CLINICAL RESEARCH
www.jasn.org
Molecular Phenotypes of Acute Kidney Injury in Kidney Transplants Konrad S. Famulski,*† Declan G. de Freitas,†‡ Chatchai Kreepala,† Jessica Chang,† Joana Sellares,† Banu Sis,*† Gunilla Einecke,§ Michael Mengel,*† Jeff Reeve,*† and Philip F. Halloran†| Departments of *Laboratory Medicine and Pathology and |Medicine, University of Alberta, Edmonton, Alberta, Canada; †Alberta Transplant Applied Genomic Centre, Edmonton, Alberta, Canada; ‡Manchester Royal Infirmary, Manchester, United Kingdom; and §Hannover Medical School, Hannover, Germany
ABSTRACT Little is known regarding the molecular phenotype of kidneys with AKI because biopsies are performed infrequently. However, all kidney transplants experience acute injury, making early kidney transplants an excellent model of acute injury, provided the absence of rejection, because donor kidneys should not have CKD, post-transplant biopsies occur relatively frequently, and follow-up is excellent typically. Here, we used histopathology and microarrays to compare indication biopsies from 26 transplants with acute injury with 11 pristine protocol biopsies of stable transplants. Kidneys with acute injury showed increased expression of 394 transcripts associated with the repair response to injury, including many epithelium-like injury molecules tissue, remodeling molecules, and inflammation molecules. Many other genes also predicted the phenotype, including the acute injury biomarkers HAVCR1 and IL18. Pathway analysis of the injury-repair transcripts revealed similarities to cancer, development, and cell movement. The injury-repair transcript score in kidneys with acute injury correlated with reduced graft function, future renal recovery, brain death, and need for dialysis, but not with future graft loss. In contrast, histologic features of acute tubular injury did not correlate with function or with the molecular changes. Thus, the transcripts associated with repair of injury suggest a massive coordinated response of the kidney parenchyma to acute injury, providing both an objective measure for assessing the severity of injury in kidney biopsies and validation for many biomarkers of AKI. J Am Soc Nephrol 23: 948–958, 2012. doi: 10.1681/ASN.2011090887
Although AKI is an important problem,1–3 native kidneys with AKI are rarely biopsied, limiting studies of AKI biomarkers to urine and body fluids.4 However, kidney transplants offer a unique opportunity to study the injury-repair response to AKI because all transplants experience AKI, CKD is excluded, and numerous indication biopsies are performed to exclude rejection, guided by the international Banff histopathology consensus system. Moreover, transplants have detailed function assessments and are followed indefinitely. AKI induced by transplantation can be modeled in rodent kidney isografts,5–7 as recently reviewed.8 The mouse studies showed that some transcript changes in transplants reflect AKI, but other transcripts reflect the acute phase response to the surgical procedure.5 The picture is further complicated in aging kidneys.9,10 948
ISSN : 1046-6673/2305-948
This prospective study of kidney transplants with AKI was undertaken to define the transcripts induced by human AKI and their clinical correlations. We previously analyzed the correlates of estimated GFR (eGFR) in transplant biopsies, but those were mainly
Received September 2, 2011. Accepted January 10, 2012. Published online ahead of print. Publication date available at www.jasn.org. Present address: Joana Sellares, Hospital de la Vall d' Hebron, Barcelona, Spain. Correspondence: Dr. Philip F. Halloran, Alberta Transplant Applied Genomics Centre, University of Alberta, 250 Heritage Medical Research Centre, Edmonton, Alberta T6G 2S2. Email:
[email protected] Copyright © 2012 by the American Society of Nephrology
J Am Soc Nephrol 23: 948–958, 2012
www.jasn.org
late biopsies with atrophy-fibrosis, not AKI.11 We hypothesized that indication biopsies from early kidney transplants, selected to exclude kidneys with rejection and diseases, will reveal the molecular features of AKI. Our strategy was to neutralize the ubiquitous minor changes inevitably induced by the transplant process by comparing AKI kidneys to histologically pristine protocol biopsies of stable transplants. This study aimed to elucidate the molecular changes that reflect clinically significant functional disturbance and their relationship with histopathology changes and prognosis.
RESULTS Selection of Biopsies from Kidney Transplants with Pure AKI
We identified AKI kidneys from a prospective study of 234 kidney transplant biopsies for clinical indications from 173 consenting patients. We excluded kidneys with rejection and kidney disease by histologic criteria, and also excluded those with nondiagnostic suspicious histologic lesions. This identified a “pure AKI” cohort of 28 biopsies from 26 patients, with mean eGFR at biopsy of 26 ml/min (range, 8–52) (Table 1). Of 28 biopsies, 21 displayed features that pathologists believe reflect acute tubular injury.12,13 Fifteen were from deceased donor kidneys, of which eight manifested delayed graft function (DGF) (i.e., initial dialysis dependency). The median follow-up after biopsy was 3.9 years. The extent of histologic tubule injury changes can be assessed for its correlation with molecular changes and function because these kidneys were not chosen on the basis of histologic criteria for tubular injury; rather, they were chosed only by time post-transplant and exclusion of diseases. During follow-up, only one kidney from the AKI cohort progressed to end stage kidney failure at 30 months, attributed to antibody-mediated rejection (ABMR) caused by nonadherence, and one patient died with a functioning graft. A validation set was generated to test the molecular features (Table 1). The results below refer exclusively to the original AKI cohort, and the validation set is analyzed at the end of the Results section. Selection of Controls
Our strategy was to distinguish clinically significant AKI from the minor injury that accompanies every transplant. Thus, controls consisted of protocol kidney transplant biopsies selected from a previously published cohort14 with clinically appropriate stable function at 6 weeks post-transplant, with no indications for biopsy. After excluding biopsies with any histologic abnormalities, including acute tubular injury changes (Table 1), we were left with a set of 11 pristine protocol biopsies similar in age to the AKI kidneys, including both living and deceased donor kidneys. Histopathology, Function, and Survival of Kidneys with AKI
Histology scores for inflammation (i-Banff, i-total) and atrophy fibrosis (ci, ct) were compared for biopsies from the J Am Soc Nephrol 23: 948–958, 2012
CLINICAL RESEARCH
AKI cohort versus those with T cell–mediated rejection (TCMR), borderline rejection, other diseases and pristine protocol biopsies (Table 2). Because of the selection criteria, the pure AKI biopsies and pristine protocol biopsies had little inflammation or atrophy fibrosis, and the pristine protocol biopsies had no acute tubular injury features. Three of 35 grafts with TCMR failed, but all had later biopsies showing ABMR or mixed rejection. The 34 other kidney failures after indication biopsies reflected diseases that emerged late after transplantation such as ABMR or recurrent GN.15,16 The mean eGFR at the time of biopsy was low in the AKI cohort (mean 26) and in TCMR and borderline rejection biopsies, compared with other indication biopsies (Table 2). However, by 6 months after biopsy, these kidneys showed the most improvement (DeGFR). As expected, the pristine protocol biopsy cohort had higher mean eGFR at the time of biopsy than the AKI cohort, and showed little improvement over time. Kidneys with pure AKI in the early post-transplant period manifest impaired function at biopsy but good recovery and prognosis, and are suitable for defining the injury-repair response to clinically significant AKI. Defining the Injury-Repair Response Associated Transcripts in the Pure AKI Biopsies
