Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295; © 2016 by Mohammed Siddiqui, et al. http://www.smartscitech.com/index.php/nt Special Issue Edited by Dr. Hugo R. Arias| Functional and therapeutic aspects of the nicotinic acetylcholine receptor family.
REVIEW
Nicotinic receptors in chronic kidney disease Mohammed Siddiqui1, Edgar A Jaimes2 1
University of Alabama at Birmingham, Birmingham, AL, 35233 USA Memorial Sloan Kettering Cancer Center, New York, NY, 10065 USA
2
Correspondence: Edgar A Jaimes E-mail:
[email protected] Received: March 31, 2016 Published online: May 12, 2016
Tobacco smoking is an important risk factor for cancer, cardiovascular and respiratory diseases. Cessation of tobacco smoking results in improvement of overall morbidity and mortality. There is strong evidence from human and animal studies that have demonstrated that cigarette smoking also accelerates the progression of chronic kidney disease (CKD) especially in patients with diabetes mellitus, hypertension, polycystic kidney disease, and post kidney transplant. The addictive properties of cigarette smoking are due to nicotine, which also causes important biological effects on variety of organs and tissues. Nicotine in humans causes transitory increases in blood pressure and also causes decrease in glomerular filtration rate and effective renal plasma flow. Nicotine in animals causes increase in the severity of renal injury in models with diabetic nephropathy, CKD, acute nephritis, subtotal nephrectomy and acute kidney injury (AKI). These effects of nicotine on the kidney are linked to increased generation of reactive oxygen species and activation of pro-fibrotic pathways. In normal kidney there are several nicotinic acetylcholine receptor (nAChR) subunits which are expressed, and blocking specific α7-subunit reduces the effects of nicotine in animal models with CKD. In summary, human and animal studies suggests that activation of specific nAChRs through nicotine, is responsible for the deleterious effects of cigarette smoking especially in worsening of CKD. Better understanding of these mechanisms may result in the development of novel strategies to reduce the effects of cigarette smoking in CKD. Keywords: Nicotinic Acetylcholine Receptors; Chronic Kidney Disease; α7 Nicotinic Acetylcholine Receptors; Tobacco smoking; Nicotine; Chronic Renal Disease To cite this article: Mohammed Siddiqui, et al. Nicotinic receptors in chronic kidney disease. Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295. Copyright: © 2016 The Authors. Licensed under a Creative Commons Attribution 4.0 International License which allows users including authors of articles to copy and redistribute the material in any medium or format, in addition to remix, transform, and build upon the material for any purpose, even commercially, as long as the author and original source are properly cited or credited.
acetylcholine receptors (nAChRs), which are selectively expressed in the muscles and the brain, respectively [3]
Introduction Nicotine is a potent parasympathomimetic alkaloid found in plants from the Solanaceae family. It is also a stimulant drug which constitutes 0.6–3.0% of the dry weight of tobacco approximately [1], and accounts for around 2–7 µg/kg in edible plants [2]. Nicotine is most commonly used in the form of tobacco, through smoking or chewing. It causes activation of the muscular and neuronal nicotinic
Approximately 15% of the world’s population are active smokers which accounts for more than one billion tobacco smokers worldwide [4]. The world prevalence of tobacco smoking for those above 15 years of age is approximately 33% [4]. Tobacco smoke contains more than 4,000 biologically active compounds among which nicotine is one
Page 1 of 13
Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295; © 2016 by Mohammed Siddiqui, et al. http://www.smartscitech.com/index.php/nt
of the most important, as it is present not only in large concentrations, but is also an active and biologically stable compound, largely responsible for the addictive properties of tobacco smoking [5-7]. In addition to nictone other important compounds include carbon monoxide, reactive oxygen species, metals, stable reactive aldehydes, and ketones [8].
review focuses on the nicotine effects on the kidney, and also describes the human and animal studies showing nicotine as one of the major components in tobacco that participates in the progression of CKD in smokers.
Tobacco smoking has been identified as the most important risk factor in a variety of diseases and is widely accepted as the most important cause of preventable morbidity and mortality [9, 10], and the most common cause for premature death in the adult population [4]. It is estimated that in the developed world, tobacco smoking is responsible for one in every five deaths and that diseases due to tobacco smoking are responsible for 6–15% of the total health care costs [4].
Structure
Diseases commonly linked to tobacco smoking include several types of cancers, accelerated atherosclerosis leading to coronary artery disease (CAD) and stroke (CVA), chronic respiratory conditions such as chronic obstructive pulmonary disease (COPD), eye conditions like cataracts and macular degeneration, bone diseases such as osteoporosis and gastrointestinal tract conditions like peptic ulcer disease (PUD) [4, 11]. In addition, tobacco smoking is now well accepted as a risk factor for accelerated progression of chronic kidney disease (CKD) [12] associated with etiologies such as diabetes mellitus (DM) [13] and hypertension [14]. Also, in post-renal transplant patients, tobacco smoking has been linked to worsening renal function [9]. Hence, tobacco smoking has a variety of biological effects that play an important role in the pathogenesis of several conditions, including renal disease. CKD is a major health problem globally particularly in the United States. There has not been any change in the incidence and prevalence of CKD even with advancement in treatment for major risk factors of CKD such as diabetes and hypertension [15-20]. In fact, the incidence and prevalence of CKD has been rising continuously, and has resulted in an increased number of deaths within the last 20 years, from 400,000 deaths in 1990 to 735,000 deaths in 2010 [21]. In the United States, the Center for Disease Control and prevention (CDC) estimated that between years 1999 and 2004, 16.8% adults’ ages 20 years and older had CKD [22]. Additionally, the number of patients with end stage renal disease (ESRD), the final stage in the progression of CKD, surpassed 550,000 in 2009 [23]. CKD results in progressive loss of renal function over a period of months or years. The mechanism by which smoking tobacco contributes to and causes the progression of CKD of different etiologies has not been established. This
Nicotinic acetylcholine receptors
The effects of nicotine are mediated by the activation of muscle and neuronal nicotinic acetylcholine receptors (nAChRs) [3]. The nAChRs are a group of transmembrane ligand-gated ion-channels that are formed as result of the combinatorial assembly of diverse nAChR subunits [11] symmetrically arranged around a central pore [3]. Each of the nAChRs subunits has four transmembrane domains with an extracellular located N- and C-terminus. There are 17 nAChR subunits, which are divided into neuronal and muscle-type subunits [24]. The muscle nAChRs consist of five subunits including one α (α1) and four non-α subunits (β1, δ, ε and γ). The neuronal nAChRs are formed of ten subunits that include three non-α (β2-β4) subunits and eight α-like subunits (α2-α7, α9, α10). These receptors are varied in that they are made from the various combinations of α and β subunits [3] which are mainly responsible for its special properties and functions. The structure of nAChRs can be either homopentameric (e.g., for α7 and α9 subunits) or heteropentameric. The different nAChR subunit combinations vary in their distribution, pharmacological, and kinetic properties in the brain and central nervous system. In the central nervous system, high affinity nicotine-binding receptors consist of at least α4 and β2 nAChR subunits [25-27]. The two most abundant nAChR subtypes in the brain are the α7 homo-oligomer with a binding affinity Ki 400-1500 nM and characterized by high Ca2+ permeability a rapid desensitization, low affinity and [28] and the α4β2 hetero-oligomer with a binding affinity of Ki 0.6-1.0 nM, and characterized by a high affinity and slow desensitization [27]. Less frequent combinations in nAChRs include α3β4β2, α3β4, α3β2, α6β2 and α4β4. In addition to nAChRs present in the central and peripheral nervous systems, nAChRs are also present in non-neuronal cells including vascular smooth muscle cells, bronchial epithelial cells, endothelial cells, and mesangial cells [29-34]. The composition and pharmacological properties of nAChRs in the CNS have been well characterized, but the properties of these receptors in other cells and tissues, including kidney cells, are not known and it is an area in need of further study. Ligand binding The nAChRs are directly linked to ligand-gated ion channels and do not use any second messengers (although
Page 2 of 13
Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295; © 2016 by Mohammed Siddiqui, et al. http://www.smartscitech.com/index.php/nt
the activation of α7 AChRs can activate an intracellular cascade which is triggered by Ca2+ influx). The opening of the nAChR channel pore requires binding of a chemical messenger including endogenous agonists such as acetylcholine (ACh), choline (for α7 AChRs), as well as exogenous agonists such as nicotine and epibatidine [35]. In the muscle type of nAChRs, the ACh binding sites are located in the interface of two subunits in the extracellular domain [36, 37]. The binding affinity of agonists in neuronal nAChRs is in the nanomolar range while that of muscle nAChRs is in the micromolar range [38]. In addition, the binding affinity of nicotine at neuronal nAChRs is known to be approximately 50-fold higher as compared to muscle nAChRs. Ion channel opening The nAChR is a non-selective cation channel [35]. It is permeable to both Na+ and K+ but has a higher permeability to Ca2+ [39] as in the case of α7 AChRs. The activation of these nAChR cation channels produce an influx of Na+ and Ca2+ ions and an efflux of K+ ions, resulting in an inward net flow. nAChR induced transmission The activation of nAChRs is initiated either by the movement of cations resulting in depolarization of the plasma membrane or via the activation of voltage-gated ion channels, leading to an excitatory postsynaptic potential in neurons. As result there is a direct or indirect entry of calcium, which triggers several intracellular cascades that lead to the regulation of the activity of target genes or the release of several neurotransmitters. The nicotinic receptors can be presynaptic [40] (neuronal nAChRs) as well as postsynaptic (neuronal and muscle nAChRs).The two major types of neurotransmission linked to nAChRs includes classical synaptic transmission, in which the neurotransmitter is released in high concentrations and acts on the immediate postsynaptic receptors, and paracrine transmission in which the neurotransmitter is released in synaptic buttons, and diffuses through the extracellular medium to reach their distant receptors. Biological effects of nicotine Nicotine is widely recognized as responsible for the addictive effects of tobacco smoking, but in addition nicotine has a variety of biological effects that could participate in the pathogenesis and progression of several pathologic conditions linked to smoking.
