Physiology of Complement-Related Hemolytic Anemia. Robert A. Brodsky, MD.
You are asked to see a 37-year-old male carpenter who was noted to be anemic
...
PHYSIOLOGY IN MEDICINE: A SERIES OF ARTICLES LINKING MEDICINE WITH SCIENCE Physiology in Medicine: Dale J. Benos, PhD, Editor; Edward Abraham, MD, Associate Editor; Peter D. Wagner, MD, Associate Editor
Review
Annals of Internal Medicine: Harold C. Sox, MD, Series Editor
Narrative Review: Paroxysmal Nocturnal Hemoglobinuria: The Physiology of Complement-Related Hemolytic Anemia Robert A. Brodsky, MD
Clinical Principles
Pathophysiologic Principles
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare hematopoietic stem-cell disorder caused by a somatic mutation in a gene known as phosphatidylinositol glycan class A (PIGA). It may arise de novo or in the setting of acquired aplastic anemia.
The product of the PIGA gene is required for the biosynthesis of a glycolipid anchor that attaches a class of membrane proteins known as glycosylphosphatidylinositol (GPI)– anchored proteins to the cell surface.
Clinical presentation can include hemolytic anemia, hemoglobinuria, thrombosis, severe fatigue, abdominal pain, and esophageal spasm. Thrombosis, the leading cause of death from PNH, most commonly occurs in abdominal and cerebral veins. Therapeutic options include supportive care, bone marrow transplantation, and monoclonal antibody therapy with the terminal complement inhibitor eculizumab.
The absence of GPI-anchored proteins leads to complementmediated intravascular hemolysis, because 2 important complement regulatory proteins (CD55 and CD59) are missing from PNH cells. Hemolysis in PNH occurs intravascularly. This leads to release of free hemoglobin, a potent nitric oxide scavenger. Depletion of nitric oxide at the tissue level contributes to fatigue, esophageal spasm, thrombosis, and male erectile dysfunction. Eculizumab decreases hemolysis in PNH by binding to C5 and blocking the terminal portion of the complement cascade.
Y
ou are asked to see a 37-year-old male carpenter who was noted to be anemic and mildly thrombocytopenic during a routine physical examination. The patient has been married for 11 years and has a 5-year-old son and an 8-year-old daughter. He reports that he has been in good health but has noted increasing fatigue over the past 2 months. Two weeks ago, he and his son had viral gastroenteritis that manifested with nausea and diarrhea. His son recovered within 24 hours, but the patient had burgundy-colored urine that persisted for 2 additional days (Figure 1). On physical examination, the patient is well developed and well nourished, has mildly icteric sclera, and has mild discomfort on deep abdominal palpation but no masses or organomegaly. Complete blood count reveals a leukocyte count of 4.7 ⫻ 109 cells/L with a normal differential, hemoglobin level of 84 g/L, and platelet count of 96 ⫻ 109 cells/L. His absolute reticulocyte count is 322.5 ⫻ 109 cells/L, and his lactate dehydrogenase level is 2950 U/L. His biochemical profile was canceled by the clinical laboratory due to a “hemolyzed specimen.” Urinalysis reveals a marked increase in hemoglobin but no erythrocytes. Flow cytometric analysis of his peripheral blood using anti-CD59 and
fluorescein-labeled proaerolysin (FLAER) (see Glossary) reveals that most granulocytes were missing glycosylphosphatidylinositol (GPI)–anchored (see Glossary) proteins, consistent with a diagnosis of paroxysmal nocturnal hemoglobinuria (PNH) (Figure 2). Two weeks later, the patient has a similar episode of hemoglobinuria associated with extreme fatigue, severe abdominal pain, esophageal spasm, and erectile dysfunction. Hemoglobin level is now 70 g/L, and lactate dehydrogenase level is 3450 U/L. The patient begins taking weekly doses of intravenous eculizumab (see Glossary), 600 mg for 4 weeks and then 900 mg every other week. Within 2 days of starting
See also: Print Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 589 Web-Only CME quiz Conversion of graphics into slides
Ann Intern Med. 2008;148:587-595. For author affiliation, see end of text.
© 2008 American College of Physicians 587
Review
Physiology of Complement-Related Hemolytic Anemia
Figure 1. Early morning urine sample in a patient with paroxysmal nocturnal hemoglobinuria.
ment-mediated hemolysis that is characteristic of PNH (12, 13).
