. Post-partum observation of pelvic tissue damage. Am J Obstet Gynecol 1943; 46: 457–466. 12. Gainey HL. Postpartum observation of pelvic tissue damage: Further studies. Am J Obstet Gynecol 1955; 70: 800–807. 13. Dietz H, Steensma A. The prevalence of major abnormalities of the levator ani in urogynaecological patients. BJOG 2006; 113: 225–230. 14. Dietz HP. Quantification of major morphological abnormalities of the levator ani. Ultrasound Obstet Gynecol 2007; 29: 329–334. 15. Kearney R, Miller JM, Ashton-Miller JA, DeLancey JO. Obstetric factors associated with levator ani muscle injury after vaginal birth. Obstet Gynecol 2006; 107: 144–149. 16. Margulies R, Huebner M, DeLancey J. Levator ani muscle defects: what origins and insertion points are affected? Int Urogynecol J 2006; 17 (S2): S118–S119. 17. Kearney R, Miller JM, DeLancey JO. Interrater reliability and physical examination of the pubovisceral portion of the levator ani muscle, validity comparisons using MR imaging. Neurourol Urodyn 2006; 25: 50–54. 18. Dietz HP, Hyland G, Hay-Smith J. The assessment of levator trauma: A comparison between palpation and 4D pelvic floor ultrasound. Neurourol Urodyn 2006; 25: 424–427. 19. Delorme E, Droupy S, de Tayrac R, Delmas V. Transobturator tape (Uratape): a new minimally-invasive procedure to treat female urinary incontinence. Eur Urol 2004; 45: 203–207. 20. Ulmsten U, Ulmsten U, Henriksson L, Johnson P, Varhos G. An ambulatory surgical procedure under local anesthesia for treatment of female urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct 1996; 7: 81–5; Discussion 85–86. 21. Shek K, Dietz H, Rane A. Transobturator mesh anchoring for the repair of large recurrent cystocele. ICS Annual Scientific Meeting, 2006; Christchurch, New Zealand. 22. Dietz H, Lekskulchai O. Older age at first delivery is associated with major levator trauma. Int Urogynecol J 2006; 17 (S2): S148.
Ultrasound Obstet Gynecol 2007; 29: 368–371.