Nicotine has been shown to induce angiogenesis, accelerate atherosclerosis and promote lesion growth in animal models of lung cancer [41]. In mouse models of lung cancer, concentrations of nicotine in the nanomolar range (10 nM) stimulates the formation of capillary-like structures in cultured endothelial cells and concentrations of nicotine between 1 and 10 nM have been shown to promote endothelial cell proliferation. The angiogenic effects of nicotine in these studies were partially dependent on vascular endothelial growth factor (VEGF) and in large part mediated by phosphatidylinositol 3-kinase, mitogen activated protein kinase pathways and NF-κB (nuclear factor kappa-light-chain-enhancer of activated B cells) activation [33] . Nicotine can also induce proliferation of other cell types including vascular endothelial and smooth muscle cells from bovine aorta. These effects are mediated by increased generation of basic fibroblast growth factor (bFGF) and platelet derived growth factor [42-44]. In these studies it was also observed that nicotine reduced transforming growth factor (TGF-β) release by endothelial cells and that these effects were concentration dependent [42-44]. These proliferative effects of nicotine are concentration dependent, where a significant proliferative response is seen at nicotine concentrations of 60 nM and peaking at concentrations of 600 nM, concentrations that are unlikely to occur in vivo in smokers. Nicotine through its stable metabolite cotinine can also induce migration of human vascular smooth muscle cells at concentrations between 10 and100 nM. These effects are independent of the activation of specific nAChRs and mediated by increased production of bFGF and expression of matrix metalloproteinases such as collagenase-1, stromelysin-1 and gelatinase A [45]. The administration of nicotine in vivo at a concentration of 100 μg/mL in the drinking water, results in nicotine levels similar to those found in the plasma of active smokers. At these concentrations nicotine produces a significant increase in the formation of atherosclerotic plaque in Apo-E deficient mice and also stimulates neovascularization after limb ischemia [33]. The administration of nicotine at these concentrations does not increase the formation of atherosclerotic plaque in Apo E deficient mice that also lacked CD36, an important mediator of oxidized LDL (oxLDL) uptake and also contributor of macrophage foam formation [33]. In these studies the stimulation of macrophages with nicotine in vitro at concentrations of 100 nM had synergistic effects with oxidized Low Density Lipoprotein (LDL) on the expression of pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α), monocyte chemoattractant protein-1 (MCP-1), interleukin-6 (IL-6) and chemokine (C-X-C motif) ligand 9 (CXCL-9) [46]. These effects of nicotine on angiogenesis are prevented by specific blockade of the α7 nAChR indicating that this
Page 3 of 13
Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295; © 2016 by Mohammed Siddiqui, et al. http://www.smartscitech.com/index.php/nt
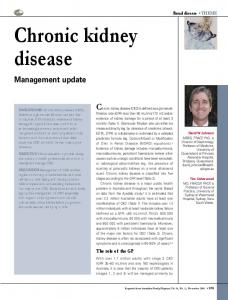
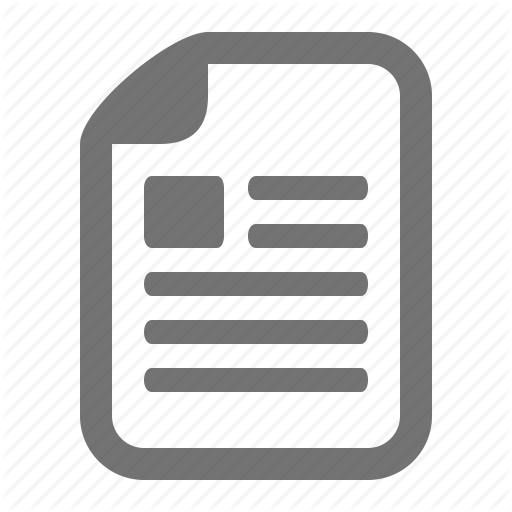
Figure 1. Localization of α7 nAChRs in cortex. Panel A: Incubated with primary antibody not with secondary antibody (20 X) - Control slide. Panel B: Representative photomicrograph showing expression of α7 nAChRs in proximal tubules identified by Lotus tetragonolobus lectin (20 X). Panel C: Representative photomicrograph of a slide showing expression of α7 nAChRs in distal tubules as identified by peanut agglutinin (20 X). Panel D: Representative photomicrograph demonstrating lack of expression of α7 nAChRs in the intra-renal vasculature (20 X).
receptor is involved in these effects [33].Similarly, in the Lewis lung cancer mouse models the administration of nicotine in vivo increases tumor size [33]. In addition to these pro-proliferative effects, nicotine increases extracellular matrix production and deposition in various cell types. Administration of nicotine at concentrations of 10-100 µg/mL in vivo and/or in vitro causes increases in the production of fibronectin by lung fibroblasts via protein kinase C activation, mitogen-activated protein kinases (MAPKs) activation, increased intracellular levels of cyclic adenosine monophosphate (cAMP) and deoxyribonucleic acid (DNA) binding to the transcription factor cAMP response element-binding protein (CREB) [47]. Moreover, nicotine at micromolar concentrations and via activation of α3-containing nAChRs, produce increases in type 1 collagen, metalloproteinase-1 (elastin and matrix) and also cell cycle regulators such as cyclin-dependent kinase inhibitor / interacting protein 1 (p21), cyclin D1, anigen Ki-67 and proliferating cell nuclear antigen (PCNA) in dermal fibroblasts [48]. Nicotine at concentrations of 1 µM, induces cell proliferation via β-arrestin-mediated activation
of Src and Rb-Raf-1 pathways in non-small cell lung cancer cell lines [49]. Importantly, these effects were prevented by α7 nAChR blockade suggesting that were mediated by α7 nAChR containing receptors. In addition, in human coronary artery endothelial cells, nicotine at concentrations between 100 nM to 10 µM increases the mRNA levels of endothelial nitric oxide synthase (eNOS), plasminogen activator inhibitor, angiotensin-I converting enzyme, tissue type plasminogen activator, von Willebrand factor and vascular cell adhesion molecule-1 [50]. Nicotinic receptors in kidney derived cells In studies from our laboratory we demonstrated the expression of several nAChR subunits, including α4, α5, α7, β2, β3 and β4 in human mesangial cells [34]. Among these subunits, the α7 subunit has been identified as one of the most important subunits for numerous cholinergic actions mediated by nAChRs in macrophages, vascular smooth muscle cells and cancer cell lines [51, 52]. In the normal
Page 4 of 13
Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295; © 2016 by Mohammed Siddiqui, et al. http://www.smartscitech.com/index.php/nt
kidney, the renal cortex expresses the α7 subunit predominantly in the proximal tubules and at a lesser extent in the distal tubules [53] (Figure 1). There are also regional differences in the vascular expression of the α7 nAChR, since we did not detect measurable amounts of this subunit in the intrarenal vasculature in contrast to its expression in the systemic vasculature [33, 34]. Effects of nicotine in renal disease Tobacco smoking is well established as a risk factor in the progression of CKD secondary to well-established risk factor for renal disease like diabetes and hypertension [3, 12, 17, 24, 31, 39, 54] . The role of nicotine as a mediator of the deleterious effects of tobacco smoking in renal disease has been investigated in models of renal injury including models of acute kidney injury (AKI), CKD, diabetes nephropathy and glomerular diseases. Recently, we reported the role of the α7 nAChR on the effects of nicotine in the progression of CKD. For these studies we used a rat model of CKD induced by subtotal nephrectomy (5/6Nx), which results in progressive glomerulosclerosis and fibrosis similar to the changes observed in humans with CKD [55, 56]. In rats with 5/6Nx, the administration of nicotine at concentrations of 100 µg/L in the drinking water for 12 weeks resulted in a small increase in blood pressure [57] and cotinine levels similar to those found in the plasma of active smokers [57]. In rats with 5/6Nx the administration of nicotine led to significant increases in urinary protein excretion, higher glomerular injury score and increased cortical expression of fibronectin and TGF-β, an important growth factor involved in extracellular matrix production [58]. The administration of nicotine to these rats also resulted in a large increase in the cortical expression of nitrotyrosine, a marker of oxidative stress, and of the NADPH isoform NADPH oxidase 4 (NOX4) [53]. These effects were prevented by the α7 nAChR competitive antagonist methyllycaconitine (MLA) indicating that they were mediated by α7 nAChR containing receptors. These studies also suggest that since the proximal tubules are a source of both pro-fibrotic and pro-inflammatory cytokines, the activation of tubular α7 nAChRs maybe mediating the increased production of these mediators [53, 59]. We have also demonstrated that nicotine at concentrations of 100 nM (similar to peak concentrations found in the plasma of active smokers) stimulates cell proliferation in human mesangial cells as well as the production of the extracellular matrix protein fibronectin [60]. These effects of nicotine were inhibited by α-bungarotoxin at nanomolar concentrations, suggesting they were mediated by α7 nAChR containing receptors. Nicotine induced proliferation of human mesangial cells and fibronectin production were also