HISTORY
eculizumab therapy, most symptoms resolved, and after 6 months, he reports no further hemolytic episodes and marked improvement in his energy level. He has no further episodes of esophageal spasm, and erectile dysfunction has resolved. Hemoglobin level is 101 g/L, platelet count is 107 ⫻ 109 cells/L, and lactate dehydrogenase level has decreased to 359 U/L. Paroxysmal nocturnal hemoglobinuria is a rare clonal hematopoietic stem-cell disorder (approximately 1 to 2 cases per 1 million people in the United States) with protean clinical manifestations (1). The disease manifests with complement-mediated intravascular hemolysis, smoothmuscle dystonia, and thrombosis (1– 4). It can arise spontaneously or evolve from acquired aplastic anemia (5– 8). The median age of presentation is 40 years, but the disease occurs in all age groups (2, 3, 9, 10). It is an acquired genetic disorder that results from a mutation occurring during life rather than being inherited from a parent. With supportive care alone, median survival is roughly 10 to 15 years. Thrombosis is the leading cause of death (2, 3, 11). Virtually all clinical manifestations of PNH result from the absence of a class of cell membrane proteins known as GPI-anchored proteins. At least 2 of these GPI-anchored proteins (CD55 and CD59 [see Glossary]) normally function as complement (see Glossary) regulatory proteins; their absence from PNH erythrocytes explains the comple588 15 April 2008 Annals of Internal Medicine Volume 148 • Number 8
Dr. Paul Stru¨bing provided one of the earliest descriptions of PNH (14). In 1882, he reported a 29-year-old cartwright who presented with fatigue, abdominal pain, and severe nocturnal paroxysms of hemoglobinuria. Later reports by Marchiafava and Micheli led to the eponym the Marchiafava–Micheli syndrome, but Enneking introduced the term paroxysmal nocturnal hemoglobinuria in 1925 (15). In 1937, Thomas Ham found that PNH erythrocytes hemolyzed when incubated with normal, acidified serum (16). This seminal discovery resulted in the first diagnostic test for PNH: the acidified serum, or Ham, test. Erythrocyte lysis following acidified serum seemed to be complement-dependent because heat inactivation abrogated the reaction; however, it was not until 1954, with the discovery of the alternative pathway of complement activation, that increased complement sensitivity was proven to cause hemolysis of PNH erythrocytes (17). After the emergence of specific diagnostic tests, researchers discovered additional disease manifestations associated with PNH, such as venous thrombosis, smooth-muscle dystonia, and other clonal stem-cell disorders. These nonerythroid manifestations of the disease foreshadowed the discovery that PNH results from clonal expansion of a mutated hematopoietic stem cell, and all of a patient’s PNH cells are therefore the progeny of that cell. In the 1980s, investigators discovered that PNH cells are deficient in a group of proteins normally attached to the cell surface by a GPI moiety. Of interest, 2 of these missing proteins (CD55 and CD59) are important complement regulatory proteins. Investigators discovered the genetic mutation responsible for the defective GPI-anchor protein a few years later (18). Most recently, a humanized monoclonal antibody that inhibits terminal complement activation has been shown to alleviate hemolysis and disease symptoms in patients with PNH (19, 20).
GPI-ANCHORED PROTEINS Most cell membrane proteins have a transmembrane region that spans the lipid bilayer 1 or more times. The members of a small subset of membrane proteins are individually tethered to the lipid bilayer by a GPI glycolipid moiety (Figure 3). Hematopoietic cells contain more than a dozen different, important GPI-anchored proteins, including blood group antigens, adhesion molecules, complement regulatory proteins, enzymes, and receptors. The structure of GPI-anchored proteins has remained very similar throughout evolution, which means that the proteins are essential for survival. A GPI anchor comprises 3 main elements: a molecule of phosphatidylinositol, a glycan core, and a molecule of phosphoethanolamine, to which the prowww.annals.org
Physiology of Complement-Related Hemolytic Anemia
tein is covalently attached (21–23). Glycosylphosphatidylinositol is synthesized in the endoplasmic reticulum and transferred en bloc to the carboxyl terminus of a protein that has a GPI attachment signal (see Glossary) peptide. Biosynthesis of GPI anchors involves at least 10 chemical steps and more than 20 different genes (23); therefore, researchers were initially surprised to find that the somatic mutation that causes PNH always occurs on the same gene. This puzzle soon had an answer.
MOLECULAR BIOLOGY
OF
PNH
To date, all patients with PNH have had genetic mutations in an X-linked gene known as phosphatidylinositol glycan class A (PIGA) (see Glossary) (8, 18, 24, 25). The PIGA gene product is required for the first step in the assembly of GPI anchors (26); thus, PIGA gene mutations block the biosynthesis of the GPI anchor. Failure to synthesize a mature GPI anchor causes cognate proteins (see Glossary) to be degraded intracellularly, including those involved in complement regulation. As a result, no GPIanchored proteins appear on the cell surface. Why is the somatic mutation in PNH always in the PIGA gene? Unlike the other genes involved in GPI anchor biosynthesis, PIGA is located on the X chromosome. Because males and females have only 1 active X chromosome per cell (in females, 1 X chromosome is inactivated through lyonization), it is possible for a single somatic mutation to generate a PNH phenotype. All other involved genes are found on autosomes, meaning that inactivating mutations would have to occur on both copies of a gene in the same stem cell—a statistically unlikely occurrence.
