Respiratory Medicine (2015) 109, 671e679
Available online at www.sciencedirect.com
ScienceDirect journal homepage: www.elsevier.com/locate/rmed
REVIEW
Respiratory dysfunction in multiple sclerosis George E. Tzelepis a,b,*, F. Dennis McCool a,b a Department of Pathophysiology and Laiko General Hospital, and University of Athens Medical School, Athens, Greece b Department of Pulmonary and Critical Care Medicine, The Memorial Hospital RI, and The Warren Alpert Medical School of Brown University, Providence, RI, USA
Received 12 May 2014; accepted 19 January 2015
Available online 12 February 2015
KEYWORDS Multiple sclerosis; Respiration; Respiratory failure; Respiratory muscles
Summary Respiratory dysfunction frequently occurs in patients with advanced multiple sclerosis (MS), and may manifest as acute or chronic respiratory failure, disordered control of breathing, respiratory muscle weakness, sleep disordered breathing, or neurogenic pulmonary edema. The underlying pathophysiology is related to demyelinating plaques involving the brain stem or spinal cord. Respiratory complications such as aspiration, lung infections and respiratory failure are typically seen in patients with long-standing MS. Acute respiratory failure is uncommon and due to newly appearing demyelinating plaques extensively involving areas of the brain stem or spinal cord. Early recognition of MS patients at risk for respiratory complications allows for the timely implementation of care and measures to decrease disease associated morbidity and mortality. ª 2015 Elsevier Ltd. All rights reserved.
Contents Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 672 Pathophysiology of respiratory dysfunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 672 Respiratory failure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 672 Respiratory muscle weakness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 673 Impaired cough . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 674 Control of breathing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 674 Sleep-disordered breathing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 674 Neurogenic pulmonary edema . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 675 Identifying patients at risk for respiratory dysfunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 675 * Corresponding author. Department of Pathophysiology, University of Athens Medical School, 75 M. Asias Street, 11527 Athens, Greece. Tel.: þ30 210 746 2649; fax: þ30 210 746 2664. E-mail address:
[email protected] (G.E. Tzelepis). http://dx.doi.org/10.1016/j.rmed.2015.01.018 0954-6111/ª 2015 Elsevier Ltd. All rights reserved.
672
G.E. Tzelepis, F.D. McCool Pulmonary function tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 675 Exercise capacity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 676 Treatment of respiratory complications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 676 General aspects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 676 Respiratory muscle training . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 676 Disclosure of conflicts of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 677 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 677
Introduction Multiple sclerosis (MS) is a chronic central nervous system disorder characterized by multiple areas of nerve demyelination that impair nerve conduction. Its symptoms are either relapsing, remitting or progressive and include muscle weakness, spasticity, impairment of coordination, generalized fatigue, vision loss, and cognitive impairment [1]. The importance of respiratory dysfunction in MS has been recognized only during the last few decades [2]. Unlike neuromuscular diseases that involve the peripheral nerves or muscles intrinsic to the respiratory “pump”, respiratory dysfunction in MS arises only when demyelinating plaques involve distinct brain regions associated with breathing. This may explain the rare occurrence of respiratory dysfunction in the early stages of MS and its relatively higher prevalence in patients with advanced disease. Factors contributing to respiratory dysfunction in MS include weakness of the respiratory muscles, bulbar dysfunction, abnormal ventilatory control, and sleep disordered breathing. Respiratory dysfunction contributes significantly to morbidity and mortality in MS [3]. Respiratory complications are one of the most common causes of death in MS [3e7]. In one large study, respiratory complications accounted for approximately 47% of all deaths in MS patients [8]. Recognizing which patients with MS are at the greatest risk for respiratory complications is critical as it may help the clinician to carefully screen these patients and initiate appropriate preventive measures or care to decrease the associated morbidity and mortality. In the present review we focus on clinical aspects of respiratory dysfunction in MS, paying particular emphasis on respiratory failure and clinically relevant sequelae of respiratory muscle weakness such as sleep fragmentation (desaturation), impaired cough and respiratory infection.