We compared microarray results from AKI biopsies versus pristine protocol biopsies to define the features of clinically significant injury. This comparison identified 946 probe sets, including 394 nonredundant genes whose expression was increased at least $1.5-fold higher in AKI than in pristine protocol biopsies (Supplemental Table 1), at the false discovery rate (FDR) of 0.05. We named these injury-repair response– associated transcripts (IRRATs). For detailed study, we selected from the 394 IRRATs the 30 with the highest fold increase compared with the pristine protocol biopsies (Table 3). The expression of the individual top 30 IRRATs in AKI biopsies was 2.7- to 7.9-fold higher than in pristine protocol biopsies. Four of the top 30 IRRATs (LCN2, AKAP12, FOS, and EGR1) had previously been identified as biomarkers of AKI, on the basis of detection of the product in urine or blood,17–19 or mRNA expression in human kidney.20,21 The complete set of 394 IRRATs included four other known AKI biomarkers (CLU, CXCL1, CYR61, and THSB1) but did not include some known biomarkers such as HAVCR1 and IL18. Although the IRRATs were defined without reference to GFR measurements, they correlated strongly with eGFR. Thus, expression of 26 of the top 30 individual IRRATs correlated with reduced eGFR at biopsy, and 24 of 30 also correlated with eGFR recovery 6 months after biopsy (Table 3). After excluding the top 30 IRRATs, there were 138 additional IRRATs whose expression correlated with eGFR, with correlation coefficients ranging from 20.82 to 20.50 (Table 4). Mouse orthologs of the 394 IRRATs had extensive overlap with transcripts previously shown to be increased in mouse AKI, Acute Kidney Injury in Transplants
949
CLINICAL RESEARCH
www.jasn.org
Table 1. Demographics of patients selected for early AKI from biopsies for clinical indications and stable early transplants selected from protocol biopsies
Demographics
Pure AKI Cohort
Patient characteristics at diagnosis number of patients 26 mean recipient age (yr) 52 (16–75) primary disease GN 9 (32) diabetic nephropathy 4 (14) others 9 (32) unknown etiology 6 (21) mean donor age (yr) 50 (22–69) mean donor age (living donor) 46 (37–56) mean donor age (deceased donor) 53 (22–69) donor type deceased/living (% deceased 15/ 11 (57.6) donor transplants) delayed graft function rate 8/26(31) median time from transplant to biopsy (d) 16 (6–42) median duration follow-up postbiopsy (d) 1414 (98–2155) allograft failure 2/26 (7.7)a Clinical characteristics at time of biopsy number of biopsies 28 indication for biopsy as indicated by clinician concerns about renal function 20 (71) other or unknown 8 (29) histologic diagnosis acute tubular injury ($5% acute tubular 21 (75) injury score) no major abnormalities 7 (25) mean eGFRd at the time of biopsy 26 (8–52) immunosuppressive drug regimen MMF, tacrolimus, steroids 11 (39.3) MMF, tacrolimus 8 (28.6) MMF, cyclosporine, steroids 3 (10.7) other 6 (21.4)
P Value (Pure AKI versus Pristine Protocol Biopsies)
P Value (Validation Set versus Pristine Protocol Biopsies)
27 49 (21–68)
.0.05
.0.05
3 (11) 10 (37) 14 (52) 13 (48) 43 (16–59) 44 (16–59) 42 (26–56) 8/19 (30)
.0.05 .0.05 .0.05 .0.05 .0.05 .0.05 .0.05 .0.05
.0.05 .0.05 .0.05 .0.05 .0.05 .0.05 .0.05 0.004
2/11 (18) 42 2000 (732–2932) 1/11 (9.1)b
5/27 (19) 24 (7–42) 727 (1–2146) 2/27 (7.4)c
.0.05 ,0.001 0.006 .0.05
.0.05 ,0.001 ,0.001 .0.05
11
28
Pristine Protocol Biopsy Cohort
Validation Set
11 49 (29–70) 2 (18.2) 1 (9.1) 4 (36.4) 4 (36.4) 53 (20–82) 44 (35–52) 55 (20–82) 9/2 (81.8)
(protocol) (protocol)
25 (89) 3 (11)
0 (0)
18 (64)
,0.001
,0.001
10 (36) 31 (10–46)
,0.001 ,0.001
,0.001 ,0.001
0.017 .0.05 ,0.001 .0.05
.0.05 .0.05 0.010 .0.05
11 (100) 49 (23–89) 0 (0) 0 (0) 8 (72.7) 3 (27.3)
5 (18) 7 (25) 7 (25) 9 (32)
Data are shown as n (%) or median (range) unless otherwise indicated. MMF, mycophenolate mofetil. a The cause of failure: death with functioning graft, and ABMR in a nonadherent patient 30 months post-transplant. b The cause of failure: death with functioning graft. c The cause of failure: death with functioning graft, and membranoproliferative GN at 60 months post-transplant. d eGFR obtained using the four-variable MDRD formula (in milliliters per minute per 1.73 m2).
either isografts (n=124, P,0.001) or native kidneys with ischemic ATN (n=254, P,0.0001).5 Of 18 mouse orthologs of the top 30 human IRRATs, 17 were increased in mouse AKI models5 (Table 5). Six of those belonged to the previously published injury-repair induced sets IRIT(I) and IRIT(L).5 Thus, IRRAT changes in AKI are largely conserved between human and mouse. Relationship of the IRRAT Score to Histology and Function in Injured Transplants
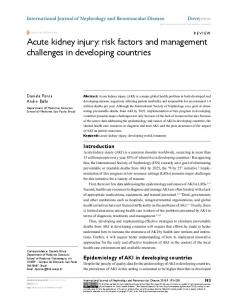
The 28 AKI biopsies were arranged by increasing IRRAT score (geometric mean of the fold increase in the top 30 IRRATs versus control nephrectomies) to compare the IRRAT scores with DGF, eGFR, and histopathology features of acute tubular injury (Figure 1). We discretized the IRRAT scores into tertiles 950
Journal of the American Society of Nephrology
(see top of Figure 1). Nine of 10 kidneys with DGF had IRRAT scores in the top tertile (P,0.05). The top tertile also contained nine biopsies from deceased donors (P,0.05). Kidneys from deceased donors had higher IRRAT scores than kidneys from living donors (3.0 versus 1.6, P,0.05). Whereas high IRRATscores were associated with low eGFR, acute tubular injury features were not; they were present in 6 of 9 in the lowest tertile, 6 of 9 in the middle tertile, and 9 of 10 in the upper tertile (not significant). Histologic features of acute tubular injury were also not associated with DGF or donor type. However, inflammation in AKI biopsies, albeit mild by definition, was nevertheless highest in the top tertile: the mean inflammation scores (i-total) were 2% for the lowest tertile, 5% for the middle tertile, and 13% for the top tertile (P,0.05). J Am Soc Nephrol 23: 948–958, 2012
www.jasn.org
CLINICAL RESEARCH
Table 2. Histology and kidney function in 28 AKI kidney biopsies compared with 206 other transplant biopsies for clinical indications Feature
Pure AKI (n=28)
TCMR (n=35)
Borderline (n=23)
Remaining Biopsies (n=148)a
Pristine Protocol Biopsies (n=11)
4 7 7 6 1
26b 45b 24c 23b 3
8.9 28b 27b 26b 1
7.9 23b 22b 22b 34
3.9 3.9 0b 0.5c 0
4.2
3.8
6.3
Histologic lesions (continuous scores, % of cortex) inflammation (i-Banff) inflammation (i-total) scarring (ci) atrophy (ct) Grafts failed during follow-up (excluding death with function)d Median follow-up time after first biopsy (yr) Renal function (eGFR, ml/min) eGFR at biopsy eGFR at 6 mo DeGFR by 6 mo
3.9
26 51e 25
4.0
33 42e 9f
34 40 5b
35c 38c 2b
49c 55 6b
AKI biopsies were compared with the remaining biopsy groups. Kruskal–Wallis test with Dunn’s correction for multiple comparisons. a Remaining biopsies included diagnoses of ABMR, mixed ABMR/TCMR, GN, polyoma virus, and other nonrejecting biopsies. b P,0.001. c P,0.01. d Failed grafts are represented by one biopsy per patient. e Indicates significant difference between eGFR at biopsy and 6-month eGFR, by the paired t test. f P,0.05.