COMPLEMENT-MEDIATED HEMOLYSIS
IN
PNH
The term nocturnal is misleading—it implies that the hemolysis is somehow triggered only at night— but in fact, it can occur at any time. The more concentrated morning urine makes hemoglobinuria even more conspicuous and probably led to the misleading name. Hemolysis in PNH results from the increased susceptibility of PNH erythrocytes to complement (12, 13, 27, 28). Complement can be activated by 3 pathways: the classic pathway, the lectin pathway, and the alternative pathway (29). Paryoxysmal nocturnal hemoglobinuria erythrocytes are vulnerable to complement activation through any of these pathways; however, the alternative pathway is in a state of continuous activation, which explains why hemolysis can occur at any time in patients with PNH. Paroxysmal nocturnal hemoglobinuria erythrocytes are highly vulnerable to complement-mediated lysis due to a reduction, or absence, of 2 important GPI-anchored complement regulatory membrane proteins (CD55 and CD59). CD59 is a 19 000molecular-weight glycoprotein that directly prevents the membrane attack complex (see Glossary) from forming a www.annals.org
Review
Glossary Cognate protein: Protein that possesses a glycosylphosphatidylinositol (GPI) attachment signal and is destined to be attached to the cell membrane by a GPI anchor. Complement: Battery of more than 25 proteins that combine with antibodies or cell surfaces, participate in killing certain bacteria, produce chemotactic substances, increase vascular permeability, and promote mast cell degranulation. Complement is activated by any of 3 pathways: the classical, activated by antibody; the lectin, activated by mannose-binding lectin; and the alternative, which is continuously activated at a low level due to spontaneous hydrolysis. CD55: Cell-surface GPI-anchored protein that blocks C3 convertase. Its deficiency in paroxysmal nocturnal hemoglobinuria (PNH) erythrocytes is partly responsible for their increased susceptibility to complement-mediated intravascular hemolysis. CD59: GPI-anchored protein that normally functions to regulate formation of the membrane attack complex by interfering with its assembly. Eculizumab: Humanized monoclonal antibody that binds to C5 and prevents cleavage of C5 into C5a and C5b; lack of C5b prevents formation of the membrane attack complex and protects PNH cells from complement-mediated hemolysis. FLAER: Fluorescein-labeled variant of proaerolysin that binds with high specificity to GPI-anchored proteins. It is useful as a diagnostic reagent in PNH. GPI anchor: Highly evolutionarily conserved glycolipid moiety comprising a molecule of phosphatidylinositol, a glycan core containing 3 mannoses, and an ethanolamine phosphate that tethers certain proteins (e.g., CD55 and CD59) to the cell membrane. GPI attachment signal: Hydrophobic domain located at the carboxyl terminus of a protein that “directs” attachment of the protein to a mature GPI anchor. Membrane attack complex: Comprises C5b, C6, C7, C8, and multiple units of C9. These terminal complement proteins form a channel that causes cell lysis. Multipotent hematopoietic stem cell: Bone marrow–derived cell with extensive self-renewal capacity and the ability to differentiate into all lymphohematopoietic lineages. Phosphatidylinositol glycan class A (PIGA) gene: One of more than 20 genes required for the biosynthesis of GPI anchors. The PIGA gene is required for the first step in the pathway; mutations of this gene lead to a marked deficiency in or absence of all GPI-anchored proteins. All patients with PNH to date have been found to harbor clonal PIGA mutations. Proaerolysin: Protoxin secreted by the bacterium Aeromonas hydrophila. The GPI-anchored proteins serve as the receptor for this channel-forming toxin. The toxin does not bind to PNH cells, because they are deficient in GPI-anchored proteins.
hole in the cell membrane by blocking the aggregation of C9 (13, 30). CD55, a 68 000-molecular-weight glycoprotein, accelerates the rate of destruction of membranebound C3 convertase (12). Hence, CD55 reduces the amount of C3 that is cleaved and CD59 reduces the number of membrane attack complexes that are formed. Of these, CD59 is more important in protecting cells from complement.
SMOOTH-MUSCLE DYSTONIA
IN
PNH
Many clinical manifestations of PNH are readily explained by hemoglobin-mediated nitric oxide scavenging after free hemoglobin is released from hemolyzed cells (31, 32). Nitric oxide is a major regulator of vascular physiology. Normally, oxygen and arginine react with nitric oxide synthase in the endothelium to produce nitric oxide and citrulline. Nitric oxide then acts on the vascular wall to 15 April 2008 Annals of Internal Medicine Volume 148 • Number 8 589
Review
Physiology of Complement-Related Hemolytic Anemia
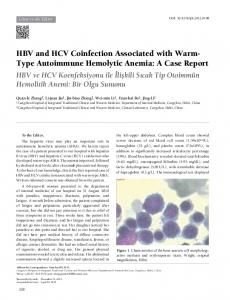
Figure 2. Flow cytometric assay of normal and paroxysmal nocturnal hemoglobinuria granulocytes.
