1417
Predictive Modeling for the Presence of Prostate Carcinoma using Clinical, Laboratory, and Ultrasound Parameters in Patients with Prostate Specific Antigen Levels < 10 ng/mL Mark Garzotto, M.D.1,2 R. Guy Hudson, M.D1,2 Laura Peters, R.N.1 Yi-Ching Hsieh, M.S.3 Eduardo Barrera, M.D.1 Motomi Mori, Ph.D.3 Tomasz M. Beer, M.D.4 Thomas Klein, M.D.1,2 1
Division of Urology, Portland Veterans Administration Medical Center, Portland, Oregon.
2
Divison of Urology, Oregon Health and Science University, Portland, Oregon.
3
Biostatistics and Bioinformatics Shared Resource, Oregon Health and Science University Cancer Institute, Portland, Oregon.
4
Division of Hematology and Medical Oncology, Oregon Health and Science University, Portland, Oregon.
Supported by a Veterans Administration Career Development Award (M. G.) and by National Institutes of Health grant P30 CA 69533 to the Biostatistics and Bioinformatics Shared Resource of the Oregon Health and Science University Cancer Institute (Portland, Oregon). Address for reprints: Mark Garzotto, M.D., Urology Section, Portland Veterans Administration Medical Center, 3710 S.W. US Veterans Hospital Road, Portland, OR 97239; Fax: (503) 220-3415; E-mail:
[email protected] Received April 3, 2003; revision received June 16, 2003; accepted July 3, 2003. © 2003 American Cancer Society DOI 10.1002/cncr.11668
BACKGROUND. The objective of the current study was to develop a model for predicting the presence of prostate carcinoma using clinical, laboratory, and transrectal ultrasound (TRUS) data. METHODS. Data were collected on 1237 referred men with serum prostate specific antigen (PSA) levels ⱕ 10 ng/mL who underwent an initial prostate biopsy. Variables analyzed included age, race, family history, referral indication(s), prior vasectomy, digital rectal examination (DRE), PSA level, PSA density (PSAD), and TRUS findings. Twenty percent of the data were reserved randomly for study validation. Logistic regression analysis was performed to estimate the relative risk, 95% confidence interval, and P values. RESULTS. Independent predictors of a positive biopsy result included elevated PSAD, abnormal DRE, hypoechoic TRUS finding, and age 75 years or older. Based on these variables, a predictive nomogram was developed. The sensitivity and specificity of the model were 92% and 24%, respectively, in the validation study for which the predictive probability ⱖ 10% was used to indicate the presence of prostate carcinoma. The area under the receiver operating characteristic curve (AUC) for the model was 73%, which was significantly higher compared with the prediction based on PSA alone (AUC, 62%). If it was validated externally, then application of this model to the biopsy decision could result in a 24% reduction in unnecessary biopsy procedures, with an overall reduction of 20%. CONCLUSIONS. Incorporation of clinical, laboratory, and TRUS data into a prebiopsy nomogram significantly improved the prediction of prostate carcinoma over the use of individual factors alone. Predictive nomograms may serve as an aid to patient counseling regarding prostate biopsy outcome and to reduce the number of unnecessary biopsy procedures. Cancer 2003;98:1417–22. © 2003 American Cancer Society. KEYWORDS: prostate carcinoma, detection, prediction, nomogram.