The IRRAT score in the AKI biopsies anticorrelated with the eGFR at biopsy (20.77, P,0.001) and correlated with the increase in eGFR by 6 months (0.62, P,0.001). The acute tubular injury score by histology did not correlate with eGFR or the increase in GFR (Figure 2). In AKI kidneys, the IRRAT score is associated with DGF, brain death, impairment in eGFR, future recovery of function, and interstitial inflammation. The histologic features that pathologists believe represent acute tubular injury were not related to DGF, deceased donation, eGFR, recovery of function, or IRRAT scores. Cellular Expression and Functional Annotation of IRRATs
Functional annotation of the top 30 IRRATs using Ingenuity Pathway Analysis (Table 6) indicated that the pathways overrepresented included cancer; cellular movement, including migration of tumor cells; tissue development, including cell adhesion; and acute phase response. The complete list of 394 nonredundant IRRATs yielded similar results. Most IRRATs are expressed in parenchymal cells of kidney or in a broad expression in many cells, making kidney parenchymal expression likely. Relatively few were expressed in inflammatory cells. Many Other Transcripts Correlate with IRRATs and Predict AKI
Using our statistical filtering rules, some reported biomarkers of AKI were not found in the top 30 or the complete 394 IRRAT lists, including HAVCR1 (KIM1), IL18, UMOD, CTS3, or FABP1. HAVCR1 did not meet the fold cutoff criteria, and IL18 did not pass the statistical filter. Nevertheless, HAVCR1 and IL18 expression correlated with the IRRAT score in the AKI biopsies J Am Soc Nephrol 23: 948–958, 2012
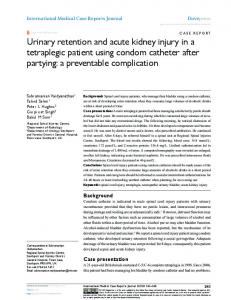
(r=0.9 and r=0.7, P,0.0001, respectively). UMOD, CTS3, and FABP1 had no positive correlation with the IRRAT score. We re-examined all probe sets passing the interquartile range filter (n=12,552) to identify transcripts missed by the initial filtering rules, comparing the binary phenotype of AKI versus pristine protocol biopsies. Our goal was to identify all transcripts that differ between these phenotypes by their P value and by their ability to predict these phenotypes. In Figure 3, the x-axis gives the uncorrected P values for the comparison of phenotypes, whereas the y-axis gives the area under the curve for prediction (AUC). The transcripts positively associated with the phenotype have an AUC .0.5. If negatively associated, the AUC is ,0.5. An AUC at or near 0.5 signifies no discriminatory power. Apart from the top 30 IRRATs (shown as yellow dots), other redundant transcripts (n=1424) had high predictive values for the AKI (AUC $0.7). HAVCR1 and IL18 (pink dots) now showed correlations similar to many top 30 IRRATs. After adjustment for the FDR, 930 transcripts remained, including all IRRATs. Another 1785 transcripts (after the FDR adjustment) were highly negatively associated with the AKI phenotype (AUC #0.3). As an additional control, we examined these relationships after random shuffling of the phenotype labels of AKI and protocol biopsies. No transcript was significant at FDR=0.05 when the labels were randomly shuffled. Relationship between IRRATs, Histology, and Function in the Validation Set
For validation of the molecular studies, we identified a second, independent set of kidneys with AKI, selected only as being the next consecutive kidney biopsies meeting the same criteria in this ongoing study (Table 1). The validation set of 27 kidneys Acute Kidney Injury in Transplants
951
CLINICAL RESEARCH
www.jasn.org
Table 3. Top 30 IRRATs ordered by fold change in AKI biopsies versus pristine protocol biopsies Gene Symbol
Gene Name
Integrin b6 Serine (or cysteine) proteinase inhibitor, clade A NADH dehydrogenase, subunit 6 (complex I) Olfactomedin 4 Pentaxin-related gene, rapidly induced by IL-1b lipocalin 2 (oncogene 24p3) chondroitin sulfate proteoglycan 2 (versican) Lactotransferrin Secretory leukocyte protease inhibitor (antileukoproteinase) ADAMTS1 A disintegrin-like and metalloprotease (reprolysin type) with thrombospondin type 1 motif, 1 MEGF11 Multiple EGF-like domains CDH6 cadherin 6, type 2, K-cadherin (fetal kidney) PI15 Peptidase inhibitor 15 FCGR3A Fc fragment of IgG, low affinity IIIa, receptor for (CD16) NNMT Nicotinamide N-methyltransferase S100A8 S100 calcium binding protein A8 (calgranulin A) SOD2 SOD2, mitochondrial ITGB3 Integrin b3 (platelet glycoprotein IIIa, antigen CD61) NFKBIZ NF of k light polypeptide gene enhancer in B cells inhibitor, z AKAP12a A kinase (PRKA) anchor protein (gravin) 12 VMP1 Likely ortholog of rat vacuole membrane protein 1 ADAM9 A disintegrin and metalloproteinase domain 9 (meltrin g) PTPRC Protein tyrosine phosphatase, receptor type, C FOSa V-fos FBJ murine osteosarcoma viral oncogene homolog OSMR Oncostatin M receptor C9orf71 Chromosome 9 open reading frame 71 EGR1a Early growth response 1 CTSS Cathepsin S RARRES1 Retinoic acid receptor responder (tazarotene induced) 1 VI2A Ecotropic viral integration site 2A ITGB6 SERPINA3 MTND6 OLFM4 PTX3 LCN2a VCAN LTF SLPI
Correlation Raw Signal Correlation Fold Change P in Protocol with eGFR at with DGFR at AKI versus Value Biopsy in AKI 6 Mo in AKI Biopsies Protocol Biopsies 7.9 6.1 5.6 5.5 5.3 4.3 4.1 4.1 4.1
0.001 0.001 0.003 0.001 0.002 0.004 0.004 0.032 0.013
72 252 67 53 15 89 47 441 334
20.69 20.71 20.51 20.74 20.58 20.57 20.35b 20.63 20.70
0.54 0.47 0.43 0.46 0.52 0.50 0.38 0.54 0.52
4.0
0.000
110
20.64
0.52
3.8 3.7 3.6 3.4 3.3 3.2 3.2 3.0 3.0
0.001 0.000 0.008 0.002 0.005 0.004 0.001 0.006 0.004
12 105 17 41 155 175 264 45 141
20.68 20.72 20.40 20.30b 20.56 20.11b 20.61 20.74 20.67
0.59 0.56 0.23b 0.30b 0.52 0.07b 0.57 0.71 0.59
3.0 2.9 2.9 2.9 2.9 2.8 2.8 2.8 2.7 2.7 2.7
0.007 0.003 0.009 0.002 0.000 0.001 0.005 0.009 0.021 0.025 0.008
57 375 103 56 29 65 283 184 190 76 59
20.60 20.71 20.57 20.53 20.48 20.80 20.41 20.48 20.50 20.55 20.32b
0.32b 0.59 0.41 0.37b 0.49 0.73 0.38 0.56 0.43 0.54 0.25b
Nonredundant and annotated genes are shown. In case of multiple transcripts per gene, the one with highest fold change was selected. Spearman correlations of gene expression with eGFR at the time of biopsy and with change in eGFR (DeGFR) at 6 months were considered significant at P,0.05. a Prototypical markers of kidney injury. b P value not significant (P.0.05).