100
Cell Frequency
80
60
thesis (34, 35). Haptoglobin removes free hemoglobin, but the concentration of plasma hemoglobin in PNH exceeds the capacity of haptoglobin to remove the hemoglobin from the plasma (31). Depletion of nitric oxide at the tissue level manifests clinically as fatigue, abdominal pain, esophageal spasm, erectile dysfunction, and possibly thrombosis; hemoglobinuria, thrombosis, male erectile dysfunction, and esophageal spasm are much more common in patients with PNH who have large populations of PNH cells (⬎60% of granulocytes) (2).
40
THROMBOSIS 20
0 100
101
102
103
Fluorescence Intensity
100
Cell Frequency
80
60
40
20
0 100
101
102
103
Fluorescence Intensity
Top. Granulocytes from a normal control participant show bright fluorescein-labeled proaerolysin (FLAER) staining in all cells. Bottom. A patient with paroxysmal nocturnal hemoglobinuria who has a large population of paroxysmal nocturnal hemoglobinuria granulocytes (84% FLAER-negative) and 16% normal granulocytes.
maintain normal tone and limit platelet activation. Free hemoglobin has enormous affinity for nitric oxide and can reduce the plasma level of nitric oxide to the point of causing symptoms; the administration of cell-free hemoglobin solutions to healthy volunteers and patients is associated with development of abdominal pain and esophageal spasm (33). Under normal conditions, hemoglobin is sequestered by the erythrocyte membrane, which minimizes the scavenging of nitric oxide. In PNH, failure to regulate complement on the erythrocyte membrane can lead to massive intravascular hemolysis, resulting in release of large amounts of free hemoglobin and erythrocyte arginase into the plasma. This leads to scavenging of nitric oxide and degradation of the substrate (arginine) for nitric oxide syn590 15 April 2008 Annals of Internal Medicine Volume 148 • Number 8
IN
PNH
Thrombosis—the leading cause of death in PNH— occurs in up to 40% of patients. Venous thrombosis in PNH can occur anywhere, with the abdominal veins (hepatic, portal, splenic, and mesenteric) and the cerebral veins being the most common sites. Patients with a large PNH cell population (⬎60% of granulocytes) seem to be at greatest risk for thrombosis. The mechanism of thrombosis in PNH is not entirely understood and is probably multifactorial; however, it must also relate to the GPI anchor protein deficiency. Nitric oxide depletion is associated with increased platelet aggregation, increased platelet adhesion, and accelerated clot formation (32). In an attempt to repair the damage, platelets in patients with PNH undergo exocytosis of the complement attack complex, leading to formation of microvesicles lined with phosphatidylserine on their external surface (36). Phosphatidylserine is a potent procoagulant that is normally confined to the inner leaflet of the plasma membrane; the circulating microvesicles from PNH platelets activate coagulation and probably contribute to thrombophilia in PNH (37). Fibrinolysis may also be disrupted in PNH, because PNH blood cells lack the GPI-anchored receptor for urokinase-type plasminogen activator (38). Urokinase normally cleaves plasminogen to generate plasmin, regulating fibrinolysis. Finally, tissue factor pathway inhibitor, a major inhibitor of the procoagulant tissue factor, requires a GPI-anchored protein as a cofactor (39).
DIAGNOSTIC ASSAYS The Ham test and the sucrose hemolysis test (sugar water test) were 2 of the first assays used to diagnosis PNH (16, 40). Both assays are performed on erythrocytes and discriminate PNH cells from normal cells on the basis of their greater sensitivity to the hemolytic action of complement. These assays are relatively insensitive and nonspecific, especially in patients requiring red blood cell transfusions. Monoclonal antibodies to GPI-anchored proteins (for example, anti-CD59 and anti-CD55) began to replace the sucrose hemolysis and Ham tests in the early 1990s (41, 42). Later assays were based on the discovery that GPI-anchored proteins were receptors for proaerolysin (see www.annals.org
Physiology of Complement-Related Hemolytic Anemia
Glossary), a bacterial channel-forming toxin derived from Aeromonas hydrophila (43). Because PNH cells are deficient in GPI-anchored proteins, they are resistant to the toxin (44). A fluoresceinated proaerolysin variant (FLAER) that binds to the GPI anchor without forming channels can be used in conjunction with flow cytometry to diagnose PNH (45, 46), because it binds to normal mononuclear cells but not PNH cells. Most clinical laboratories in the United States now use flow cytometry– based assays to diagnose PNH; these tests are more sensitive and specific than the complement-based assays and can measure the size of the PNH cell population. Flow cytometric analysis of granulocytes is the best way to diagnose PNH; flow cytometric analysis of erythrocytes alone is not optimal. Erythrocyte assays underestimate the size of the PNH clone because PNH erythrocytes are more susceptible to complement-mediated lysis. In addition, red blood cell transfusions from healthy donors can mask a small PNH erythrocyte population; however, red blood cell or platelet transfusions would not affect the percentage of PNH granulocytes. Granulocytes are also most representative of the PNH stem cell pool due to their half-life of several hours. In contrast, T lymphocytes tend to be the least affected lineage in PNH (that is, they have the lowest percentage of GPI anchor– deficient cells) due to their half-life of months to years.