prevented by α-lobeline and dihydro-β-erythroidine suggesting a role for nAChRs containing the α4 and β2 subunits [34]. In addition, the proliferative and pro-fibrotic actions of nicotine were prevented by two different NADPH oxidase inhibitors, demonstrating the role of NADPH oxidase derived Reactive Oxygen Species (ROS) generation on these effects and also demonstrating that the enzyme NADPH oxidase is the main source of ROS in response to nicotine [34]. It is well recognized that protein kinase C (PKC) is required for NADPH oxidase activation in several cell types [61, 62] . PKC inhibition also reduced the proliferative and pro-fibrotic effects of nicotine in these studies indicating that PKC activation is required for these effects, probably via NADPH oxidase activation. NADPH oxidase mediated ROS promote the activation of MAPKs [63, 64] such as extracellular-signal-regulated kinases (ERK1 and ERK2), which promote growth related responses [61, 65], including proliferation and differentiation in response to Angiotensin II [61] , platelet-derived growth factor (PDGF) [65] and TGF-β [66]. Nicotine at a concentration of 100 nM induces ERK1 and ERK2 phosphorylation and specific ERK1 and ERK2 inhibitors of these MAPKS prevent mesangial cell proliferation and fibronectin production in response to nicotine, suggesting a role for these MAPKS on these effects[34, 67]. Nicotine also increases cyclooxygenase-2 (COX-2) expression and activity in human mesangial cells and COX-2 inhibition reduces nicotine-induced mesangial cells proliferation and production of fibronectin, suggesting that COX- 2 derived prostaglandins produced in response to nicotine may play a major role as mediators of glomerular injury in response to nicotine [68]. Indeed, COX-2 inhibition in a model of renal ablation significantly reduces mesangial cell proliferation, mesangial matrix expansion, glomerular sclerosis, expression of fibronectin and collagen IV [69]. Moreover, pro-inflammatory cytokines and Angiotensin II also have been seen to induce COX-2 via NADPH oxidase derived ROS [70, 71]. NADPH oxidase inhibition reduces COX-2 expression in vivo in response to nicotine stimulation, suggesting that COX-2 derived prostaglandins may be playing a role in the deleterious pro-angiogenic and pro-atherosclerotic effects of nicotine in renal disease [41]. Nicotine at concentrations of 200 μM also increases the production of ROS from NADPH oxidase and mitochondria in cultured renal proximal tubule cells [72], resulting in oxidative stress and leading to JNK mediated activation of the activator protein-1 (AP-1) transcription factor in vitro.. In addition, nicotine at concentrations of 200 µM and via expression of USTAT3, a unphosphorylated form of signal transducer and activator of transcription-3 (which is a
Page 5 of 13
Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295; © 2016 by Mohammed Siddiqui, et al. http://www.smartscitech.com/index.php/nt
noncanonical mediator of inflammation and fibrosis), enhances the effects of TGF-β on α-SMA, vimentin and fibronectin production in proximal tubular cells [73] and unveiling another potential mechanism that may be involved in the deleterious effects of nicotine in renal disease. The administration of nicotine at a concentration of 200 µg/mL in the drinking water in rat models of warm-ischemia reperfusion is linked to increased expression of markers of oxidative stress including nitrotyrosine and malondialdehyde, worsening of renal injury, and reduced renal function [72]. Similar findings were also observed but without morphologic alterations in sham-operated rats and were associated with kidney sensitization, facilitating the progression of acute kidney injury to chronic kidney injury [72]. Importantly the plasma concentrations of cotinine observed (127–134 ng/mL) in these studies were within the range described in active smokers [74]. In another study, nicotine induced a pro-inflammatory to pro-fibrotic phenotype shift in isolated macrophages which could also be a mechanism by which nicotine promotes fibrosis [75]. In contrast, however other studies have shown that the administration of a single nicotine injection of 1 mg/kg IP before injury attenuates the severity of renal injury in rodent models of ischemia reperfusion and sepsis [76, 77]. Also in these studies administration of nicotine was associated with reduction in inflammatory infiltrates, expression of pro-inflammatory cytokines and NF-kB activation [76, 77], suggesting that nicotine can have anti-inflammatory effects under specific circumstances. However, in these studies the concentrations of cotinine or other stable nicotine metabolites were not measured. Therefore, studies from isolated macrophages suggest that nicotine can induce changes in macrophages from a pro-inflammatory to a more pro-fibrotic phenotype [75] . The effects of nicotine have also been investigated in models of glomerulonephritis. In the anti-Thymocyte differentiation antigen 1 (Thy1) glomerulonephritis model, a single injection of anti-Thy1 antibody causes initial mesangiolysis followed by transient glomerular cell proliferation, inflammation and fibronectin production which resolves spontaneously after 4 weeks [78, 79]. In this model of glomerulonephritis the administration of nicotine at concentrations of 100 µg/mL in the drinking water resulted in cotinine levels around 60 ng/ml and increased glomerular cell proliferation and fibronectin production [68]. These changes were also accompanied by an increase in the inducible COX isoform COX-2, a major source of prostaglandins in the kidney [70]. COX-2 expression has been shown to be increased in glomerular inflammatory conditions such as acute glomerulonephritis and ureteral obstruction [80-82] and also in experimental models of diabetes [83, 84] and
CKD [85, 86]. In the Munich–Wistar–Frömter rat model of proteinuria-induced renal inflammation, the long term administration of nicotine at concentrations of 20–100 µg/mL in the drinking water, resulted in improvements in proteinuria and renal function [87]. These rats have a reduced number of podocytes [88] which results in spontaneous albuminuria that is under polygenic influence and linked to a trait locus on the rat chromosome 8 [89]. Chronic albuminuria in this model is linked with progressive glomerulosclerosis and fibrosis [89]. The plasma levels of cotinine obtained from this experiment varied by nicotine dosages, 139 ng/mL for lower doses and more than 500 ng/mL for higher doses. In these studies the administration of nicotine also reduced glomerular sclerosis, desmin deposition, podocin loss, and number of renal macrophages and myofibroblasts. It also reduced the expression of MCP-1 and vascular cell adhesion protein (VCAM) [86]. In db/db mice, a well-established model of type II diabetes that after several weeks of hyperglycemia develops mesangial expansion, glomerular hypertrophy, increased expression and deposition of extracellular matrix proteins such as fibronectin and collagen IV, and increased expression of pro-fibrotic cytokines including TGF-β [90]. These changes are accompanied by increased urinary albumin excretion and proteinuria, resembling the changes of diabetic nephropathy of humans [91]. These mice have a leptin receptor mutation that leads to defective signaling of the adipocyte hormone leptin [92, 93] which causes polyphagia, obesity and insulin resistance followed by diabetes mellitus. In these mice the administration of nicotine at a concentration 100 μg/mL in the drinking water resulted in worsening glomerular hypertrophy and mesangial expansion with increase in urinary albumin excretion and without significant hemodynamic changes [67]. The administration of nicotine to non-diabetic mice resulted in a small increase in cortical fibronectin expression, while diabetic mice had a significant increase in cortical fibronectin [67]. Diabetes mellitus has been associated with increases in oxidative stress [94, 95] and increased expression in cortical NOX4, the most abundant form of NADPH oxidase in the kidney [95]. The administration of nicotine to diabetic mice increased cortical NOX4, nitrotyrosine expression and Akt/PKB phosphorylation, a serine-threonine kinase Akt/PKB activated by ROS that plays a major role in cell growth and matrix expansion in diabetic nephropathy [95] . The effects of nicotine on renal disease and the mechanisms involved are complex and are mediated by
Page 6 of 13
Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295; © 2016 by Mohammed Siddiqui, et al. http://www.smartscitech.com/index.php/nt