A
denocarcinoma of the prostate is the most common malignancy in men and is the second leading cause of male cancer mortality in the U.S.1 In the absence of clinical trial data demonstrating a benefit, the practice of screening for the presence of disease remains controversial. A recent trend toward decreased prostate carcinoma deaths in the U.S. (that has not been observed in the U.K., where prostate carcinoma screening is not recommended routinely) may indicate that early detection and intervention are effective.2 Furthermore, a recent report from a randomized trial that compared observation with surgery showed an improvement in metastases free and
1418
CANCER October 1, 2003 / Volume 98 / Number 7
prostate carcinoma specific survival in the prostatectomy arm.3 Randomized trials designed to examine the effect of prostate screening currently are underway in Europe and the U.S.4,5 Approximately 10% of men are found to have an elevated total prostate specific antigen (PSA) level at initial prostate screening.4,6 The PSA value is considered unequivocally abnormal above 10.0 ng/mL, because the incidence of a positive prostate biopsy is ⬎ 50% at that level.6 However, in the intermediate PSA range (4.1–10.0 ng/mL), the positive biopsy rate is 25%; thus, the majority of these patients have PSA elevations due to benign disease.7 In the intermediate range, PSA alone lacks the specificity needed to allow for making informed choices regarding the appropriateness of a full evaluation for prostate carcinoma. In addition to total PSA, other factors that have been associated with the detection of prostate carcinoma include age, race, family history, abnormal digital rectal examination (DRE), hypoechoic lesions on transrectal ultrasound (TRUS), PSA density (PSAD), PSA velocity, transition zone PSAD, and the percentage of free PSA (fPSA).8 With the exception of the percent of fPSA, these individual factors have limited predictive value and, thus, are not used routinely to estimate the risk of a positive biopsy in the course of counseling patients. Clearly, tools that could accurately predict the presence of cancer significantly could reduce the number of unnecessary biopsies and their accompanying pain and morbidity.9 Several groups have sought to develop models to aid in the prediction of a positive prostate biopsy in men who are being evaluated for prostate carcinoma.8,10 –12 Those studies demonstrated the capacity of either artificial neural networks or logistic regression to improve the accuracy of the prediction of prostate carcinoma over individual factors alone. The clinical utility of these models has been limited due to an inability to identify low-risk groups that could avoid undergoing prostate biopsies (for review, see Ohori and Swindle13). More recently, Djavan et al. developed an artificial neural network that utilizes multiple variables, including ultrasound data, to determine the risk of a positive biopsy with improved predictive capacity.14 The objective of this study was to develop a predictive model for the biopsy detection of prostate carcinoma in a referred population with serum PSA levels ⱕ 10 ng/mL by incorporating clinical, laboratory, and ultrasound data. In this study, significant independent covariates for the detection of carcinoma were PSAD, DRE, hypoechoic TRUS lesions, and patient age. Using these risk factors, a nomogram was constructed that was capable of providing more precise risk-analysis information for the individual patient. This model of-
fers a robust tool that potentially may improve the prediction of prostate carcinoma over individual factors.
MATERIALS AND METHODS Population Between February 1993 and October 2000, data were collected prospectively and uniformly for the purposes of clinical care on 1635 referred patients who underwent a TRUS with prostate biopsy at the Portland Veterans Administration Hospital. Within this group, 1239 patients presented with an initial serum PSA level ⱕ 10 ng/mL and had a minimum of 6 biopsy cores obtained. At the time of presentation, the serum PSA was repeated with a microparticle enzyme immunoassay (Abbott Diagnostic Laboratories, Abbott Park, IL). A member of the urology team performed a DRE on all patients prior to the TRUS. The DRE was classified as normal, asymmetric, suspicious, or cancerlikely. Any prostatic nodule or induration was considered a suspicious finding on DRE. Evidence of extraprostatic extension and/or a rock-hard prostate was classified as cancer-likely. Those who underwent prior TRUS-guided biopsy of the prostate, had evidence of a urinary tract infection, and those with biopsies of ⬍ 6 cores or a PSA level ⬎ 10 ng/mL were excluded from this analysis. This study was approved by the Portland Veterans Administration Institutional Review Board and was exempted from informed consent.