STEM CELLS
IN
PNH
In patients with PNH, GPI-anchored protein– deficient erythroid, myeloid, and lymphoid cells are clonal; every PNH cell has the same PIGA gene mutation. From these observations, one can infer that PNH originates in a multipotent hematopoietic stem cell (see Glossary) in which the PIGA gene has undergone somatic mutation (47, 48). Of interest, granulocytes from the blood of 1 in 50 000 healthy control participants also harbor a mutation of the PIGA gene (49). In contrast to the PIGA gene mutations associated with PNH, most PIGA gene mutations in healthy control participants arise from a more differentiated colony-forming cell rather than a multipotent hematopoietic stem cell (48). Unlike hematopoietic stem cells, colony-forming cells have no capacity for self-renewal; mutations arising at this level of hematopoietic differentiation will not be propagated beyond their fully differentiated progeny and are too few in number to cause human disease. (Rare granulocytes from healthy control participants even contain BCR-ABL translocations.) These observations suggest that most, if not all, clonal hematopoietic stem-cell disorders must arise from cells with extensive self-renewal capacity. Whether PIGA gene mutations occurring in a multipotent hematopoietic stem cell are sufficient to cause the disease is not known; immune selection or secondary www.annals.org
Review
mutations may be necessary to give the PNH clone a survival advantage (50, 51).
PNH
VERSUS
APLASTIC ANEMIA
Acquired aplastic anemia and PNH are closely related diseases that are sometimes confused. Paroxysmal nocturnal hemoglobinuria often occurs in patients with preexisting aplastic anemia, and many patients with aplastic anemia have small to moderate numbers of PNH granulocytes (typically ⬍20%) at diagnosis (46, 52), which often leads to confusion about whether PNH or aplastic anemia is the primary disorder. The apparent lack of a threshold PNH cell population above which hemolysis or thrombosis consistently occurs adds to the confusion over diagnosis. The classic definition of PNH (classic PNH) requires evidence of intravascular hemolysis; patients with hypocellular bone marrow and a small PNH population without intravascular hemolysis should be classified as having aplastic anemia with a subpopulation of PNH cells. Distinguishing between classic PNH and aplastic anemia is important because treatment differs considerably. Patients with aplastic anemia have symptoms of anemia, thrombocytopenia, and neutropenia because of inadequate bone marrow production (46); treatment— usually immunosuppression or bone marrow transplantation—should target aplastic anemia rather than the small PNH population. Classic PNH manifests with overt hemolysis, an elevated reticulocyte count, an elevated lactate dehydrogenase level, normal to hypercellular bone marrow, and a large population of PNH granulocytes (typically ⬎50%). As discussed in the next section, treatment of classical PNH is highly specific.
THERAPEUTIC OPTIONS Clinical manifestations of PNH range from indolent to life-threatening. Patients with minimal symptoms should receive folic acid supplementation and supportive care. Corticosteroids are sometimes helpful, but prolonged
Figure 3. Schematic representation of cell membrane showing transmembrane proteins and glycosylphosphatidylinositol (GPI)–anchored proteins. Transmembrane proteins
GPI-anchored protein
Extracellular space
Lipid bilayer Cytoplasm
The lipid portion of the GPI anchor inserts into the lipid bilayer; no peptide transmembrane portion or cytoplasmic tail is present. 15 April 2008 Annals of Internal Medicine Volume 148 • Number 8 591
Review
Physiology of Complement-Related Hemolytic Anemia
use should be avoided. Prophylactic anticoagulation has not been proven to decrease the risk for thrombosis (53). Managing patients with PNH receiving warfarin can also be challenging; they often have low platelet counts, and a therapeutic international normalized ratio is difficult to maintain in patients having frequent paroxysms, which may be associated with abdominal pain, nausea, and vomiting. No widely accepted, evidence-based indications for treatment of PNH exist. Disabling fatigue, thromboses, transfusion dependence, or frequent pain paroxysms are often used as indications for more aggressive therapy. Two major treatment modalities have emerged: allogeneic bone marrow transplantation and protection of PNH cells from the effects of terminal complement. Successful allogeneic bone marrow transplantation can cure the disease by replacing hematopoietic stem cells containing PIGA gene mutations with hematopoietic stem cells from a healthy donor (54); successful transplantation in patients with
PNH has been reported after myeloablative and nonmyeloablative conditioning regimens (55, 56). Despite its potential to cure the disease, allogeneic bone marrow transplantation is seldom used to treat PNH because of high morbidity and mortality; lack of suitable donors; and recent emergence of effective, specific drug therapy.