activation of specific nAChRs. Importantly these effects are not universal and are highly dependent on the specific animal models and experimental conditions. However several experimental studies suggest that nicotine is a potential mediator of the deleterious effects of tobacco smoking in renal injury, and it seems to be particularly relevant to the progression of CKD. It is important to note that tobacco smoke contains thousands of biologically active compounds other than nicotine and that therefore some of the adverse effects observed in humans cannot be attributed entirely to nicotine. Effects of tobacco smoking in humans Clinical and epidemiological studies have shown an association between tobacco smoking and increases in urinary albumin excretion in normal healthy patients with no renal disease and in subjects with underlying diseases such as diabetes and hypertension, implying that tobacco smoking is a contributor to the development of “de novo” renal injury [17, 24, 31, 39, 54] . In the initial stages of renal injury of diverse etiologies, there is an increase in fractional filtration rate and the subsequent development of intraglomerular hypertension which has been postulated as a mechanism implicated in the progression of CKD [96]. These changes are also linked to a decrease in renal plasma flow and an increase in albumin excretion (well-known markers of early renal injury) and occur in the absence of any significant changes in GFR or serum creatinine [97]. In one study, 24 non-smokers were compared to 30 cigarette smokers (13 current smokers, and 17 former smokers), and their renal function was evaluated by clearance of technetium-99m-diethylenetriamine penta-acetic acid (DTPA scan) to measure GFR, and by clearance of technetium-99m-mercaptoacetyltriglycine (MAG3 scan) to assess renal plasma flow [98]. Although GFR was no different among smokers and not smokers, renal plasma flow measured was significantly lower in smokers (199.20 ± 58.85 mL/min per 1.73 m2) as compared non-smokers (256.54 ± 60.14 mL/min per 1.73 m2, p < 0.001). These findings therefore suggest that smoking is linked to changes in renal perfusion that could have a long term impact on renal function. A cross-sectional survey completed on a cohort from the Norwegian general population investigated the effects of tobacco smoking use, obesity and physical inactivity on CKD [99]. This study showed, after adjusting for age and sex, a relative risk of 1.52 (95% CI 1.13–2.06) for the development of CKD in tobacco smokers with a history of >25 pack years of smoking. Another similar study in the general population of Australia found an association between
tobacco smoking and CKD in men, with an odds ratio of 3.59 but no association between CKD and tobacco smoking in women. The reasons for these gender differences in this study were not investigated [101, 102]. Another study however found that tobacco smoking was independent risk factor for the development of CKD among women [103]. [100]
In the HOPE (Heart Outcomes and Prevention Evaluation) study it was observed that tobacco smoking was an independent risk factor for microalbuminuria in both diabetic and non-diabetic patients and linked to the number of cigarettes smoked suggesting a “dose dependent” effect [104]. The Chronic Renal Insufficiency Cohort (CRIC) study investigated risk factors for CKD in over 3,500 CKD patients. The results of the CRIC study showed an association between tobacco smoking and lower eGFR [105]. Another recent study also showed that smoking increased the risk of CKD in the general population (OR = 1.6, p = 0.009, 95% CI = 1.12– 2.29), where the highest risk was for patients with preexisting hypertension, diabetes [41], and heavy cigarette smoking. Other studies have also demonstrated that smoking in a dose-dependent manner, increases urinary albumin excretion and worsens renal function in the general population as well as in subjects with pre-existing renal disease [18, 19]. Tobacco smoking, either active smoking or passive/second hand smoke exposure, has also been shown to have deleterious effects on renal function in younger individuals as shown by a study that evaluated the effects of active smoking and passive/second hand smoke exposure among adolescents [106]. In this study the median eGFR in non-smokers was 99.1 (88.1-111.0) mL/min per 1.73 m2 compared to those exposed to second hand smoke 96.8 (85.0-109.0) mL/min per 1.73 m2 and to those who smoked 90.1 (81.3-100.9) mL/min per 1.73 m2 [106]. Role of tobacco smoking in patients predisposing to CKD with comorbidities For subjects with coexisting comorbidities such as diabetes, hypertension, or adult polycystic kidney disease (ADPKD), tobacco smoking is a risk factor for increased urine albumin excretion and faster progression of CKD [18, 23] . Hypertension In a prospective study, hypertensive smokers were treated to a target MAP of 100 mmHg, and followed for 3 years; these subjects had more microalbuminuria as compared to normotensive patients who smoked and to hypertensive subjects who did not smoke [15, 16], underscoring the additive
Page 7 of 13
Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295; © 2016 by Mohammed Siddiqui, et al. http://www.smartscitech.com/index.php/nt
harmful effects of tobacco smoking in patients with underlying vascular disease such as hypertension [107]. Based on the findings of this study it could be concluded that tobacco smoking is an important risk factor for predicting a decline in eGFR [9]. The relationship between tobacco use and increased urine albumin excretion in patients with hypertension has been demonstrated in numerous studies [108, 109] . A number of studies have shown an association between tobacco smoking and hypertension with a higher risk associated with longer duration of smoking and number of cigarettes smoked per day [110-112]. Tobacco smoking causes direct postganglionic sympathetic nerve ending stimulation resulting in increased plasma concentrations of norepinephrine and epinephrine and subsequent increases in blood pressure, heart rate and vascular resistance [113], effects that can be inhibited by β1-receptor antagonism [114]. Tobacco smoking also causes elevation of adrenocorticotrophic hormone and aldosterone levels in patients with essential hypertension[115]. The kidney response to increased systemic blood pressure may be impaired by smoking leading to increased GFR and possibly increased intraglomerular pressure, when compared to non-smokers that have the normal reno-protective decrease in GFR and effective renal plasma flow [110]. Those who smoke are more prone to atherosclerotic renal artery stenosis than who do not smoke [116]. Diabetes Tobacco smoking is linked to new onset of microalbuminuria, faster progression of microalbuminuria to macro albuminuria, and a decrease in GFR in diabetics [7, 23, 96, 104, 107, 117-120] . In smokers with type I diabetes mellitus there is a 2.8-fold higher incidence of albuminuria[118]. Tobacco smoking has also been shown to have deleterious effects on CKD in patients with type II diabetes in which a significant elevation in serum creatinine, increase in urinary albumin excretion, and progression of diabetic nephropathy was noted in tobacco smokers followed for 5 years, in spite of good glycemic and blood pressure control, and treatment with RAS blocking agents [7]. In a clinical prediction rule study the development of microalbuminuria in patients with type I diabetes, tobacco smoking was found to be a clinically relevant predictor (OR 1.40, CI 1.16, 1.69 in multivariate analysis) of baseline albumin excretion rate, glycosylated hemoglobin, body mass index and waist to hip ratio [121]. Another prospective study conducted in 91 patients with type II diabetes that included smokers, former smokers and non-smokers. These patients were treated on recommended BP and glycemic control and followed prospectively for 5 years; annual measurements of eGFR and urinary albumin excretion indicated that smokers had a 17% higher