were similar to the original set, differing only in longer median time to biopsy (24 versus 16 days), fewer deceased donors (30% versus 58%), and fewer grafts with DGF (19% versus 31%). Because of these differences, the eGFR was higher in the validation set (31 versus 26 ml/min), reflecting the fact that the extent of AKI was less than in the original AKI set. In the validation set, only one graft was lost, due to membranoproliferative GN, 60 months after the transplant, and one patient died with a functioning graft. The correlation of the top 30 IRRAT score in the validation set with the eGFR at biopsy was 20.62 (P,0.001) and with the increase in eGFR by 6 months was 0.45 (P,0.05). The recovery of eGFR was highest in kidneys with high IRRAT scores (Table 7). The acute tubular injury features did not correlate with IRRAT scores. Inflammation was again highest in the top tertile by the IRRAT score. Thus, the relationships among 952
Journal of the American Society of Nephrology
kidney function, histology, and IRRAT score expression were confirmed in the validation set biopsies. The IRRAT score was higher in the original set than in the validation set (2.5 versus 1.6, P=0.02), because the kidneys from the validation set were less injured (i.e., had better eGFR and less DGF). Analysis of gene expression revealed that 19 of the top 30 IRRATs and 212 of the 394 IRRATs were significantly increased (FDR=0.05) in the validation set (Supplemental Table 1).
DISCUSSION
Although all kidney transplants experience AKI, some are more injured and require an indication biopsy. When rejection and diseases are excluded, such kidneys constitute a pure AKI J Am Soc Nephrol 23: 948–958, 2012
www.jasn.org
CLINICAL RESEARCH
Table 4. Examples of other IRRATs anticorrelating with eGFR at the time of biopsy in AKI biopsies
overlapped the transcripts previously identified in injured mouse kidneys, as well as many biomarkers previously described in Correlation Gene Symbol Gene Title body fluids. Thus, the results present a comwith eGFR prehensive picture of molecular events in TRIM38 Tripartite motif-containing 38 20.82 clinically significant human transplant AKI CLDN1 Claudin 1 20.78 CDC42SE2 CDC42 small effector 2 20.75 that will be useful in supporting diagnostic ICAM1 Intercellular adhesion molecule 1 20.73 applications. IFITM2 IFN induced transmembrane protein 2 (1-8D) 20.73 The elucidation of the transcripts exC2CD4A C2 calcium-dependent domain containing 4A 20.73 pressed in human transplant kidneys with KPNA2 Karyopherin a2 (RAG cohort 1, importin a1) 20.72 AKI offers new support to and understandCASP1 Caspase 1, apoptosis-related cysteine 20.72 ing of developing biomarkers, refining their peptidase (IL-1, b, convertase) interpretation, and establishing how exRASD1 RAS, dexamethasone-induced 1 20.71 pression of AKI biomarkers in body fluids UGCG UDP-glucose ceramide 20.71 correlates with expression in kidney tissue. glucosyltransferase Some biomarkers are more sensitive to TGM2 Transglutaminase 2 (C polypeptide, protein20.71 minor injury or more persistent after injury glutamine-g-glutamyltransferase) CLIC1 Chloride intracellular channel 1 20.70 resolves, whereas others may be more quanTFPI Tissue factor pathway inhibitor (lipoprotein20.70 titative at distinguishing current functional associated coagulation inhibitor) impairment.22,23 For example, increased CASP8 Caspase 8, apoptosis-related cysteine peptidase 20.69 expression of HAVCR1 is reported in priSERPINA1 Serpin peptidase inhibitor, clade A (a-1 20.69 mary diseases24 and in the zero-hour transantiproteinase, antitrypsin), member 1 plant biopsies.25 However, in one study, KLF6 Kruppel-like factor 6 20.69 HAVCR1 lacked the ability to distinguish AMACR/// a-methylacyl-CoA racemase///C1q and 20.68 major from minor injury states in kidney C1QTNF3 TNF-related protein 3 transplants.26 Moreover, the expression of TNIK TRAF2 and NCK interacting kinase 20.68 biomarkers such as HAVCR1 and IL18 in HN1 Hematologic and neurologic expressed 1 20.67 body fluids may also be a sign of systemic MT1M Metallothionein 1M 20.67 PTP4A1 Protein tyrosine phosphatase type IVA, member 1 20.67 trauma.10,27–29 The fact that two AKI, bioNFKBIZ NF of k light polypeptide gene enhancer 20.67 markers HAVCR1 (KIM1) or IL18 were not in B cells inhibitor, z identified as IRRATs by our initial statistical SEC23IP SEC23 interacting protein 20.67 filtering strategy (fold change and FDR) yet GBP2 Guanylate binding protein 2, IFN-inducible 20.67 were nevertheless associated with AKI pheMCL1 Myeloid cell leukemia sequence 1 (BCL2-related) 20.66 notype, when re-analyzed, illustrates a caMET Met proto-oncogene (hepatocyte growth 20.66 veat about reaching negative conclusions in factor receptor) microarray data. Arbitrary selection criteria ABCC4 ATP-binding cassette, subfamily C 20.66 may miss important associations when (CFTR/MRP), member 4 many features are highly correlated, and a SFN Stratifin 20.66 comprehensive examination of the phenoSOCS3 Suppressor of cytokine signaling 3 20.66 CPD Carboxypeptidase D 20.66 type associations of all transcripts should be Genes previously identified as top 30 IRRATs by the fold change in AKI biopsies versus pristine PBx included. were excluded because their correlations with eGFR are shown in Table 3. Although IRRAT expression accurately reflected the functional disturbance in transplants with AKI, the histologic features believed to reflect cohort with varying degrees of functional impairment. We acute tubular injury did not. Various focal features of acute compared this cohort to pristine protocol biopsies of similar ages, thus neutralizing the mild injury present even in well tubular necrosis in humans have previously been reported in native kidney AKI,30 the ability of these features to predict functioning transplants and identifying the IRRATs as the signal evoked in human kidneys by recent major parenchymal current GFR impairment or future functional recovery has injury. In the AKI cohort, the IRRATs correlated with a history been poor, indicating that focal abnormalities are not quantitaof DGF and with deceased donors, depression of eGFR at time tively related to overall parenchymal function. The emergence of of biopsy, future eGFR recovery, and interstitial inflammation. the IRRATs as a reliable measurement of AKI in human biopsies Histologic features considered typical of acute tubular injury can be used in place of histopathology, but can also be used to did not correlate with these measurements or with the IRRATs. guide the identification of new histologic features. For examAn independent validation set confirmed all of the major relaple, we recently showed using confocal microscopy that kidney tionships, as well as IRRAT expression. The IRRATs extensively transplants with AKI undetected by conventional features J Am Soc Nephrol 23: 948–958, 2012
Acute Kidney Injury in Transplants
953
CLINICAL RESEARCH
www.jasn.org
Table 5. All 18 identified mouse orthologs of the top 30 IRRATs show elevated expression in mouse AKI models (isografts and/or ATN) Gene Symbol
Isografts and ATN
Adamts1 Akap12 Ctss Egr1 Evi2a Itgb3 Fos Fcgr4 Olfm4 Ltf Lcn2 Nnmt Osmr Ptprc S100a8 Serpina3n Sod2 Vcan Havcr1a Il18a
Yes Yes Yes Yes Yes
Isografts Only
ATN Only
IRIT (I)
IRIT (L)
Yes Yes Yes
Yes Yes Yes Yes Yes
Yes
Yes Yes Yes Yes Yes Yes
Yes
Yes Yes
Yes Yes
Yes No
No
a
AKI biomarkers that are absent in the human IRRAT set.