TRUS and Biopsy Procedure Prior to TRUS, a cleansing rectal enema and prophylactic antibiotics were administered. A Bruel and Kjær system 3535 ultrasound device (Marlboro, MA) with a model 8551 7.0-MHz probe was used to obtain ultrasound data. The prostate was measured in 3 dimensions, and prostate volume was estimated using a modification of the prolate ellipsoid formula and recorded in cm3 (0.52[length (cm) ⫻ width (cm) ⫻ height (cm)]). The PSAD was calculated by dividing the serum PSA by the calculated prostate volume. At the same setting, all patients underwent ultrasoundguided prostate biopsies that were performed using the Biopty威 spring-loaded, 18-gauge biopsy instrument (Bard, Covington, GA). A minimum of six cores was obtained from each study patient with additional cores, when indicated, sampled from suspicious areas. The biopsy specimens were examined for the presence of adenocarcinoma and were categorized by Gleason score.
Predictive Model for Prostate Carcinoma/Garzotto et al.
Statistical Analysis The primary endpoint of the study was the detection of prostate carcinoma in the biopsy material. We randomly selected 80% of patients for model building and reserved the remaining 20% of patients for model validation. Thus, the model was built containing data from 976 men (231 men with positive biopsy results and 745 men with negative biopsy results). Factors that were evaluated for the risk of a positive biopsy included: age, race, family history, indication(s) for referral, prior vasectomy, DRE findings, hypoechoic lesions, PSA, PSAD, and prostate volume. PSA, PSAD, age, and prostate volume were analyzed as categorical variables with the following categories: age (younger than 65 years, 65– 69 years, 70 –74 years, or 75 years and older), serum PSA (⬍ 3.0 ng/mL, 3.0 –5.0 ng/mL, 5.1–7.0 ng/mL, or 7.1–10.0 ng/mL), volume (⬍ 24.1 cm3, 24.1–34.25 cm3, 34.26 – 47.80 cm3, or ⬎ 47.8 cm3), and PSAD (⬍ 0.09 ng/mL/cc, 0.09 – 0.15 ng/mL/cc, 0.16 – 0.27 ng/mL/cc, or ⬎ 0.27 ng/mL/cc). The selected categories represent either commonly used groupings or quartiles of the distribution. The significance of each factor was assessed by univariate logistic regression analyses. Multivariate logistic regression analysis, specifically, stepwise logistic regression, was used to determine which factors were independent predictors of prostate carcinoma in the model-building set. Relative risks (RR) and 95% confidence intervals (95% CIs) also were derived. A nomogram for positive biopsy was developed based on the final logistic regression model. Using the validation data set, the receiver operating characteristics (ROC) curve was used to measure the model’s performance compared with the prediction based on PSA alone. Based on the ROC curve, we selected the cut-off value for the predicted probability of prostate cancer. The selected cutoff value provides a high sensitivity at the same time reducing the total number of unnecessary biopsies. Logistic regression analyses were performed using Statistical Analysis System (SAS) software (SAS, Inc., Cary, NC), and the ROC analysis was performed using LABROC1 software.15
1419
TABLE 1 Patient Demographics in the Biopsy Cohort (n ⴝ 1239 men) Variable Age (%) ⬍ 65 yrs 65–69 yrs 70–74 yrs ⱖ 75 yrs Race (%) White African American Other Positive family history (%) Prior vasectomy (%) Serum prostate specific antigen Mean Median Distribution (%) ⬍ 3.0 ng/mL 3.0–5.0 ng/mL 5.1–7.0 ng/mL 7.1–10.0 ng/mL Digital rectal examination (%) Normal Asymmetric only Suspicious Cancer likely
Value
40.7 25.3 25.0 9.0 93.5 4.2 2.3 16.9 33.1 4.93 ng/mL 5.10 ng/mL 27.6 21.2 27.5 23.7 49.0 5.7 41.9 3.4
Ultrasound Findings A hypoechoic lesion was detected in 47.7% of patients. The median prostate volume was 32.4 cm3. The median PSAD was 0.12 ng/mL/cm3.