macroalbuminuria (p < 0.003) and a faster eGFR decline rate than patients who did not smoke and former smokers [122]. Additional studies have also demonstrated faster progression of CKD in both type I and type II diabetics who smoke [123, 124] . Among subjects with diabetic nephropathy smokers have also shown to have higher resting energy expenditure, increased levels of biomarkers of oxidative stress and inflammation [125]. Glomerular Diseases Two retrospective studies in patients with CKD secondary to primary glomerulopathies have demonstrated the association between smoking and CKD progression in older men (though similar results were not seen in women) [101, 102]. In another retrospective study of 160 patients with lupus nephritis, tobacco smokers developed End Stage Renal Disease (ESRD) faster as compared to those who did not smoke (145 months vs. 273 months) [126]. Autosomal polycystic kidney disease Tobacco smoking is independently associated with proteinuria and rapid progression of kidney disease in patients with autosomal polycystic kidney disease [127, 128]. Tobacco smoking and its effects on renal allografts In the United States population, studies on over 40,000 renal transplant recipients have demonstrated that smokers have worse outcomes, including death censored allograft loss as well as increased mortality [9, 103, 105, 106, 129]. Of these, 9.9% were found to be prior smokers and 4.6% were noted to start smoking after transplantation. In new smokers, tobacco smoking was associated with increased risk of death-censored graft loss (adjusted hazard ratio 1.46, 95% CI 1.19–1.79, p < 0.0001) and death (adjusted hazard ratio 2.26, 95% CI 1.91– 2.66, p < 0.001). Importantly in former smokers, tobacco smoking also increased the risk of death and censored allograft loss (adjusted hazard ratio of 1.20, 95% CI 1.06–1.35, p = 0.003). In addition smokers at the time of the transplant (25 pack-year smoking history) had a 30% higher risk of graft failure (relative risk 1.30; 95% confidence interval [CI], 1.04–1.63; p = 0.021) as compared to non-smokers and patients who smoked less than 25 pack-years [9]. There was also reduced kidney graft survival in smokers at the time of transplant evaluation of 84%, 65%, and 48% at 1, 5, and 10 years, respectively, compared with graft survival on individuals that did not smoke (88%, 78%, and 62%; p = 0.007) [130]. Another study showed that smokers had worse renal allograft function at 3 years after renal transplantation as compared non smokers (1.45 ± 0.55 mg/dL vs. 1.57 ± 0.48 mg/dL, p < 0.05) [105]. In
Page 8 of 13
Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295; © 2016 by Mohammed Siddiqui, et al. http://www.smartscitech.com/index.php/nt Table 1. Summary of clinical effects of nicotine in humans Increased albumin excretion Progression of microalbuminuria to macroalbuminuria in diabetic patients Increased incidence of renal artery stenosis Decreased eGFR - Subtle as measured by renal perfusion scans- Frank reduction as measured by serum creatinine Decreased renal allograft survival Increased mortality in patients with ESRD
a single center living donor kidney transplant recipients study, smokers had worse allograft survival (p = 0.01), overall survival (p = 0.02), as well as rejection free first year as compared to non-smokers (p = 0.03) [106]. In a multivariate analysis of a prospective study on patients older than 60 years and who underwent cadaveric kidney transplants [129], showed that tobacco smoking was one of three modifiable risk factors for patient survival [hazard ratio (HR) 2.09, 95% confidence interval (CI) 1.22–3.60], others being BMI and time on dialysis prior to transplant. Moreover smoking was found to be the only modifiable risk factor linked to renal allograft survival (HR 2.04, 95% CI 1.24–3.30). In addition history of smoking in kidney donors has been shown to have detrimental effects on both allograft survival (HR 1.05, p < 0.05) and recipient survival (HR 1.06, p < 0.05) [131]. Conclusion In conclusion, there is a large amount of evidence about the adverse effects of tobacco smoking on renal function such as increased urinary albumin excretion, increased incidence of renal artery stenosis, increased mortality in patients with ESRD, faster progression of microalbuminuria to macro albuminuria in diabetic patients, decrease in eGFR, and reduced renal allograft survival (Table 1). Several experimental studies suggest that the activation of nicotinic receptors in smokers may be one of the mechanisms by which tobacco smoking accelerates the progression of renal disease. The effects of tobacco smoking start at an early age, and have a long lasting effect. There is also a significant impact on health care outcomes and cost. The increasing prevalence of CKD needs to be halted by controlling the mechanisms that lead to its progression, particularly by tobacco smoking cessation. In future studies it will be necessary to determine the association and the mechanisms involved in tobacco smokers in which nicotinic receptors are activated by nicotine causing the progression of CKD in humans. Moreover, given the growing use of electronic cigarettes additional experimental and clinical studies will be needed to determine the effects of these non-combustible tobacco products on renal disease.
Acknowledgements The authors acknowledge the assistance provided by Johanna Lehner and Alma Feliciano in the drafting and submission of this manuscript. References 1.
Hoffmann, D and Hoffmann, I. The changing cigarette, 1950-1995. J Toxicol Environ Health 1997; 50: 307-364.
2.
Siegmund, B, Leitner, E and Pfannhauser, W. Determination of the nicotine content of various edible nightshades (Solanaceae) and their products and estimation of the associated dietary nicotine intake. J Agric Food Chem 1999; 47: 3113-3120.
3.
Albuquerque, EX, Pereira, EF, Alkondon, M and Rogers, SW. Mammalian nicotinic acetylcholine receptors: from structure to function. Physiol Rev 2009; 89: 73-120.
4.
Fagerstrom, K. The epidemiology of smoking: health consequences and benefits of cessation. Drugs 2002; 62 Suppl 2: 1-9.
5.
Stedman, RL. The chemical composition of tobacco and tobacco smoke. Chem Rev 1968; 68: 153-207.
6.
Changeux, JP. Nicotinic receptors and nicotine addiction. C R Biol 2009; 332: 421-425.
7.
Albuquerque, EX, Pereira, EF, Castro, NG, Alkondon, M, Reinhardt, S, Schroder, H, et al. Nicotinic receptor function in the mammalian central nervous system. Ann N Y Acad Sci 1995; 757: 48-72.
8.
Huang, MF, Lin, WL and Ma, YC. A study of reactive oxygen species in mainstream of cigarette. Indoor Air 2005; 15: 135-140.
9.
Boyle, P. Cancer, cigarette smoking and premature death in Europe: a review including the Recommendations of European Cancer Experts Consensus Meeting, Helsinki, October 1996. Lung Cancer 1997; 17: 1-60.
10. McBride, PE. The health consequences of smoking. Cardiovascular diseases. Med Clin North Am 1992; 76: 333-353. 11. Steenland, K, Thun, M, Lally, C and Heath, C, Jr. Environmental tobacco smoke and coronary heart disease in the American Cancer Society CPS-II cohort. Circulation 1996; 94: 622-628. 12. Jain, G and Jaimes, EA. Nicotine signaling and progression of chronic kidney disease in smokers. Biochem Pharmacol 2013; 86: 1215-1223. 13. Chuahirun, T and Wesson, DE. Cigarette smoking predicts faster progression of type 2 established diabetic nephropathy despite ACE inhibition. Am J Kidney Dis 2002; 39: 376-382.
Conflicting interests The authors have declared that no conflict of interests exist.
14. Yacoub, R, Habib, H, Lahdo, A, Al Ali, R, Varjabedian, L, Atalla, G, et al. Association between smoking and chronic kidney disease: a case control study. BMC Public Health 2010; 10: 731.
Page 9 of 13
Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295; © 2016 by Mohammed Siddiqui, et al. http://www.smartscitech.com/index.php/nt 15. Pinto-Sietsma, SJ, Mulder, J, Janssen, WM, Hillege, HL, de Zeeuw, D and de Jong, PE. Smoking is related to albuminuria and abnormal renal function in nondiabetic persons. Ann Intern Med 2000; 133: 585-591. 16. Tozawa, M, Iseki, K, Iseki, C, Oshiro, S, Ikemiya, Y and Takishita, S. Influence of smoking and obesity on the development of proteinuria. Kidney Int 2002; 62: 956-962. 17. Hillege, HL, Janssen, WM, Bak, AA, Diercks, GF, Grobbee, DE, Crijns, HJ, et al. Microalbuminuria is common, also in a nondiabetic, nonhypertensive population, and an independent indicator of cardiovascular risk factors and cardiovascular morbidity. J Intern Med 2001; 249: 519-526. 18. Halimi, JM, Giraudeau, B, Vol, S, Caces, E, Nivet, H, Lebranchu, Y, et al. Effects of current smoking and smoking discontinuation on renal function and proteinuria in the general population. Kidney Int 2000; 58: 1285-1292. 19. Ishizaka, N, Ishizaka, Y, Toda, E, Shimomura, H, Koike, K, Seki, G, et al. Association between cigarette smoking and chronic kidney disease in Japanese men. Hypertens Res 2008; 31: 485-492. 20. Dyck, RF, Hayward, MN, Harris, SB and Group, CS. Prevalence, determinants and co-morbidities of chronic kidney disease among First Nations adults with diabetes: results from the CIRCLE study. BMC Nephrol 2012; 13: 57. 21. Lozano, R, Naghavi, M, Foreman, K, Lim, S, Shibuya, K, Aboyans, V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380: 2095-2128. 22. Prevalence of Chronic Kidney Disease and Associated Risk Factors --- United States, 1999--2004. 2007, Centers for disease control and prevention (CDC). 23. Collins, AJ, Foley, RN, Chavers, B, Gilbertson, D, Herzog, C, Johansen, K, et al. 'United States Renal Data System 2011 Annual Data Report: Atlas of chronic kidney disease & end-stage renal disease in the United States. Am J Kidney Dis 2012; 59: A7, e1-420. 24. Le Novere, N and Changeux, JP. Molecular evolution of the nicotinic acetylcholine receptor: an example of multigene family in excitable cells. J Mol Evol 1995; 40: 155-172.