Pathophysiology of respiratory dysfunction The pathophysiological hallmark of respiratory dysfunction in MS is the presence of demyelinating lesions in the central nervous system. These lesions may involve one or more locations associated with production and/or propagation of neural impulses to the respiratory muscles. Depending upon the location and extent of demyelinating lesions, respiratory dysfunction may manifest with symptoms due to respiratory muscle weakness and impaired cough, dysfunction of bulbar muscles, abnormalities in the control of breathing, or respiratory failure (Table 1). Additional factors such
as drugs, disease-related fatigue, or nerve conduction block due to elevated body temperature may independently compromise respiratory muscle function.
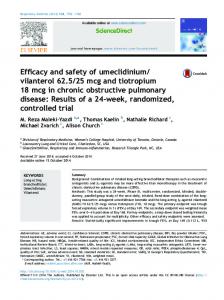
Respiratory failure Respiratory failure occurs in the terminal stages of MS and is usually associated with significant bulbar or limb paralysis [9]. It is rare in ambulatory patients. Respiratory failure may be acute, typically secondary to demyelinating lesions in the cervical cord or the medulla (Fig. 1), or chronic, typically found in the terminal stages of the disease and related to weak respiratory muscles, and ineffective cough, leading to aspiration, atelectasis and pneumonia [9e11]. Of the two types, only acute respiratory failure is potentially reversible with treatment [10]. Acute respiratory failure is a rather uncommon entity. Its clinical characteristics primarily have been described in single cases or small patient series [9,10,12e18]. Patients at risk are those with the relapsing-remitting form of MS and new extensive demyelinating plaques [10], with acute respiratory failure occurring after a median of 6 years from disease onset. Dyspnea, orthopnea or confusion often develops over a period of hours or days in patients with no preexisting respiratory problems. Rapid shallow breathing with diminished abdominal excursions or abdominal paradox occurs when there is marked diaphragmatic weakness [10]. Forced vital capacity (FVC) is markedly diminished, with values often being less than 1 L. A decrement of vital capacity (VC) in the supine position of more than 30% of that measured in the upright position is indicative of bilateral diaphragm dysfunction [19] and may be seen in a significant proportion of patients with acute respiratory failure [10]. On MRI, individuals often have demyelinating lesions involving the medulla or the spinal cord interfering with motor output to the respiratory muscles. In the series of Howard et al., the majority of patients had quadriplegia, or spastic paraplegia with upper arm weakness, of moderate or severe degree [10].
Table 1
Types of respiratory dysfunction in MS.
Respiratory muscle weakness Bulbar dysfunction Control of breathing abnormalities Sleep disordered breathing Respiratory failure Neurogenic pulmonary edema
Respiratory dysfunction in MS
673
Figure 1 Digital T2-weighted MRI showing a demyelinating plaque in the medulla of a patient with relapsing-remitting multiple sclerosis and acute respiratory failure. The respiratory failure resolved following treatment with intravenous methylprednisolone. (Reproduced from Pinedo et al. [15] with permission).
The chronic type of respiratory failure usually occurs in the terminal stages of the disease and is associated with significant bulbar dysfunction [10]. Typically these patients are wheelchair bound, with upper extremity weakness and weak respiratory muscles [10]. Frequent episodes of aspiration and atelectasis in conjunction with respiratory muscle weakness and a weak cough may lead to bouts of pneumonia and frequent hospitalizations. However, advanced respiratory support with mechanical ventilation and/or permanent tracheostomy is unusual in MS. Pittock et al. described 22 MS patients over a period of 33 years who required mechanical ventilation or tracheostomy [20]. The most common indications for mechanical ventilation or tracheostomy were aspiration pneumonia, and mucous plugging and difficulty in removing bronchial secretions [20]. The majority of patients had progressive MS, with a median survival of 22 months following institution of mechanical ventilation [20].