ECULIZUMAB Eculizumab is a humanized monoclonal antibody against C5 that inhibits terminal complement activation (Figure 4). In 2007, the U.S. Food and Drug Administration approved its use in PNH. A 12-week, open-label trial of eculizumab in 11 patients with PNH demonstrated that the drug reduced intravascular hemolysis and transfusion requirements (19). Subsequently, an international, doubleblind, randomized, placebo-controlled trial, TRIUMPH (Transfusion Reduction Efficacy and Safety Clinical Investigation, a Randomized, Multicenter, Double-Blind, Place-
Figure 4. Complement activation: classic, alternative, and lectin binding pathways converge at the point of C3 activation.
Classic pathway
Eculizumab
CD55
C5b
C5 Mannose-binding lectin pathway
C3 convertase
C5 convertase
C6
C5a C7
C8 Lytic pathway
Alternative pathway
us uo tin ion n Co tivat ac
C9
CD59
Membrane attack complex
The alternative pathway is in a state of continuous activation. The formation of C5 convertase initiates the lytic pathway and leads to the assembly of the membrane attack complex from C5, C6, C7, C8, and multiple C9 proteins. Normally, CD55 inhibits C3 convertases and CD59 blocks incorporation of C9 into the C5b– 8 complex. Eculizumab is a humanized monoclonal antibody that binds to C5, thereby preventing the formation of C5a and C5b (the initiating component of the membrane attack complex). 592 15 April 2008 Annals of Internal Medicine Volume 148 • Number 8
www.annals.org
Physiology of Complement-Related Hemolytic Anemia
bo-Controlled, Using Eculizumab in Paroxysmal Nocturnal Hemoglobinuria), showed that eculizumab stabilized hemoglobin levels and reduced transfusion requirements in PNH (20). The researchers randomly assigned 87 patients with PNH to receive either placebo (44 patients) or eculizumab (43 patients) intravenously at 600 mg weekly for 4 weeks, 900 mg the following week, and then 900 mg every 2 weeks for a total of 6 months. The primary end points were cellular hemoglobin stabilization and units of transfused blood. To be eligible, patients had to be red blood cell transfusion– dependent, have a platelet count greater than 100 ⫻ 109 cells/L, and have a lactate dehydrogenase level greater than 1.5 times the upper limit of normal. Stabilization of hemoglobin levels in the absence of transfusions was achieved in 49% (21 of 43 patients) of the patients assigned to eculizumab and none (0 of 44 patients) of those assigned to placebo (P ⬍ 0.001). During the 6-month study, the eculizumab group received a median of 0 units of packed red blood cells, compared with 10 units in the placebo group (P ⬍ 0.001). The eculizumab group had an 85.8% lower median area under the receiver-operating characteristic curve for lactate dehydrogenase levels plotted against time (in days) than the placebo group (58 587 vs. 411 822 U/L; P ⬍ 0.001), demonstrating that eculizumab reduced intravascular hemolysis. Patients who received eculizumab also experienced significant improvements in quality of life as measured by scores on the Functional Assessment of Chronic Illness Therapy-Fatigue instrument (P ⬍ 0.001) and the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire. The most common adverse events reported by patients who received eculizumab were headache, nasopharyngitis, back pain, and upper respiratory tract infections. Eculizumab decreased intravascular hemolysis in PNH, greatly improved quality of life, and reduced or eliminated the need for blood transfusions in most (but not all) patients. By reducing plasma free hemoglobin levels, eculizumab also mitigated the smooth-muscle dystonias that are often associated with PNH. More recent data (53) demonstrate that eculizumab decreases the risk for thrombosis in patients with PNH and show that patients with PNH and thrombocytopenia and transfusion requirements that are lower than those of TRIUMPH participants respond equally well (57). Several cautions apply to using eculizumab. First, blocking the terminal portion of the complement cascade predisposes patients to Neisseria infections; all patients taking eculizumab should be immunized against Neisseria infections 2 weeks before treatment begins. Even after vaccination, rare breakthrough Neisseria infections may occur. Second, eculizumab is most effective for patients with classic PNH who have high levels of intravascular hemolysis (lactate dehydrogenase level ⬎1.5 times the upper limit of normal and an elevated reticulocyte index). Third, patients with aplastic anemia are not likely to benefit from eculizumab; they generally have minor PNH cell populations, www.annals.org
Review
and anemia and fatigue are largely due to immune-mediated bone marrow failure and not intravascular hemolysis (58). Fourth, eculizumab is very expensive (more than $300 000 a year) and requires lifelong administration.