human keratinocytes. J Invest Dermatol 1995; 105: 774-781. 30. Maus, AD, Pereira, EF, Karachunski, PI, Horton, RM, Navaneetham, D, Macklin, K, et al. Human and rodent bronchial epithelial cells express functional nicotinic acetylcholine receptors. Mol Pharmacol 1998; 54: 779-788. 31. Macklin, KD, Maus, AD, Pereira, EF, Albuquerque, EX and Conti-Fine, BM. Human vascular endothelial cells express functional nicotinic acetylcholine receptors. J Pharmacol Exp Ther 1998; 287: 435-439. 32. Wessler, I, Kirkpatrick, CJ and Racke, K. The cholinergic 'pitfall': acetylcholine, a universal cell molecule in biological systems, including humans. Clin Exp Pharmacol Physiol 1999; 26: 198-205. 33. Heeschen, C, Weis, M, Aicher, A, Dimmeler, S and Cooke, JP. A novel angiogenic pathway mediated by non-neuronal nicotinic acetylcholine receptors. J Clin Invest 2002; 110: 527-536. 34. Jaimes, EA, Tian, RX and Raij, L. Nicotine: the link between cigarette smoking and the progression of renal injury? Am J Physiol Heart Circ Physiol 2007; 292: H76-82. 35. Purves D, AGJ, Fitzpatrick D, Hall WC, Lamantia AS, McNamara JO, White LE Neuroscience, Fourth Edition. Vol. 4th Edition. 2008. 36. Squire, LR. Fundamental neuroscience. 2nd ed. 2003, Amsterdam ; San Diego, Calif. ; London: Academic Press. xix, 1426 p. 37. Siegel GJ, AB, Fisher SK, Albers RW, Uhler MD. GABA Receptor Physiology and Pharmacology, in Basic Neurochemistry: 6th Edition, Molecular, Cellular and Medical Aspects. 1999. 38. Rozental, R, Aracava, Y, Scoble, GT, Swanson, KL, Wonnacott, S and Albuquerque, EX. Agonist recognition site of the peripheral acetylcholine receptor ion channel complex differentiates the enantiomers of nicotine. J Pharmacol Exp Ther 1989; 251: 395-404. 39. Unwin, N. Refined structure of the nicotinic acetylcholine receptor at 4A resolution. J Mol Biol 2005; 346: 967-989. 40. Wonnacott, S. Presynaptic nicotinic ACh receptors. Trends Neurosci 1997; 20: 92-98. 41. Heeschen, C, Jang, JJ, Weis, M, Pathak, A, Kaji, S, Hu, RS, et al. Nicotine stimulates angiogenesis and promotes tumor growth and atherosclerosis. Nat Med 2001; 7: 833-839.
25. Flores, CM, DeCamp, RM, Kilo, S, Rogers, SW and Hargreaves, KM. Neuronal nicotinic receptor expression in sensory neurons of the rat trigeminal ganglion: demonstration of alpha3beta4, a novel subtype in the mammalian nervous system. J Neurosci 1996; 16: 7892-7901.
42. Cucina, A, Corvino, V, Sapienza, P, Borrelli, V, Lucarelli, M, Scarpa, S, et al. Nicotine regulates basic fibroblastic growth factor and transforming growth factor beta1 production in endothelial cells. Biochem Biophys Res Commun 1999; 257: 306-312.
26. McCallum, SE, Collins, AC, Paylor, R and Marks, MJ. Deletion of the beta 2 nicotinic acetylcholine receptor subunit alters development of tolerance to nicotine and eliminates receptor upregulation. Psychopharmacology (Berl) 2006; 184: 314-327.
43. Cucina, A, Sapienza, P, Corvino, V, Borrelli, V, Randone, B, Santoro-D'Angelo, L, et al. Nicotine induces platelet-derived growth factor release and cytoskeletal alteration in aortic smooth muscle cells. Surgery 2000; 127: 72-78.
27. Wu, J and Lukas, RJ. Naturally-expressed nicotinic acetylcholine receptor subtypes. Biochem Pharmacol 2011; 82: 800-807.
44. Cucina, A, Sapienza, P, Corvino, V, Borrelli, V, Mariani, V, Randone, B, et al. Nicotine-induced smooth muscle cell proliferation is mediated through bFGF and TGF-beta 1. Surgery 2000; 127: 316-322.
28. Castro, NG and Albuquerque, EX. alpha-Bungarotoxin-sensitive hippocampal nicotinic receptor channel has a high calcium permeability. Biophys J 1995; 68: 516-524. 29. Grando, SA, Horton, RM, Pereira, EF, Diethelm-Okita, BM, George, PM, Albuquerque, EX, et al. A nicotinic acetylcholine receptor regulating cell adhesion and motility is expressed in
45. Carty, CS, Soloway, PD, Kayastha, S, Bauer, J, Marsan, B, Ricotta, JJ, et al. Nicotine and cotinine stimulate secretion of basic fibroblast growth factor and affect expression of matrix metalloproteinases in cultured human smooth muscle cells. J Vasc Surg 1996; 24: 927-934; discussion 934-925.
Page 10 of 13
Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295; © 2016 by Mohammed Siddiqui, et al. http://www.smartscitech.com/index.php/nt 46. Zhou, MS, Chadipiralla, K, Mendez, AJ, Jaimes, EA, Silverstein, RL, Webster, K, et al. Nicotine potentiates proatherogenic effects of oxLDL by stimulating and upregulating macrophage CD36 signaling. Am J Physiol Heart Circ Physiol 2013; 305: H563-574.
other nicotine treatments. Clin Pharmacokinet 2001; 40: 661-684. 61. Jaimes, EA, Galceran, JM and Raij, L. Angiotensin II induces superoxide anion production by mesangial cells. Kidney Int 1998; 54: 775-784.
47. Roman, J, Ritzenthaler, JD, Gil-Acosta, A, Rivera, HN and Roser-Page, S. Nicotine and fibronectin expression in lung fibroblasts: implications for tobacco-related lung tissue remodeling. Faseb j 2004; 18: 1436-1438.
62. Sharma, P, Evans, AT, Parker, PJ and Evans, FJ. NADPH-oxidase activation by protein kinase C-isotypes. Biochem Biophys Res Commun 1991; 177: 1033-1040.
48. Arredondo, J, Hall, LL, Ndoye, A, Nguyen, VT, Chernyavsky, AI, Bercovich, D, et al. Central role of fibroblast alpha3 nicotinic acetylcholine receptor in mediating cutaneous effects of nicotine. Lab Invest 2003; 83: 207-225.
63. Sano, M, Fukuda, K, Sato, T, Kawaguchi, H, Suematsu, M, Matsuda, S, et al. ERK and p38 MAPK, but not NF-kappaB, are critically involved in reactive oxygen species-mediated induction of IL-6 by angiotensin II in cardiac fibroblasts. Circ Res 2001; 89: 661-669.
49. Dasgupta, P, Rastogi, S, Pillai, S, Ordonez-Ercan, D, Morris, M, Haura, E, et al. Nicotine induces cell proliferation by beta-arrestin-mediated activation of Src and Rb-Raf-1 pathways. J Clin Invest 2006; 116: 2208-2217.
64. Tian, W, Zhang, Z and Cohen, DM. MAPK signaling and the kidney. Am J Physiol Renal Physiol 2000; 279: F593-604.
50. Zhang, S, Day, I and Ye, S. Nicotine induced changes in gene expression by human coronary artery endothelial cells. Atherosclerosis 2001; 154: 277-283. 51. Razani-Boroujerdi, S, Boyd, RT, Davila-Garcia, MI, Nandi, JS, Mishra, NC, Singh, SP, et al. T cells express alpha7-nicotinic acetylcholine receptor subunits that require a functional TCR and leukocyte-specific protein tyrosine kinase for nicotine-induced Ca2+ response. J Immunol 2007; 179: 2889-2898. 52. Charpantier, E, Wiesner, A, Huh, KH, Ogier, R, Hoda, JC, Allaman, G, et al. Alpha7 neuronal nicotinic acetylcholine receptors are negatively regulated by tyrosine phosphorylation and Src-family kinases. J Neurosci 2005; 25: 9836-9849. 53. Rezonzew, G, Chumley, P, Feng, W, Hua, P, Siegal, GP and Jaimes, EA. Nicotine exposure and the progression of chronic kidney disease: role of the alpha7-nicotinic acetylcholine receptor. Am J Physiol Renal Physiol 2012; 303: F304-312. 54. Graham, A, Court, JA, Martin-Ruiz, CM, Jaros, E, Perry, R, Volsen, SG, et al. Immunohistochemical localisation of nicotinic acetylcholine receptor subunits in human cerebellum. Neuroscience 2002; 113: 493-507. 55. Tain, YL, Freshour, G, Dikalova, A, Griendling, K and Baylis, C. Vitamin E reduces glomerulosclerosis, restores renal neuronal NOS, and suppresses oxidative stress in the 5/6 nephrectomized rat. Am J Physiol Renal Physiol 2007; 292: F1404-1410. 56. Shimamura, T and Morrison, AB. A progressive glomerulosclerosis occurring in partial five-sixths nephrectomized rats. Am J Pathol 1975; 79: 95-106. 57. Heinrich, J, Holscher, B, Seiwert, M, Carty, CL, Merkel, G and Schulz, C. Nicotine and cotinine in adults' urine: The German Environmental Survey 1998. J Expo Anal Environ Epidemiol 2005; 15: 74-80. 58. Ziyadeh, FN, Hoffman, BB, Han, DC, Iglesias-De La Cruz, MC, Hong, SW, Isono, M, et al. Long-term prevention of renal insufficiency, excess matrix gene expression, and glomerular mesangial matrix expansion by treatment with monoclonal antitransforming growth factor-beta antibody in db/db diabetic mice. Proc Natl Acad Sci U S A 2000; 97: 8015-8020.