Figure 1. Relationship between IRRAT scores, histopathology, delayed graft function, and eGFR at the time of biopsy for clinical indication in kidneys with AKI. Biopsies (open circles) are ordered by the IRRAT score, and the graph illustrates the relationship of IRRAT scores to the histologic assessment of tubular injury (filled circles), delayed graft function (*), and eGFR (triangles).
have a profound diffuse loss of solute carriers in the brush border.7 A systematic search for new histologic features that predict IRRAT expression and GFR is now warranted. Moreover, one histologic feature that correlates with IRRAT expression in kidney transplants with pure AKI, mild interstitial inflammation, should probably be given more weight. Interstitial inflammation is an inherent component of the injuryrepair response, like the inflammation in a healing wound, and has been described in reperfusion31,32 and DGF.33 954
Journal of the American Society of Nephrology
The IRRATs show considerable similarity to the transcripts induced in late kidneys with diseases that predict progression to renal failure in such kidneys and that can be used to define a risk score (e.g., ITGB6, VCAN, NNMT).34 Thus, 11 of the top 30 IRRATs were previously reported by us as frequently used by the molecular risk score classifier for predicting a graft loss in late kidney transplant biopsies.34 Although the significance of this observation is the subject of a separate study, it seems likely that the IRRATs are an important signal in a variety of renal diseases other than AKI, but their significance will reflect whether that disease is treatable or self-limited or untreatable and relentlessly progressive. In this respect, the close relationship between the top 30 IRRATs and cancer provides insights, illustrating the ubiquitous nature of the injury-repair/woundhealing response, and recalling the concept of cancers as “wounds that do not heal.”35,36 Thus, the IRRATs represent major general mechanisms such as development37,38 and cancer,37 particularly invasive39 and metastatic cancers,40 as well as fibrosis.41,42 Pure AKI in transplants did not lead to late graft failures in our analyses, either in the first AKI cohort or the validation set, consistent with recent studies indicating that most late kidney transplant failures reflect the onset of diseases such as late ABMR or recurrent disease.16,43 All of the kidneys in the AKI set and the validation set recovered, and the only two kidney failures were due to rejection triggered by nonadherence and recurrent GN. Thus, AKI evokes the injury-repair response, like wound healing, and does not lead to progressive deterioration in humans. At first glance this may seem to contradict some analyses of DGF in transplant registry data. However, DGF in registry data reflects many different disease states, including not only AKI but also technical failures and undetected ABMR.44,45 Moreover, kidneys with DGF carry the weight of many covariates, such as donor and recipient age, that increase the probability of both DGF and future failure.46 Thus, the impaired long-term survival of kidneys with DGF in registry data are likely not an effect of pure AKI, which is always undesirable but nevertheless inherently reversible.
CONCISE METHODS Human Biopsies for Clinical Indications, Histopathology, and Diagnoses The collection of 234 human kidney biopsies for clinical indications and eight normal nephrectomies was previously described.47 Biopsies were obtained under ultrasound guidance by spring-loaded needles (ASAP Automatic Biopsy; Microvasive, Watertown, MA). This study was approved by the University of Alberta Health Research Ethics Board (Issue #5299), the University of Illinois Chicago Office for the Protection of Research Subjects (protocol #2006-0544), and the University of Minnesota (protocol HSR#0606 M87646). Biopsies were assessed by a pathologist (M.M.), blinded to the results of molecular studies. The total interstitial inflammation (i total score, recorded as a continuous variable 48) was scored in both
J Am Soc Nephrol 23: 948–958, 2012
www.jasn.org
nonscarred and fibrotic cortical parenchyma. In addition, we assessed the interstitial fibrosis and tubular atrophy in the parenchyma. We previously described the Banff histopathologic diagnoses.47 We thus analyzed two independent sets of 28 nonrejecting biopsies each with early injury (see Results), 35 biopsies with Banff TCMR, 23 biopsies with borderline rejection, and 148 remaining biopsies representing 46 with ABMR (including 17 C4d-positive and 29 suspicious for ABMR, aka C4d-negative ABMR), 10 with mixed (ABMR/TCMR) rejection, 24 with GN, and 68 late nonrejecting biopsies. All diagnoses reflect updated donor-specific antibody status. Protocol biopsies were taken around 6 weeks post-transplant and were described previously.14 From those, we selected a subset of biopsies that represented kidneys with a stable future function (at least 2 years of follow-up), no evidence for AKI and rejection by histology, and no clinical indication for biopsy (clinical or subclinical, before or after biopsy). Thus, this subset of the pristine protocol biopsies, 11 in total, represents histologically normal kidneys whose only injury pertains
CLINICAL RESEARCH
to the transplantation process. The mean eGFR in these biopsies was 51.2 compared with a mean of 48.8 in remaining protocol biopsies. The histologic features of kidney injury assessed as the percentage of involved cortical tubules were as follows: loss of brush border, epithelium-like vacuolization, cytoplasmic lucency, and/or cell necrosis. Biopsies with $5% tubules showing such histologic features were labeled as having acute tubular injury by histology.