Biopsy Results A minimum of 6 cores was obtained from all patients during the procedure (mean, 6.7 cores; range, 6 –13 cores). Adenocarcinoma of the prostate was detected on biopsy in 24.3% of men (300 of 1239 patients). In the 300 patients with carcinoma, Gleason scores were classified as 2– 4 in 4.1% of positive biopsies, 5 in 19.1% of positive biopsies, 6 in 48.5% of positive biopsies, 7 in 21.2% of positive biopsies, and 8 –10 in 7.2% of positive biopsies.
RESULTS
Development of Predictive Model
Patient Data
In the univariate logistic regression analysis, significant predictors for a positive prostate biopsy in the order of statistical significance were: hypoechoic lesion (P ⬍ 0.0001), cancer-likely DRE (P ⬍ 0.0001), PSA and DRE referral (P ⬍ 0.0001), PSA (3–5 ng/mL, P ⫽ 0.0001; 5.1–7.0 ng/mL, P ⬍ 0.0001; 7.1–10.0 ng/mL, P ⬍ 0.0001), PSAD (0.09 – 0.15 ng/mL/cc, P ⫽ 0.0007; 0.16 – 0.27 ng/mL/cc, P ⬍ 0.0001; ⬎ 0.27 ng/mL/cc, P ⬍ 0.0001), prostate volume ⬎ 47.8 (P ⫽ 0.0005), PSA alone referral (P ⫽ 0.0013), age 75 years and older (P
Characteristics of the study population are shown in Table 1. The median age was 66.0 years. Race was classified as white in 93.5% of patients and African American in 4.2% of patients. Family history for prostate carcinoma in a first-degree relative was present in 16.9% of patients. A history of vasectomy was noted in 33.1% of patients. The median serum PSA level was 5.1 ng/mL. The DRE was classified as suspicious or carcinoma-likely in 45.3% of men (Table 1).
1420
CANCER October 1, 2003 / Volume 98 / Number 7
TABLE 2 Results of a Stepwise Multivariate Analysis Evaluating the Risk of a Positive Biopsy Risk factor/finding DRE Suspicious Cancer likely TRUS Hyperechoic PSAD (ng/mL/cc) ⬍ 0.09 0.09–0.15 0.16–0.27 ⬎ 0.27 Age ⱖ 75 yrs
RR
95% CI
P value
1.63 6.44
1.15–2.30 2.83–14.7
0.0061 ⬍ 0.0001
1.61
1.15–2.26
0.0058
1.00 2.41 5.83 11.4 1.84
— 1.44–4.02 3.55–9.58 6.42–20.13 1.10–3.08
— 0.0008 ⬍ 0.0001 ⬍ 0.0001 0.0213
RR: relative risk; 95% CI: 95% confidence interval; DRE: digital rectal examination; TRUS: transrectal ultrasound; PSAD: prostate specific antigen density.
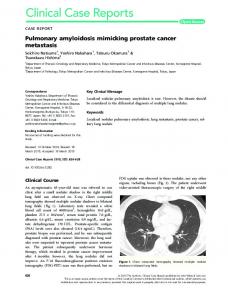
⫽ 0.0041), and suspicious DRE (P ⫽ 0.0227). Factors that were not found significant were family history, prostate asymmetry, race, and prior vasectomy. In the stepwise multivariate logistic regression analysis, significant predictors for the detection of prostate carcinoma in the study cohort, in the order of their statistical significance, were PSAD ⬎ 0.27 ng/ mL/cc, carcinoma-likely DRE, PSAD 0.16 – 0.27 ng/ mL/cc, PSAD 0.09 – 0.15 ng/mL:/cc, age 75 years and older, suspicious DRE, and hypoechoic lesion on TRUS. In independent analyses, using both forward and backward stepwise procedures yielded identical results. A nomogram was developed based on these results utilizing the four independent risk factors for the diagnosis of prostate carcinoma. For each of the four categories, an individual accumulates a number of points that are totaled to calculate the overall likelihood of a positive biopsy, as described previously.16 For example, a male age 68 years with a PSA of 4.9 ng/mL is found to have a normal DRE, normal TRUS, and a PSAD of 0.08 ng/mL/cc: According to the model, his risk of a positive biopsy would be 5%, not the 25% risk commonly quoted due to a PSA level in the intermediate range (4 –10 ng/mL). In another example, a male age 63 years with a PSA of 7.2 ng/mL, suspicious DRE, a PSAD of 0.30 ng/mL/cc, and a hypoechoic area on TRUS would have a 59% risk of a positive biopsy. Using this model, the possibility for a positive biopsy ranges from 5% to 55% for patients with a PSA level ⱕ 10 ng/mL (Table 2, Fig. 1). The accuracy of the model was determined using the validation set. The ROC curve was used to evaluate the accuracy of the predicted probability from the model compared with the prediction based on total PSA alone (Fig. 2). The area under the curve (AUC) was
FIGURE 1.