Respiratory muscle weakness Respiratory muscle weakness is a frequent finding in patients with MS. Usually, it is not severe enough to cause respiratory failure but strength can be reduced to a degree sufficient to be associated with other respiratory complications. In studies of individuals with MS, respiratory muscle strength was evaluated by measuring maximal static mouth inspiratory (MIP) and maximal static mouth expiratory pressure (MEP) [11,21e25]. These tests reflect the global strength of inspiratory and expiratory muscles. Specific evaluation of diaphragmatic function such as measurement of transdiaphragmatic pressure during volitional efforts have only been reported in occasional patients with acute respiratory failure [9,14]. A universal finding of all studies is decreased indices of MIP and MEP in MS. In general, respiratory muscle weakness is more pronounced in bedridden or wheelchair bound patients than in ambulatory MS patients (Table 2) [11,21e23,25] and the decrement of MEP is proportionally greater than that of MIP [11,21e26]. In these studies [11,21,23,25e27], MEP more often than MIP correlated with the level of disability (EDSS score) [11,21,23,25,26].
Diaphragm weakness in MS usually occurs in conjunction with weakness of other respiratory muscles. In the study by Howard et al. [10], diaphragmatic weakness was diagnosed clinically on the basis of orthopnea, severe sleep disturbance, abdominal paradox, and significant reduction of VC in the supine position. MRI or autopsy findings were consistent with severe involvement of the medulla and cervical cord to the C7 level. Patients with diaphragmatic weakness usually have advanced disease, quadriplegia, and bulbar dysfunction [10,14]. Isolated diaphragmatic paralysis in the absence of bulbar or limb weakness is rare [9,12]. In ambulatory patients with MS, electrophysiologic evaluation of the diaphragm by means of magnetic transcranial, magnetic cervical, or electrical stimulation of the phrenic nerves revealed abnormal diaphragmatic latency and compound muscle action potential in a significant portion of patients, even in patients with normal pulmonary function studies [28,29]. Respiratory muscle strength indices do not typically correlate with duration of illness [30,31]. Respiratory muscle weakness, particularly expiratory muscle weakness, is more prevalent in patients with upper extremity weakness, and the presence of a weak cough, difficulty in clearing secretions, as rated by the patient and examiner, and by the patient’s ability to count on a single exhalation (these clinical signs comprise the “pulmonary index”) [23]. In the study by Smeltzer et al. [23], the pulmonary index, upper extremity weakness and the maximal voluntary
Table 2 Respiratory muscle strength indices (% predicted) and MVV (% predicted) in MS patients categorized according to level of disability.
Ambulatory Wheelchair-bound Bedridden
MIP
MEP
MVV
87 83 76
73 55 36
88 55 31
MVV, maximal voluntary ventilation; MIP, maximal inspiratory pressure; MEP, maximal expiratory pressure. Adapted from Tantucci et al. [25] and Smeltzer et al. [23].
674 ventilation accounted for 60% of the variance of MEP. The high prevalence of expiratory muscle weakness in patients with upper arm weakness is most likely explained by the pattern of progression of paralysis. Because paralysis in advanced MS usually ascends from lower to upper extremities, abdominal muscle involvement occurs earlier than involvement of the diaphragm and the intercostal muscles and thus expiratory muscle strength function will be compromised to a greater extent than inspiratory muscle strength [11]. Respiratory muscle weakness may result from multiple causes, with demyelination of respiratory motor pathways being the most important cause. Additional causes include inactivity and muscle deconditioning, steroid induced myopathy in patients treated chronically with steroids, and malnutrition [32]. Fatigue, a quite common and debilitating symptom in MS, may also contribute to respiratory muscle weakness in these patients. Current evidence suggests that fatigue is related to a reduced voluntary activation of muscles due to failure to sustain the required neural drive to the muscle (central fatigue) [33]. As with peripheral muscles [34], incomplete activation or dyscoordination [35] of the respiratory muscles will similarly lead to muscle weakness. Finally, in patients with bulbar dysfunction and facial weakness, respiratory muscle strength indices may be falsely low due to inability of patients to make a tight seal around the mouthpiece [36,37]. Despite severe decrements in inspiratory and expiratory muscle strength, patients with MS rarely complain of dyspnea [11,22]. Possible explanations for the lack of dyspnea are the limited capacity of patients to exert because of peripheral motor abnormalities, marked fatigue, or cognitive impairment which occurs late in the course of the disease [11,22].