Renal Function Renal function was defined by estimated creatinine clearance, using a four-variable Modified Diet in Renal Disease equation at the time of biopsy and 6 months later. We also calculated the change in eGFR at 6 months after the biopsy, and studied the graft losses in the AKI cohort.
RNA Extraction and Microarrays As previously reported,49 one 18-gauge biopsy core was collected for gene expression analysis. RNA extraction, quality control, and HG_U133_Plus_2.0 GeneChip (Affymetrix Santa Clara, CA) processing were described previously. 49 Detailed protocols are available in the Affymetrix Technical Manual (www.affymetrix.com).
Microarray Data Analyses
Figure 2. Correlation of IRRAT scores (left panel) and AKI scores (right panel) with eGFR at the time of biopsy (upper panels) or change in eGFR (DeGFR) at 6 months after biopsy (lower panels) in biopsies for clinical indication with AKI. Values are Spearman correlation coefficients. AP,0.001; BP.0.05.
Microarray data files from 28 AKI biopsies, 11 protocol biopsies,14 and 8 nephrectomies were preprocessed using robust multichip averaging in Bioconductor and interquartile range filtering was used to eliminate probe sets with low variation across the dataset.34 The details of microarray expression data are posted on the Gene Expression Omnibus website (GSE30718). Discovery of transcripts differentially expressed between binary phenotypes (kidneys with AKI and pristine protocol biopsies) of both the test set and the validation set was based on the Welch t test with Benjamini–Hochberg false discovery rate correction (GeneSpring 7.3; Agilent, Santa Clara CA). A corrected P value #0.05 was considered significant. Summarized expression of transcripts in the IRRAT set (set score) was calculated as the geometric mean of the fold change values versus nephrectomies across all transcripts in a set.
Table 6. Functional annotation of IRRATs in human transplants with AKI by IPA Annotation Tool
Function or Pathway
Number of Genes Present in All 394 IRAATs (% of All IRRATs)
Number of Genes Present in the Top 30 IRRATs (% of Top 30 IRRATs)
IPA diseases and disorders IPA molecular and cellular function IPA development and function IPA canonical pathway
Cancer (n=6087) Cellular movement (n=2755) Tissue development (n=959) Acute phase response signaling (n=172)
215 (55) 131 (33) 100 (25) 19 (5)
25 (83) 19 (63) 11 (36) 4 (13)
All IRRATs $1.5-fold in AKI versus protocol biopsies (394, nonredundant) and 30 top IRRATs were used for annotation. Enrichment in Ingenuity Pathway Analysis (IPA) terms was tested by the Fisher’s exact test. All enrichments were highly significant, P,0.0001, and remained significant after the multiple test correction (P values ranged from 0.023 to ,0.0001).
J Am Soc Nephrol 23: 948–958, 2012
Acute Kidney Injury in Transplants
955
CLINICAL RESEARCH
www.jasn.org
Statistical Analyses Statistical significance of differences between the groups of biopsies was tested by Kruskal– Wallis test with Dunn’s correction for multiple comparisons. The Spearman two-tailed correlation was used to analyze relationship between features and gene set scores. The chi-squared test was used for contingency tables. P values ,0.05 were considered significant. AUC analysis tested the ability of transcripts to predict AKI.
ACKNOWLEDGMENTS The authors thank Anna Hutton and Vido Ramassar for providing technical support and Zija Jacaj for collecting the clinical data. The authors also thank Dr. Bruce Kaplan and Dr. Arthur Matas for biopsy material. The Alberta Transplant Applied Genomic Centre has been supported by Genome Canada, University of Alberta, University of Alberta Hospital Foundation, Alberta Advanced EduFigure 3. Prediction of AKI by individual transcripts. (A) Comparison of AKI biopsies to cation and Technology, Roche Molecular Syspristine protocol biopsies. All transcripts that went into the analysis are shown. (B) Only tems, Hoffmann-La Roche Canada Ltd, Alberta the top 30 IRRATs, HAVCR1, and IL18 are shown. (C) Comparison of AKI biopsies to Ministry of Advanced Education and Technolpristine protocol biopsies. Only transcripts significant at the false discovery rate of 0.05 ogy, Roche Organ Transplant Research Founare shown. (D) Vertical line indicates the uncorrected P value of 0.05. The top 30 IRdation (grants to B.S. and M.M.), Kidney RATs are represented by yellow dots, and HAVCR1 and IL18 by pink dots. Foundation of Canada, Stromedix Inc, and Astellas Canada. P.F.H. also holds a Canada ReTable 7. Relationship of the IRRAT score to the histology search Chair in Transplant Immunology and the Muttart Chair in and function of kidneys with AKI in the validation set Clinical Immunology.
eGFR at biopsya eGFR at 6 mo DeGFR by 6 mo Features of ATI (yes/no) i-total (%) Delayed/immediate graft functione Deceased/living donor
Bottom Tertile (n=9)
Middle Tertile (n=9)
Top Tertile (n=10)
39.8b 47.2 7.4b 4/5 6.3b 0/9
31.3 50.5c 20.1 7/2 2.6d 2/5
23.2 47.7c 24.9 7/3 18.8 3/6
2/7
3/5
3/7
Kruskal–Wallis test with Dunn’s correction for multiple comparisons. The top tertile was compared with the remaining tertiles. Graft function and the donor type are represented by one biopsy per patient. a eGFR and DeGFR are in milliliters per minute per 1.73 m2. b P,0.01. c Indicates significant difference between eGFR at biopsy and 6-month eGFR, by the paired t test. d P,0.001. e Missing data for two grafts.
Functional annotations of transcript sets were done using the Ingenuity Pathway Analysis Global Molecular Network. Enrichment in functional categories was tested by Fisher’s exact test. A P value ,0.05 was considered significant. 956
Journal of the American Society of Nephrology
DISCLOSURES P.F.H. holds shares in Transcriptome Sciences Inc, a company with an interest in molecular diagnostics. The other authors have no competing financial interests.