Nomogram for the detection of prostate cancer in men with prostate specific antigen (PSA) levels ⱕ10.0 ng/mL. Directions: locate digital rectal examination (DRE), age, transrectal ultrasound (TRUS) finding, and PSA density (PSAD) for the individual patient. Draw a line in the upward direction to find the number of points given in each category. Total these points, then draw a line downward to find the patient’s risk for a positive biopsy. The total score of 6.8 corresponds to 10% likelihood of positive prostate biopsy.
FIGURE 2.
Receiver operating characteristic curve (ROC) comparing the model (using prostate specific antigen [PSA], PSA density, transrectal ultrasound, and age) versus PSA alone for the prediction of prostate carcinoma. AUC: area under the ROC.
73% for the model, in contrast to 62% for the prediction based on PSA alone. If we decide that only those patients with ⱖ 10% predicted probability of prostate carcinoma will undergo a biopsy, a probability that approximates the widely accepted PSA cut-off value of 4.0 ng/mL, then the model will capture 92% of all prostate carcinoma cases (sensitivity) while sparing 24% of patients without prostate carcinoma from undergoing an unnecessary procedure (specificity). Overall, the application of this model would reduce by 20% the total number of biopsies. The performance of
Predictive Model for Prostate Carcinoma/Garzotto et al.
FIGURE 3. Estimated sensitivity, specificity, and percent reduction in biopsies based on the validation data set (n ⫽ 244 patients; 23% prostate carcinoma) as a function of a cut-off point for the predicted probability.
the model at specific cut-off values for the probability of carcinoma is shown in Figure 3.
DISCUSSION Population-based screening shows that 1 in 10 men will be identified with an elevated PSA level at initial presentation.4,6 However, of these men, only 1 in 4 will be identified with carcinoma as a cause, because the majority of intermediate PSA elevations are the result of benign disease. Thus, prostate screening with total PSA is considered a sensitive means of identifying those at risk for a positive prostate biopsy; but it fails to discriminate them from patients with PSA elevations who are not at risk. In an effort to improve the specificity of PSA, several PSA derivatives have been introduced. These include age specific PSA, PSAD, transition-zone PSAD, PSA velocity, and percent of fPSA.8 Nevertheless, with the exception of percent of fPSA, application of these individual factors does not reduce significantly the number of biopsies performed.13 In the current study, we evaluated several biopsy risk factors that are readily available to the practicing urologist. This was a prospective, single-institution cohort of 1239 referred men with a PSA level ⱕ 10 ng/mL who underwent an initial prostate biopsy. Total PSA, as reported previously, was a poor predictor of a positive biopsy result.7,10 Independent factors that were associated with a positive biopsy were elevated PSAD, hypoechoic lesion on TRUS, abnormal DRE, and age 75 years and older. Based on the results of multivariate logistic regression, these factors were then used to generate a predictive model for the diag-
1421
nosis of prostate carcinoma. One of the limitations of several prior models is that they were unable to identify low-risk groups that were at minimal risk of having a positive biopsy result.13 The model presented herein showed that patients younger than age 75 years with a normal DRE, normal TRUS, and a PSAD ⬍ 0.9 ng/ mL/cc had a 5% chance of having a positive biopsy. Others have reported similar rates as acceptable cutoff levels for missed positive biopsies. In patients with a normal DRE and PSA level (⬍ 4.0 ng/mL), prostate carcinoma can be found in 6% to 9% of those biopsied.17,18 Similar rates of missed tumors have been reported with percent of fPSA. Using a percent of fPSA cut-off level of 25% in men with an intermediate PSA level and a normal DRE, the risk of carcinoma on biopsy is 8%.7 One of the objectives of developing a predictive model for the detection of prostate carcinoma is to reduce the number of men requiring prostate biopsies. Using a carcinoma probability cut-off level of 10%, we were able to predict a reduction of the