Impaired cough An effective cough is essential for clearing respiratory secretions and keeping the airways free of foreign material [38]. The normal cough consists of three components, an inspiratory phase, glottis closure, and an expiratory phase during which high expiratory flows are generated [39]. Cough expiratory flows normally range from 6 to 16 L/s and depend upon the strength of expiratory muscles and normal bulbar function [39,40]. In patients with MS, cough efficiency may be impaired because of expiratory muscle weakness or bulbar dysfunction. The latter may interfere with glottis closure and thus limit the pre-expiratory augmentation of intrathoracic pressure [39,41]. Cough efficacy can be assessed by measuring peak cough gastric pressure or peak cough flow [42]. Measures of MEP to assess cough efficiency may be limited in patients with neuromuscular disease. A low MEP may result from poor effort or difficulties with the maneuver especially in presence of bulbar dysfunction and may not indicate the presence of expiratory muscle weakness [42]. A recent study [21] in patients with MS reported decreased cough peak flow and cough gastric pressure, which were correlated with disease disability (EDSS score). In the same study [21], an EDSS score >5.5 was consistent with impaired cough with a sensitivity of 0.85 and a specificity of 0.95. Measures of
G.E. Tzelepis, F.D. McCool cough gastric pressure or peak cough flow in patients with MS may help identify those at risk for developing the respiratory complications due to ineffective cough.
Control of breathing Abnormalities of the control of breathing may result from involvement of one of the respiratory centers located in the brain stem. The dorsal medullary group (nucleus tractus solitarius) is primarily responsible for inspiration and generation of the basic breathing rhythm whereas the ventral medullary group (nucleus retroambiguous) is primarily responsible for expiration when expiration becomes an active process. Thus the ventral medullary group affects timing during exercise or other conditions requiring an increase in minute ventilation [43]. The output of both medullary respiratory centers is controlled by higher respiratory centers located in the pons [43]. Involvement of these higher respiratory centers in MS result in abnormal breathing patterns such as the loss of voluntary and/or automatic control of respiration, paroxysmal ventilation, and apneustic breathing, which refers to sustained inspiratory contraction and a prolonged pause at full inspiration [2,10,44]. Their overall incidence is low, with most of the clinical features described in single case reports [2,35,44e49] or small patient series [10]. With loss of voluntary control of breathing, patients are unable to increase their tidal volume or stop breathing voluntarily [48] whereas loss of automatic control of breathing manifests as apnea or respiratory arrest during sleep [45,46,49]. In patients with loss of voluntary control, MRI and autopsy reports have revealed lesions involving the corticospinal tracts bilaterally, brainstem, or upper cervical cord. Patients who exhibit loss of automatic control have lesions involving the dorsomedial medulla, nucleus ambiguous, and medial lemnisci [2,10]. Paroxysmal hyperventilation and apneustic breathing are associated with lower brainstem lesions [2,44]. These abnormalities in respiratory control may be seen in patients with acute respiratory failure and quadriparesis [2,10] but may be present in patients with sleep disordered breathing, especially central sleep apnea. Stable patients with moderate to severe MS and weak respiratory muscles likely exhibit no abnormalities in respiratory control. Tantucci et al. reported increased respiratory drive at rest as indicated by a relatively high mouth occlusion pressure measured 0.1 s after onset of inspiratory effort (P0.1) [25]. The P0.1 response to hypercapnia was preserved while the overall ventilatory response to hypercapnia was markedly reduced [25]. Respiratory muscle dysfunction could in part account for these abnormalities [25].