CONCLUSION Paroxysmal nocturnal hemoglobinuria is a rare, clonal, hematopoietic stem-cell disorder whose protean manifestations are almost entirely explained by complement-mediated intravascular hemolysis. The close association between PNH and aplastic anemia and the reason PNH stem cells achieve a growth advantage over normal stem cells are still not entirely understood. By interrupting the assembly of the membrane attack complex, eculizumab decreases intravascular hemolysis and reduces the risk for thrombosis in patients with PNH. Whether eculizumab improves survival remains to be determined. From Johns Hopkins Medical Institutions, Baltimore, Maryland. Grant Support: From the National Institutes of Health (P01CA70970). Potential Financial Conflicts of Interest: Consultancies: Alexion Pharmaceuticals. Honoraria: Alexion Pharmaceuticals. Grants received: National Institutes of Health. Patents received: U.S. patent number 6 393 095 B1 for detection of GPI-anchored proteins. Requests for Single Reprints: Robert A. Brodsky, MD, Division of Hematology, Johns Hopkins Medicine, Ross Research Building Room 1025, 720 Rutland Avenue, Baltimore, MD 21205-2196; e-mail,
[email protected].
References 1. Brodsky RA. Paroxysmal nocturnal hemoglobinuria. In: Hoffman R, Benz EJ Jr, Shattil SJ, Furie B, Cohen HJ, Silberstein LE, et al., eds. Hematology: Basic Principles and Practice. 4 ed. Philadelphia: Elsevier Churchill Livingston; 2005: 419-27. 2. Moyo VM, Mukhina GL, Garrett ES, Brodsky RA. Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays. Br J Haematol. 2004;126:133-8. [PMID: 15198744] 3. Hillmen P, Lewis SM, Bessler M, Luzzatto L, Dacie JV. Natural history of paroxysmal nocturnal hemoglobinuria. N Engl J Med. 1995;333:1253-8. [PMID: 7566002] 4. Rosse WF. Paroxysmal nocturnal hemoglobinuria as a molecular disease. Medicine (Baltimore). 1997;76:63-93. [PMID: 9100736] 5. Dameshek W. Riddle: what do aplastic anemia, paroxysmal nocturnal hemoglobinuria (PNH) and “hypoplastic” leukemia have in common? Blood. 1967; 30:251-4. [PMID: 6031145] 6. Lewis SM, Dacie JV. The aplastic anaemia—paroxysmal nocturnal haemoglobinuria syndrome. Br J Haematol. 1967;13:236-51. [PMID: 6019033] 7. Schrezenmeier H, Hertenstein B, Wagner B, Raghavachar A, Heimpel H. A pathogenetic link between aplastic anemia and paroxysmal nocturnal hemoglobinuria is suggested by a high frequency of aplastic anemia patients with a deficiency of phosphatidylinositol glycan anchored proteins. Exp Hematol. 1995;23: 81-7. [PMID: 7995374] 8. Nagarajan S, Brodsky RA, Young NS, Medof ME. Genetic defects underlying paroxysmal nocturnal hemoglobinuria that arises out of aplastic anemia. Blood. 1995;86:4656-61. [PMID: 8541558] 9. Socie G, Mary JY, de Gramont A, Gluckman E. Long term follow-up and prognostic factors in paroxysmal nocturnal hemoglobinuria (PNH): a study on 15 April 2008 Annals of Internal Medicine Volume 148 • Number 8 593
Review
Physiology of Complement-Related Hemolytic Anemia
203 cases by the French Society of Hematology [Abstract]. Blood. 1995;86:130a. 10. Ware RE, Hall SE, Rosse WF. Paroxysmal nocturnal hemoglobinuria with onset in childhood and adolescence. N Engl J Med. 1991;325:991-6. [PMID: 1886636] 11. Socie´ G, Mary JY, de Gramont A, Rio B, Leporrier M, Rose C, et al. Paroxysmal nocturnal haemoglobinuria: long-term follow-up and prognostic factors. French Society of Haematology. Lancet. 1996;348:573-7. [PMID: 8774569] 12. Medof ME, Kinoshita T, Nussenzweig V. Inhibition of complement activation on the surface of cells after incorporation of decay-accelerating factor (DAF) into their membranes. J Exp Med. 1984;160:1558-78. [PMID: 6238120] 13. Rollins SA, Sims PJ. The complement-inhibitory activity of CD59 resides in its capacity to block incorporation of C9 into membrane C5b-9. J Immunol. 1990;144:3478-83. [PMID: 1691760] 14. Stru¨bing P. Paroxysmale haemoglobinurie. Dtsch Med Wochenschr. 1882; 8:1-16. 15. Enneking J. Eine neue form intermittierender haemoglobinurie (haemoglobinuria paroxysmalis nocturia). Klin Wochenschr. 1928;7:2045. 