number of unnecessary biopsies by 24% while maintaining a sensitivity of 92%. This result is comparable to results using a percent of fPSA cut-off level of 25%, which has been shown to reduce the number of unnecessary biopsies in men with a normal DRE and intermediate PSA levels by 20%.7 Using a cut-off probability of 18%, Carlson et al. showed that they could reduce the number of biopsies by 34% while maintaining 95% sensitivity.10 Although all of those studies were validated internally, they each will require prospective confirmation with independent data sets before general use can be recommended as an aid to patient counseling. One of the limitations of the current study was the fact that the cohort was comprised predominantly of white men, with only 4.2% African-American men. Prior studies have reported a similar racial disproportion. Catalona et al. reported that 2.9% of participants were African American in a large screening study.6 In the study by Djavan et al., none of the participants were of African descent.14 Only the study by Easthham et al. had a high rate of African-American participants.11 Another potential limitation of the current study includes the use of primarily sextant biopsies, although most of the more recent patients in this study have routinely undergone 10-core sampling. Recent reports have shown a high carcinoma detection rate in patients who had additional cores taken at the time of the procedure.19 However, in a randomized trial, Naughton et al. found that the biopsy-detection rate was similar (27% vs. 26%; P ⫽ nonsignificant) in patients who underwent either 6 biopsies or 12 biopsies.20 Finally, the percent of fPSA was not included in
1422
CANCER October 1, 2003 / Volume 98 / Number 7
the current study, because many participants were evaluated prior to its introduction into clinical practice. Notwithstanding, a recent study demonstrated that percent of fPSA and PSAD were comparable in the predicting the presence of prostate carcinoma.21 Thus, the omission of percent of fPSA may have been overcome by the use of PSAD in the current study. Controversy currently exists regarding the optimal method for development of predictive models in medicine. Two commonly used methods are logistic regression and artificial neural networks. Each is known to have its particular advantages. However, some investigators have cited the problem of over fit with artificial neural networks, in which case, the neural network overpartitions the variables to fit the data set being studied.22 In our cohort of 1239 patients PSAD, abnormal TRUS, abnormal DRE, and age were associated independently with a positive biopsy. These factors were used to construct a model that, at the 10% cut-off level, retained a sensitivity of 92%. When the model was applied to a validation cohort, its application was associated with a 24% reduction in unnecessary biopsies.
REFERENCES 1.
2.
3.
4.
5.
6.
7.
Howe HL, Wingo PA, Thun MJ, et al. Annual report to the nation on the status of cancer (1973 through 1998), featuring cancers with recent increasing trends. J Natl Cancer Inst. 2001;93:824 – 842. Shibata A, Ma J, Whittemore AS. Prostate cancer incidence and mortality in the United States and the United Kingdom. J Natl Cancer Inst. 1998;90:1230 –1231. Holmberg L, Bill-Axelson A, Helgesen F, et al. A randomized trial comparing radical prostatectomy with watchful waiting in early prostate cancer. N Engl J Med. 2002;347:781–789. Schroder FH, van der Cruijsen-Koeter I, de Koning HJ, Vis AN, Hoedemaeker RF, Kranse R. Prostate cancer detection at low prostate specific antigen. J Urol. 2000;163:806 – 812. Prorok PC, Andriole GL, Bresalier RS, et al. Design of the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial. Control Clin Trials. 2000;21:273S–309S. Catalona WJ, Richie JP, Ahmann FR, et al. Comparison of digital rectal examination and serum prostate specific antigen in the early detection of prostate cancer: results of a multicenter clinical trial of 6630 men. J Urol. 1994;151:1283– 1290. Catalona WJ, Partin AW, Slawin KM, et al. Use of the percentage of free prostate-specific antigen to enhance differentiation of prostate cancer from benign prostatic disease: a prospective multicenter clinical trial. JAMA. 1998;279:1542– 1547.