REFERENCES 1. Venkatachalam MA, Griffin KA, Lan RP, Geng H, Saikumar P, Bidani AK: Acute kidney injury: A springboard for progression in chronic kidney disease. Am J Physiol Renal Physiol 298: F1078–F1094, 2010 2. Sharfuddin AA, Molitoris BA: Pathophysiology of ischemic acute kidney injury. Nat Rev Nephrol 7: 189–200, 2011 3. Devarajan P: Update on mechanisms of ischemic acute kidney injury. J Am Soc Nephrol 17: 1503–1520, 2006 4. Siew ED, Ware LB, Ikizler TA: Biological markers of acute kidney injury. J Am Soc Nephrol 22: 810–820, 2011 5. Famulski KS, Broderick G, Einecke G, Hay K, Cruz J, Sis B, Mengel M, Halloran PF: Transcriptome analysis reveals heterogeneity in the injury response of kidney transplants. Am J Transplant 7: 2483–2495, 2007 6. Edemir B, Kurian SM, Eisenacher M, Lang D, Müller-Tidow C, Gabriëls G, Salomon DR, Schlatter E: Activation of counter-
J Am Soc Nephrol 23: 948–958, 2012
www.jasn.org
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
regulatory mechanisms in a rat renal acute rejection model. BMC Genomics 9: 71, 2008 Einecke G, Kayser D, Vanslambrouck JM, Sis B, Reeve J, Mengel M, Famulski KS, Bailey CG, Rasko JEJ, Halloran PF: Loss of solute carriers in T cell-mediated rejection in mouse and human kidneys: An active epithelial injury-repair response. Am J Transplant 10: 2241–2251, 2010 Halloran PF, de Freitas DG, Einecke G, Famulski KS, Hidalgo LG, Mengel M, Reeve J, Sellares J, Sis B: The molecular phenotype of kidney transplants. Am J Transplant 10: 2215–2222, 2010 Westhoff JH, Schildhorn C, Jacobi C, Hömme M, Hartner A, Braun H, Kryzer C, Wang CF, von Zglinicki T, Kränzlin B, Gretz N, Melk A: Telomere shortening reduces regenerative capacity after acute kidney injury. J Am Soc Nephrol 21: 327–336, 2010 Anderson S, Eldadah B, Halter JB, Hazzard WR, Himmelfarb J, Horne FM, Kimmel PL, Molitoris BA, Murthy M, O’Hare AM, Schmader KE, High KP: Acute kidney injury in older adults. J Am Soc Nephrol 22: 28–38, 2011 Bunnag S, Einecke G, Reeve J, Jhangri GS, Mueller TF, Sis B, Hidalgo LG, Mengel M, Kayser D, Kaplan B, Halloran PF: Molecular correlates of renal function in kidney transplant biopsies. J Am Soc Nephrol 20: 1149–1160, 2009 Gwinner W, Hinzmann K, Erdbruegger U, Scheffner I, Broecker V, Vaske B, Kreipe H, Haller H, Schwarz A, Mengel M: Acute tubular injury in protocol biopsies of renal grafts: Prevalence, associated factors and effect on long-term function. Am J Transplant 8: 1684–1693, 2008 Racusen L, Kashgarian M: Ischemic and toxic acute tubular injury and other ischemic renal injury. In: Heptinstall’s Pathology of the Kidney, edited by Jennette JC, Olson JL, Schwartz MM, Silva FG, 6th Ed., Philadelphia, Lippincott Williams and Wilkins, 2007, pp 1139–1198 Mengel M, Chang J, Kayser D, Gwinner W, Schwarz A, Einecke G, Broecker V, Famulski K, de Freitas DG, Guembes-Hidalgo L, Sis B, Haller H, Halloran PF: The molecular phenotype of 6-week protocol biopsies from human renal allografts: Reflections of prior injury but not future course. Am J Transplant 11: 708–718, 2011 Einecke G, Sis B, Reeve J, Mengel M, Campbell PM, Hidalgo LG, Kaplan B, Halloran PF: Antibody-mediated microcirculation injury is the major cause of late kidney transplant failure. Am J Transplant 9: 2520–2531, 2009 Sellarés J, de Freitas DG, Mengel M, Sis B, Hidalgo LG, Matas AJ, Kaplan B, Halloran PF: Inflammation lesions in kidney transplant biopsies: Association with survival is due to the underlying diseases. Am J Transplant 11: 489–499, 2011 Coca SG, Yalavarthy R, Concato J, Parikh CR: Biomarkers for the diagnosis and risk stratification of acute kidney injury: A systematic review. Kidney Int 73: 1008–1016, 2008 Vaidya VS, Ozer JS, Dieterle F, Collings FB, Ramirez V, Troth S, Muniappa N, Thudium D, Gerhold D, Holder DJ, Bobadilla NA, Marrer E, Perentes E, Cordier A, Vonderscher J, Maurer G, Goering PL, Sistare FD, Bonventre JV: Kidney injury molecule-1 outperforms traditional biomarkers of kidney injury in preclinical biomarker qualification studies. Nat Biotechnol 28: 478–485, 2010 Dieterle F, Sistare F, Goodsaid F, Papaluca M, Ozer JS, Webb CP, Baer W, Senagore A, Schipper MJ, Vonderscher J, Sultana S, Gerhold DL, Phillips JA, Maurer G, Carl K, Laurie D, Harpur E, Sonee M, Ennulat D, Holder D, Andrews-Cleavenger D, Gu YZ, Thompson KL, Goering PL, Vidal JM, Abadie E, Maciulaitis R, Jacobson-Kram D, Defelice AF, Hausner EA, Blank M, Thompson A, Harlow P, Throckmorton D, Xiao S, Xu N, Taylor W, Vamvakas S, Flamion B, Lima BS, Kasper P, Pasanen M, Prasad K, Troth S, Bounous D, Robinson-Gravatt D, Betton G, Davis MA, Akunda J, McDuffie JE, Suter L, Obert L, Guffroy M, Pinches M, Jayadev S, Blomme EA, Beushausen SA, Barlow VG, Collins N, Waring J, Honor D, Snook S, Lee J, Rossi P, Walker E, Mattes W: Renal biomarker qualification submission: A dialog between the FDA-EMEA and Predictive Safety Testing Consortium. Nat Biotechnol 28: 455–462, 2010 Perco P, Pleban C, Kainz A, Lukas A, Mayer B, Oberbauer R: Gene expression and biomarkers in renal transplant ischemia reperfusion injury. Transpl Int 20: 2–11, 2007
J Am Soc Nephrol 23: 948–958, 2012
CLINICAL RESEARCH
21. Mühlberger I, Perco P, Fechete R, Mayer B, Oberbauer R: Biomarkers in renal transplantation ischemia reperfusion injury. Transplantation 88 [Suppl]: S14–S19, 2009 22. Zhang PL, Rothblum LI, Han WK, Blasick TM, Potdar S, Bonventre JV: Kidney injury molecule-1 expression in transplant biopsies is a sensitive measure of cell injury. Kidney Int 73: 608–614, 2008 23. Hall IE, Yarlagadda SG, Coca SG, Wang Z, Doshi M, Devarajan P, Han WK, Marcus RJ, Parikh CR: IL-18 and urinary NGAL predict dialysis and graft recovery after kidney transplantation. J Am Soc Nephrol 21: 189– 197, 2010 24. Vaidya VS, Niewczas MA, Ficociello LH, Johnson AC, Collings FB, Warram JH, Krolewski AS, Bonventre JV: Regression of microalbuminuria in type 1 diabetes is associated with lower levels of urinary tubular injury biomarkers, kidney injury molecule-1, and N-acetyl-b-Dglucosaminidase. Kidney Int 79: 464–470, 2011 25. Korbély R, Wilflingseder J, Perco P, Kainz A, Langer RM, Mayer