65. Choudhury, GG, Karamitsos, C, Hernandez, J, Gentilini, A, Bardgette, J and Abboud, HE. PI-3-kinase and MAPK regulate mesangial cell proliferation and migration in response to PDGF. Am J Physiol 1997; 273: F931-938. 66. Hartsough, MT and Mulder, KM. Transforming growth factor beta activation of p44mapk in proliferating cultures of epithelial cells. J Biol Chem 1995; 270: 7117-7124. 67. Hua, P, Feng, W, Ji, S, Raij, L and Jaimes, EA. Nicotine worsens the severity of nephropathy in diabetic mice: implications for the progression of kidney disease in smokers. Am J Physiol Renal Physiol 2010; 299: F732-739. 68. Jaimes, EA, Tian, RX, Joshi, MS and Raij, L. Nicotine augments glomerular injury in a rat model of acute nephritis. Am J Nephrol 2009; 29: 319-326. 69. Wang, JL, Cheng, HF, Shappell, S and Harris, RC. A selective cyclooxygenase-2 inhibitor decreases proteinuria and retards progressive renal injury in rats. Kidney Int 2000; 57: 2334-2342. 70. Jaimes, EA, Tian, RX, Pearse, D and Raij, L. Up-regulation of glomerular COX-2 by angiotensin II: role of reactive oxygen species. Kidney Int 2005; 68: 2143-2153. 71. Wei, Y, Sowers, JR, Clark, SE, Li, W, Ferrario, CM and Stump, CS. Angiotensin II-induced skeletal muscle insulin resistance mediated by NF-kappaB activation via NADPH oxidase. Am J Physiol Endocrinol Metab 2008; 294: E345-351. 72. Arany, I, Grifoni, S, Clark, JS, Csongradi, E, Maric, C and Juncos, LA. Chronic nicotine exposure exacerbates acute renal ischemic injury. Am J Physiol Renal Physiol 2011; 301: F125-133. 73. Arany, I, Reed, DK, Grifoni, SC, Chandrashekar, K, Booz, GW and Juncos, LA. A novel U-STAT3-dependent mechanism mediates the deleterious effects of chronic nicotine exposure on renal injury. Am J Physiol Renal Physiol 2012; 302: F722-729. 74. Hukkanen, J, Jacob, P, 3rd and Benowitz, NL. Metabolism and disposition kinetics of nicotine. Pharmacol Rev 2005; 57: 79-115. 75. Wang, H, Yu, M, Ochani, M, Amella, CA, Tanovic, M, Susarla, S, et al. Nicotinic acetylcholine receptor alpha7 subunit is an essential regulator of inflammation. Nature 2003; 421: 384-388.
59. Eddy, AA. Molecular basis of renal fibrosis. Pediatr Nephrol 2000; 15: 290-301.
76. Yeboah, MM, Xue, X, Duan, B, Ochani, M, Tracey, KJ, Susin, M, et al. Cholinergic agonists attenuate renal ischemia-reperfusion injury in rats. Kidney Int 2008; 74: 62-69.
60. Schneider, NG, Olmstead, RE, Franzon, MA and Lunell, E. The nicotine inhaler: clinical pharmacokinetics and comparison with
77. Yeboah, MM, Xue, X, Javdan, M, Susin, M and Metz, CN. Nicotinic acetylcholine receptor expression and regulation in the
Page 11 of 13
Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295; © 2016 by Mohammed Siddiqui, et al. http://www.smartscitech.com/index.php/nt rat kidney after ischemia-reperfusion injury. Am J Physiol Renal Physiol 2008; 295: F654-661. 78. Sadlier, DM, Ouyang, X, McMahon, B, Mu, W, Ohashi, R, Rodgers, K, et al. Microarray and bioinformatic detection of novel and established genes expressed in experimental anti-Thy1 nephritis. Kidney Int 2005; 68: 2542-2561. 79. Hayashi, K, Osada, S, Shofuda, K, Horikoshi, S, Shirato, I and Tomino, Y. Enhanced expression of membrane type-1 matrix metalloproteinase in mesangial proliferative glomerulonephritis. J Am Soc Nephrol 1998; 9: 2262-2271. 80. Hirose, S, Yamamoto, T, Feng, L, Yaoita, E, Kawasaki, K, Goto, S, et al. Expression and localization of cyclooxygenase isoforms and cytosolic phospholipase A2 in anti-Thy-1 glomerulonephritis. J Am Soc Nephrol 1998; 9: 408-416. 81. Jerde, TJ, Mellon, WS, Bjorling, DE and Nakada, SY. Evaluation of urothelial stretch-induced cyclooxygenase-2 expression in novel human cell culture and porcine in vivo ureteral obstruction models. J Pharmacol Exp Ther 2006; 317: 965-972. 82. Norregaard, R, Jensen, BL, Topcu, SO, Nielsen, SS, Walter, S, Djurhuus, JC, et al. Cyclooxygenase type 2 is increased in obstructed rat and human ureter and contributes to pelvic pressure increase after obstruction. Kidney Int 2006; 70: 872-881. 83. Bagi, Z, Erdei, N, Papp, Z, Edes, I and Koller, A. Up-regulation of vascular cyclooxygenase-2 in diabetes mellitus. Pharmacol Rep 2006; 58 Suppl: 52-56. 84. Kellogg, AP, Cheng, HT and Pop-Busui, R. Cyclooxygenase-2 pathway as a potential therapeutic target in diabetic peripheral neuropathy. Curr Drug Targets 2008; 9: 68-76. 85. Solari, V, Piotrowska, AP, Cascio, S, Unemoto, K, Chertin, B and Puri, P. Cyclooxygenase-2 up-regulation in reflux nephropathy. J Urol 2003; 170: 1624-1627. 86. Tokuyama, H, Hayashi, K, Matsuda, H, Kubota, E, Honda, M, Okubo, K, et al. Differential regulation of elevated renal angiotensin II in chronic renal ischemia. Hypertension 2002; 40: 34-40. 87. Agarwal, PK, van den Born, J, van Goor, H, Navis, G, Gans, RO and Bakker, SJ. Renoprotective effects of long-term oral nicotine in a rat model of spontaneous proteinuria. Am J Physiol Renal Physiol 2012; 302: F895-904. 88. Macconi, D, Bonomelli, M, Benigni, A, Plati, T, Sangalli, F, Longaretti, L, et al. Pathophysiologic implications of reduced podocyte number in a rat model of progressive glomerular injury. Am J Pathol 2006; 168: 42-54. 89. Schulz, A, Schutten-Faber, S, van Es, N, Unland, J, Schulte, L, Kossmehl, P, et al. Induction of albuminuria and kidney damage in SHR by transfer of chromosome 8 from Munich Wistar Fromter rats. Physiol Genomics 2012; 44: 110-116.