8.
9.
10.
11.
12.
13.
14.
15. 16.
17.
18.
19.
20.
21.
22.
Kamoi K, Babaian RJ. Advances in the application of prostate-specific antigen in the detection of early-stage prostate cancer. Semin Oncol. 1999;26:140 –149. Rodriguez LV, Terris MK. Risks and complications of transrectal ultrasound guided prostate needle biopsy: a prospective study and review of the literature. J Urol. 1998;160:2115– 2120. Carlson GD, Calvanese CB, Partin AW. An algorithm combining age, total prostate-specific antigen (PSA), and percent free PSA to predict prostate cancer: results on 4298 cases. Urology. 1998;52:455– 461. Eastham JA, May R, Robertson JL, Sartor O, Kattan MW. Development of a nomogram that predicts the probability of a positive prostate biopsy in men with an abnormal digital rectal examination and a prostate-specific antigen between 0 and 4 ng/mL. Urology. 1999;54:709 –713. Potter SR, Horniger W, Tinzl M, Bartsch G, Partin AW. Age, prostate-specific antigen, and digital rectal examination as determinants of the probability of having prostate cancer. Urology. 2001;57:1100 –1104. Ohori M, Swindle P. Nomograms and instruments for the initial prostate evaluation: the ability to estimate the likelihood of identifying prostate cancer. Semin Urol Oncol. 2002; 20:116 –122. Djavan B, Remzi M, Zlotta A, Seitz C, Snow P, Marberger M. Novel artificial neural network for early detection of prostate cancer. J Clin Oncol. 2002;20:921–929. Metz C. Software for ROC analysis. Comm Imaging Jpn Soc Radiol Technol. 2000;23:2–9. Kattan MW, Eastham JA, Stapleton AM, Wheeler TM, Scardino PT. A preoperative nomogram for disease recurrence following radical prostatectomy for prostate cancer. J Natl Cancer Inst. 1998;90:766 –771. Cooner WH, Mosley BR, Rutherford CL Jr., et al. Prostate cancer detection in a clinical urological practice by ultrasonography, digital rectal examination and prostate specific antigen. J Urol. 1990;143:1146 –1152; discussion, 1152–1154. Ellis WJ, Chetner MP, Preston SD, Brawer MK. Diagnosis of prostatic carcinoma: the yield of serum prostate specific antigen, digital rectal examination and transrectal ultrasonography. J Urol. 1994;152:1520 –1525. Presti JC Jr., Chang JJ, Bhargava V, Shinohara K. The optimal systematic prostate biopsy scheme should include 8 rather than 6 biopsies: results of a prospective clinical trial. J Urol. 2000;163:163–166; discussion, 166 –167. Naughton CK, Miller DC, Mager DE, Ornstein DK, Catalona WJ. A prospective randomized trial comparing 6 versus 12 prostate biopsy cores: impact on cancer detection. J Urol. 2000;164:388 –392. Catalona WJ, Southwick PC, Slawin KM, et al. Comparison of percent free PSA, PSA density, and age-specific PSA cutoffs for prostate cancer detection and staging. Urology. 2000;56: 255–260. Kattan M. Statistical prediction models, artificial neural networks, and the sophism “I am a patient, not a statistic.” J Clin Oncol. 2002;20:885– 887.