Sleep-disordered breathing Patients with MS report various sleep complaints including insomnia, excessive daytime somnolence, and restless sleep more often than control subjects [50]. Sleep abnormalities have a significant impact on quality of life in these patients [51]. Because fatigue is the most common symptom in MS, the clinician often has to differentiate excessive daytime sleepiness secondary to a sleep disorder from
Respiratory dysfunction in MS excessive fatigue in these patients [52e54]. Furthermore, fatigue by itself is associated with disrupted sleep and abnormal sleep cycles [55]. Sleep disordered breathing may have the form of obstructive sleep apnea (OSA), central apnea or nocturnal hypoventilation and manifest with daytime somnolence, fatigue, decreased concentration, mood changes or decreased libido [52]. The prevalence of sleep disordered breathing in MS patients is unknown. In 28 consecutive patients initially screened with pulse oximetry and subsequently studied with polysomnography, OSA was documented in 2 patients (8%) [56]. In these two patients, OSA was not associated with a specific MRI lesion distribution [56]. Recent studies reported a higher prevalence of OSA (21%) and central sleep apnea, especially in MS patients with brainstem involvement [57,58]. In few reported cases, central sleep apnea which was associated with demyelinating lesions in the medulla [45] contributed to death in these patients [10,45]. Independent of central sleep apnea, nocturnal hypoventilation may also result from significant respiratory muscle weakness due to reduced tidal volume during REM sleep. It typically occurs in bedridden patients with advance disease and diaphragm weakness [10,12]. As with other neuromuscular diseases, nocturnal hypoventilation may develop insidiously prior to onset of respiratory failure [10].
Neurogenic pulmonary edema Neurogenic pulmonary edema rarely occurs in MS and is similar to that reported in patients with other neurological disorders. It may occur in patients with an established diagnosis of MS [2,59e62] or as the initial manifestation of the disease [63,64]. Recurrent episodes of neurogenic pulmonary edema requiring intubation and mechanical ventilation were reported by Simon et al. in a female patient with MS during disease exacerbations [59]. The pathogenesis of neurogenic pulmonary edema is not entirely known, but in most reports neurogenic pulmonary edema was associated with new demyelinating lesions involving the caudal medulla in the region of nucleus tractus solitarius [2,62]. As with other cases of neurologically-induced pulmonary edema, it is believed that involvement of specific brain regions about the caudal medulla that regulate cardiac function, systemic blood pressure and pulmonary hydrostatic pressure are responsible for sympathetic overstimulation which then leads to an increase in hydrostatic pulmonary pressure and development of pulmonary edema [65].
675 suggestive of diaphragmatic weakness [19]. Dyspnea with exertion may not be present because these patients often have limited exercise capacity. Excessive daytime sleepiness and morning headache may be due to nocturnal hypoventilation. Symptoms related to sleep apnea may be present in patients with bulbar dysfunction. Neurological exam is often essential in ascribing respiratory distress to respiratory muscle dysfunction. Patients with upper arm weakness, paraplegia, or bulbar dysfunction are more likely to have involvement of the respiratory muscles [10]. These patients typically describe weak cough and inability to clear secretions and often have difficulties with speech [66]. However, the finding of severe arm weakness in patients with respiratory distress does not invariably indicate a cause-and-effect relationship [46].
Pulmonary function tests Pulmonary function testing may provide clues as to whether respiratory muscle dysfunction is present. Lung volumes such as total lung capacity (TLC), VC, and residual volume (RV) may be reduced in patients with severe respiratory muscle weakness. However, the strength of the respiratory muscles must be reduced to as much as 50% of predicted before any significant reduction in lung volume is measured [67]. Thus, these lung volumes may be normal in patients with mild to moderate respiratory muscle weakness [11,21] and are likely diminished in bedridden patients who have respiratory muscle weakness [32]. FVC is usually within the normal range in ambulatory or ambulatory with assistance (Kurtze Expanded Disability Status Scale, EDSS