B, Oberbauer R: Molecular biomarker candidates of acute kidney injury in zero-hour renal transplant needle biopsies. Transpl Int 24: 143–149, 2011 26. Schröppel B, Krüger B, Walsh L, Yeung M, Harris S, Garrison K, Himmelfarb J, Lerner SM, Bromberg JS, Zhang PL, Bonventre JV, Wang Z, Farris AB, Colvin RB, Murphy BT, Vella JP: Tubular expression of KIM1 does not predict delayed function after transplantation. J Am Soc Nephrol 21: 536–542, 2010 27. Parikh CR, Devarajan P, Zappitelli M, Sint K, Thiessen-Philbrook H, Li S, Kim RW, Koyner JL, Coca SG, Edelstein CL, Shlipak MG, Garg AX, Krawczeski CD TRIBE-AKI Consortium: Postoperative biomarkers predict acute kidney injury and poor outcomes after pediatric cardiac surgery. J Am Soc Nephrol 22: 1737–1747, 2011 28. Parikh CR, Devarajan P, Zappitelli M, Sint K, Thiessen-Philbrook H, Li S, Kim RW, Koyner JL, Coca SG, Edelstein CL, Shlipak MG, Garg AX, Krawczeski CD, Garg AX TRIBE-AKI Consortium: Postoperative biomarkers predict acute kidney injury and poor outcomes after adult cardiac surgery. J Am Soc Nephrol 22: 1748–1757, 2011 29. Zarjou A, Agarwal A: Sepsis and acute kidney injury. J Am Soc Nephrol 22: 999–1006, 2011 30. Solez K, Morel-Maroger L, Sraer JD: The morphology of “acute tubular necrosis” in man: Analysis of 57 renal biopsies and a comparison with the glycerol model. Medicine (Baltimore) 58: 362–376, 1979 31. Avihingsanon Y, Ma N, Pavlakis M, Chon WJ, Uknis ME, Monaco AP, Ferran C, Stillman I, Schachter AD, Mottley C, Zheng XX, Strom TB: On the intraoperative molecular status of renal allografts after vascular reperfusion and clinical outcomes. J Am Soc Nephrol 16: 1542–1548, 2005 32. Bodonyi-Kovacs G, Putheti P, Marino M, Avihingsanon Y, Uknis ME, Monaco AP, Strom TB, Pavlakis M: Gene expression profiling of the donor kidney at the time of transplantation predicts clinical outcomes 2 years after transplantation. Hum Immunol 71: 451–455, 2010 33. Mas VR, Archer KJ, Yanek K, Dumur CI, Capparuccini MI, Mangino MJ, King A, Gibney EM, Fisher R, Posner M, Maluf D: Gene expression patterns in deceased donor kidneys developing delayed graft function after kidney transplantation. Transplantation 85: 626–635, 2008 34. Einecke G, Reeve J, Sis B, Mengel M, Hidalgo L, Famulski KS, Matas A, Kasiske B, Kaplan B, Halloran PF: A molecular classifier for predicting future graft loss in late kidney transplant biopsies. J Clin Invest 120: 1862–1872, 2010 35. Riss J, Khanna C, Koo S, Chandramouli GVR, Yang HH, Hu Y, Kleiner DE, Rosenwald A, Schaefer CF, Ben-Sasson SA, Yang LM, Powell J, Kane DW, Star RA, Aprelikova O, Bauer K, Vasselli JR, Maranchie JK, Kohn KW, Buetow KH, Linehan WM, Weinstein JN, Lee MP, Klausner RD, Barrett JC: Cancers as wounds that do not heal: Differences and similarities between renal regeneration/repair and renal cell carcinoma. Cancer Res 66: 7216–7224, 2006 36. Schäfer M, Werner S: Cancer as an overhealing wound: An old hypothesis revisited. Nat Rev Mol Cell Biol 9: 628–638, 2008
Acute Kidney Injury in Transplants
957
CLINICAL RESEARCH
www.jasn.org
37. Shimazui T, Oosterwijk-Wakka J, Akaza H, Bringuier PP, Ruijter E, Debruyne FM, Schalken JA, Oosterwijk E: Alterations in expression of cadherin-6 and E-cadherin during kidney development and in renal cell carcinoma. Eur Urol 38: 331–338, 2000 38. Shindo T, Kurihara H, Kuno K, Yokoyama H, Wada T, Kurihara Y, Imai T, Wang Y, Ogata M, Nishimatsu H, Moriyama N, Oh-hashi Y, Morita H, Ishikawa T, Nagai R, Yazaki Y, Matsushima K: ADAMTS-1: A metalloproteinase-disintegrin essential for normal growth, fertility, and organ morphology and function. J Clin Invest 105: 1345–1352, 2000 39. Zheng L, Pu J, Jiang G, Weng M, He J, Mei H, Hou X, Tong Q: Abnormal expression of early growth response 1 in gastric cancer: Association with tumor invasion, metastasis and heparanase transcription. Pathol Int 60: 268–277, 2010 40. Marshall FF: The level of cadherin-6 mRNA in peripheral blood is associated with the site of metastasis and with the subsequent occurrence of metastases in renal cell carcinoma. J Urol 173: 1919, 2005 41. Hahm K, Lukashev ME, Luo Y, Yang WJ, Dolinski BM, Weinreb PH, Simon KJ, Chun Wang L, Leone DR, Lobb RR, McCrann DJ, Allaire NE, Horan GS, Fogo A, Kalluri R, Shield CF 3rd, Sheppard D, Gardner HA, Violette SM: Alphav beta6 integrin regulates renal fibrosis and inflammation in Alport mouse. Am J Pathol 170: 110–125, 2007 42. Trevillian P, Paul H, Millar E, Hibberd A, Agrez MV: alpha(v)beta(6) Integrin expression in diseased and transplanted kidneys. Kidney Int 66: 1423–1433, 2004 43. Choy BY, Chan TM, Lai KN: Recurrent glomerulonephritis after kidney transplantation. Am J Transplant 6: 2535–2542, 2006
958
Journal of the American Society of Nephrology
44. Halloran PF, Hunsicker LG: Delayed graft function: State of the art, November 10-11, 2000. Summit meeting, Scottsdale, Arizona, USA. Am J Transplant 1: 115–120, 2001 45. Coca SG: Long-term outcomes of acute kidney injury. Curr Opin Nephrol Hypertens 19: 266–272, 2010 46. Terasaki PI, Gjertson DW, Cecka JM, Takemoto S, Cho YW: Significance of the donor age effect on kidney transplants. Clin Transplant 11: 366–372, 1997 47. Famulski KS, Einecke G, Sis B, Mengel M, Hidalgo LG, Kaplan B, Halloran PF: Defining the canonical form of T-cell-mediated rejection in human kidney transplants. Am J Transplant 10: 810–820, 2010 48. Mengel M, Reeve J, Bunnag S, Einecke G, Jhangri GS, Sis B, Famulski K, Guembes-Hidalgo L, Halloran PF: Scoring total inflammation is superior to the current Banff inflammation score in predicting outcome and the degree of molecular disturbance in renal allografts. Am J Transplant 9: 1859–1867, 2009 49. Mueller TF, Einecke G, Reeve J, Sis B, Mengel M, Jhangri GS, Bunnag S, Cruz J, Wishart D, Meng C, Broderick G, Kaplan B, Halloran PF: Microarray analysis of rejection in human kidney transplants using pathogenesis-based transcript sets. Am J Transplant 7: 2712–2722, 2007
This article contains supplemental material online at http://jasn.asnjournals. org/lookup/suppl/doi:10.1681/ASN.2011090887/-/DCSupplemental.
J Am Soc Nephrol 23: 948–958, 2012