db/db mice. Cell 1996; 84: 491-495. 93. Lee, GH, Proenca, R, Montez, JM, Carroll, KM, Darvishzadeh, JG, Lee, JI, et al. Abnormal splicing of the leptin receptor in diabetic mice. Nature 1996; 379: 632-635. 94. Asaba, K, Tojo, A, Onozato, ML, Goto, A, Quinn, MT, Fujita, T, et al. Effects of NADPH oxidase inhibitor in diabetic nephropathy. Kidney Int 2005; 67: 1890-1898. 95. Gorin, Y, Block, K, Hernandez, J, Bhandari, B, Wagner, B, Barnes, JL, et al. Nox4 NAD(P)H oxidase mediates hypertrophy and fibronectin expression in the diabetic kidney. J Biol Chem 2005; 280: 39616-39626. 96. Muhlhauser, I, Sawicki, P and Berger, M. Cigarette-smoking as a risk factor for macroproteinuria and proliferative retinopathy in type 1 (insulin-dependent) diabetes. Diabetologia 1986; 29: 500-502. 97. Metcalfe, W. How does early chronic kidney disease progress? A background paper prepared for the UK Consensus Conference on early chronic kidney disease. Nephrol Dial Transplant 2007; 22 Suppl 9: ix26-30. 98. Gambaro, G, Verlato, F, Budakovic, A, Casara, D, Saladini, G, Del Prete, D, et al. Renal impairment in chronic cigarette smokers. J Am Soc Nephrol 1998; 9: 562-567. 99. Hallan, S, de Mutsert, R, Carlsen, S, Dekker, FW, Aasarod, K and Holmen, J. Obesity, smoking, and physical inactivity as risk factors for CKD: are men more vulnerable? Am J Kidney Dis 2006; 47: 396-405. 100. Briganti, EM, Branley, P, Chadban, SJ, Shaw, JE, McNeil, JJ, Welborn, TA, et al. Smoking is associated with renal impairment and proteinuria in the normal population: the AusDiab kidney study. Australian Diabetes, Obesity and Lifestyle Study. Am J Kidney Dis 2002; 40: 704-712. 101. Orth, SR, Stockmann, A, Conradt, C, Ritz, E, Ferro, M, Kreusser, W, et al. Smoking as a risk factor for end-stage renal failure in men with primary renal disease. Kidney Int 1998; 54: 926-931. 102. Stengel, B, Couchoud, C, Cenee, S and Hemon, D. Age, blood pressure and smoking effects on chronic renal failure in primary glomerular nephropathies. Kidney Int 2000; 57: 2519-2526. 103. Tohidi, M, Hasheminia, M, Mohebi, R, Khalili, D, Hosseinpanah, F, Yazdani, B, et al. Incidence of chronic kidney disease and its risk factors, results of over 10 year follow up in an Iranian cohort. PLoS One 2012; 7: e45304. 104. Gerstein, HC, Mann, JF, Pogue, J, Dinneen, SF, Halle, JP, Hoogwerf, B, et al. Prevalence and determinants of microalbuminuria in high-risk diabetic and nondiabetic patients in the Heart Outcomes Prevention Evaluation Study. The HOPE Study Investigators. Diabetes Care 2000; 23 Suppl 2: B35-39.
90. Obert, DM, Hua, P, Pilkerton, ME, Feng, W and Jaimes, EA. Environmental tobacco smoke furthers progression of diabetic nephropathy. Am J Med Sci 2011; 341: 126-130.
105. Lash, JP, Go, AS, Appel, LJ, He, J, Ojo, A, Rahman, M, et al. Chronic Renal Insufficiency Cohort (CRIC) Study: baseline characteristics and associations with kidney function. Clin J Am Soc Nephrol 2009; 4: 1302-1311.
91. Sharma, K, McCue, P and Dunn, SR. Diabetic kidney disease in the db/db mouse. Am J Physiol Renal Physiol 2003; 284: F1138-1144.
106. Garcia-Esquinas, E, Loeffler, LF, Weaver, VM, Fadrowski, JJ and Navas-Acien, A. Kidney function and tobacco smoke exposure in US adolescents. Pediatrics 2013; 131: e1415-1423.
92. Chen, H, Charlat, O, Tartaglia, LA, Woolf, EA, Weng, X, Ellis, SJ, et al. Evidence that the diabetes gene encodes the leptin receptor: identification of a mutation in the leptin receptor gene in
107. Andronico, G, Rome, M, Lo Cicero, A, Parsi, R, Seddio, G, Ferraro-Mortellaro, R, et al. Renal plasma flow, filtration fraction and microalbuminuria in hypertensive patients: effects of chronic
Page 12 of 13
Neurotransmitter 2016; 3: e1295. doi: 10.14800/nt.1295; © 2016 by Mohammed Siddiqui, et al. http://www.smartscitech.com/index.php/nt smoking. Nephrology (Carlton) 2005; 10: 483-486.
II diabetes. Am J Kidney Dis 1995; 25: 836-844.
108. Mimran, A, Ribstein, J, DuCailar, G and Halimi, JM. Albuminuria in normals and essential hypertension. J Diabetes Complications 1994; 8: 150-156. 109. Horner, D, Fliser, D, Klimm, HP and Ritz, E. Albuminuria in normotensive and hypertensive individuals attending offices of general practitioners. J Hypertens 1996; 14: 655-660. 110. Orth, SR. Effects of smoking on systemic and intrarenal hemodynamics: influence on renal function. J Am Soc Nephrol 2004; 15 Suppl 1: S58-63. 111. Halimi, JM, Giraudeau, B, Vol, S, Caces, E, Nivet, H and Tichet, J. The risk of hypertension in men: direct and indirect effects of chronic smoking. J Hypertens 2002; 20: 187-193. 112. Mann, SJ, James, GD, Wang, RS and Pickering, TG. Elevation of ambulatory systolic blood pressure in hypertensive smokers. A case-control study. JAMA 1991; 265: 2226-2228. 113. Grassi, G, Seravalle, G, Calhoun, DA, Bolla, GB, Giannattasio, C, Marabini, M, et al. Mechanisms responsible for sympathetic activation by cigarette smoking in humans. Circulation 1994; 90: 248-253. 114. Benck, U, Clorius, JH, Zuna, I and Ritz, E. Renal hemodynamic changes during smoking: effects of adrenoreceptor blockade. Eur J Clin Invest 1999; 29: 1010-1018. 115. Orth, SR. Smoking--a renal risk factor. Nephron 2000; 86: 12-26. 116. Orth, SR. Smoking and the kidney. J Am Soc Nephrol 2002; 13: 1663-1672. 117. Chuahirun, T, Khanna, A, Kimball, K and Wesson, DE. Cigarette smoking and increased urine albumin excretion are interrelated predictors of nephropathy progression in type 2 diabetes. Am J Kidney Dis 2003; 41: 13-21. 118. Chase, HP, Garg, SK, Marshall, G, Berg, CL, Harris, S, Jackson, WE, et al. Cigarette smoking increases the risk of albuminuria among subjects with type I diabetes. JAMA 1991; 265: 614-617. 119. Chaturvedi, N, Stephenson, JM and Fuller, JH. The relationship between smoking and microvascular complications in the EURODIAB IDDM Complications Study. Diabetes Care 1995; 18: 785-792. 120. Savage, S, Nagel, NJ, Estacio, RO, Lukken, N and Schrier, RW. Clinical factors associated with urinary albumin excretion in type
121. Vergouwe, Y, Soedamah-Muthu, SS, Zgibor, J, Chaturvedi, N, Forsblom, C, Snell-Bergeon, JK, et al. Progression to microalbuminuria in type 1 diabetes: development and validation of a prediction rule. Diabetologia 2010; 53: 254-262. 122. Phisitkul, K, Hegazy, K, Chuahirun, T, Hudson, C, Simoni, J, Rajab, H, et al. Continued smoking exacerbates but cessation ameliorates progression of early type 2 diabetic nephropathy. Am J Med Sci 2008; 335: 284-291. 123. Sawicki, PT, Didjurgeit, U, Muhlhauser, I, Bender, R, Heinemann, L and Berger, M. Smoking is associated with progression of diabetic nephropathy. Diabetes Care 1994; 17: 126-131. 124. Biesenbach, G, Grafinger, P, Janko, O and Zazgornik, J. Influence of cigarette-smoking on the progression of clinical diabetic nephropathy in type 2 diabetic patients. Clin Nephrol 1997; 48: 146-150. 125. Agarwal, R. Smoking, oxidative stress and inflammation: impact on resting energy expenditure in diabetic nephropathy. BMC Nephrol 2005; 6: 13. 126. Ward, MM and Studenski, S. Clinical prognostic factors in lupus nephritis. The importance of hypertension and smoking. Arch Intern Med 1992; 152: 2082-2088. 127. Chapman, AB, Johnson, AM, Gabow, PA and Schrier, RW. Overt proteinuria and microalbuminuria in autosomal dominant polycystic kidney disease. J Am Soc Nephrol 1994; 5: 1349-1354. 128. Ozkok, A, Akpinar, TS, Tufan, F, Kanitez, NA, Uysal, M, Guzel, M, et al. Clinical characteristics and predictors of progression of chronic kidney disease in autosomal dominant polycystic kidney disease: a single center experience. Clin Exp Nephrol 2013; 17: 345-351. 129. Cardinal, H, Hebert, MJ, Rahme, E, Houde, I, Baran, D, Masse, M, et al. Modifiable factors predicting patient survival in elderly kidney transplant recipients. Kidney Int 2005; 68: 345-351. 130. Sung, RS, Althoen, M, Howell, TA, Ojo, AO and Merion, RM. Excess risk of renal allograft loss associated with cigarette smoking. Transplantation 2001; 71: 1752-1757. 131. Lin, SJ, Koford, JK, Baird, BC, Hurdle, JF, Krikov, S, Habib, AN, et al. Effect of donors' intravenous drug use, cigarette smoking, and alcohol dependence on kidney transplant outcome. Transplantation 2005; 80: 482-486.
Page 13 of 13