16. Ham T. Chronic hemolytic anemia with paroxysmal nocturnal hemoglobinuria. A study of the mechanism of hemolysisin relation to acid– base equilibrium. N Engl J Med. 1937;217:915-7. 17. Pillemer L, Blum L, Lepow IH, Ross OA, Todd EW, Wardlaw AC. The properdin system and immunity. I. Demonstration and isolation of a new serum protein, properdin, and its role in immune phenomena. Science. 1954;120:27985. [PMID: 13186838] 18. Miyata T, Takeda J, Iida Y, Yamada N, Inoue N, Takahashi M, et al. The cloning of PIG-A, a component in the early step of GPI-anchor biosynthesis. Science. 1993;259:1318-20. [PMID: 7680492] 19. Hillmen P, Hall C, Marsh JC, Elebute M, Bombara MP, Petro BE, et al. Effect of eculizumab on hemolysis and transfusion requirements in patients with paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2004;350:552-9. [PMID: 14762182] 20. Hillmen P, Young NS, Schubert J, Brodsky RA, Socie´ G, Muus P, et al. The complement inhibitor eculizumab in paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2006;355:1233-43. [PMID: 16990386] 21. Low MG, Saltiel AR. Structural and functional roles of glycosyl-phosphatidylinositol in membranes. Science. 1988;239:268-75. [PMID: 3276003] 22. Udenfriend S, Kodukula K. How glycosylphosphatidylinositol-anchored membrane proteins are made. Annu Rev Biochem. 1995;64:563-91. [PMID: 7574493] 23. Kinoshita T, Inoue N. Dissecting and manipulating the pathway for glycosylphos-phatidylinositol-anchor biosynthesis. Curr Opin Chem Biol. 2000;4: 632-8. [PMID: 11102867] 24. Bessler M, Mason PJ, Hillmen P, Miyata T, Yamada N, Takeda J, et al. Paroxysmal nocturnal haemoglobinuria (PNH) is caused by somatic mutations in the PIG-A gene. EMBO J. 1994;13:110-7. [PMID: 8306954] 25. Takeda J, Miyata T, Kawagoe K, Iida Y, Endo Y, Fujita T, et al. Deficiency of the GPI anchor caused by a somatic mutation of the PIG-A gene in paroxysmal nocturnal hemoglobinuria. Cell. 1993;73:703-11. [PMID: 8500164] 26. Takahashi M, Takeda J, Hirose S, Hyman R, Inoue N, Miyata T, et al. Deficient biosynthesis of N-acetylglucosaminyl-phosphatidylinositol, the first intermediate of glycosyl phosphatidylinositol anchor biosynthesis, in cell lines established from patients with paroxysmal nocturnal hemoglobinuria. J Exp Med. 1993;177:517-21. [PMID: 8426120] 27. Ham TH, Dingle JH. Studies on destruction of red blood cells. ii. chronic hemolytic anemia with paroxysmal nocturnal hemoglobinuria: certain immunological aspects of the hemolytic mechanism with special reference to serum complement. J Clin Invest. 1939;18:657-72. [PMID: 16694699] 28. Parker CJ, Baker PJ, Rosse WF. Increased enzymatic activity of the alternative pathway convertase when bound to the erythrocytes of paroxysmal nocturnal hemoglobinuria. J Clin Invest. 1982;69:337-46. [PMID: 6915939] 29. Walport MJ. Complement. First of two parts. N Engl J Med. 2001;344: 1058-66. [PMID: 11287977] 30. Meri S, Morgan BP, Davies A, Daniels RH, Olavesen MG, Waldmann H, et al. Human protectin (CD59), an 18, 000-20, 000 MW complement lysis restricting factor, inhibits C5b-8 catalysed insertion of C9 into lipid bilayers. Immunology. 1990;71:1-9. [PMID: 1698710] 31. Reiter CD, Wang X, Tanus-Santos JE, Hogg N, Cannon RO 3rd, Schechter AN, et al. Cell-free hemoglobin limits nitric oxide bioavailability in sickle-cell disease. Nat Med. 2002;8:1383-9. [PMID: 12426562] 594 15 April 2008 Annals of Internal Medicine Volume 148 • Number 8
32. Rother RP, Bell L, Hillmen P, Gladwin MT. The clinical sequelae of intravascular hemolysis and extracellular plasma hemoglobin: a novel mechanism of human disease. JAMA. 2005;293:1653-62. [PMID: 15811985] 33. Carmichael FJ. Recent developments in hemoglobin-based oxygen carriers—an update on clinical trials. Transfus Apher Sci. 2001;24:17-21. [PMID: 11515606] 34. Azizi E, Dror Y, Wallis K. Arginase activity in erythrocytes of healthy and ill children. Clin Chim Acta. 1970;28:391-6. [PMID: 5450162] 35. Morris CR, Kato GJ, Poljakovic M, Wang X, Blackwelder WC, Sachdev V, et al. Dysregulated arginine metabolism, hemolysis-associated pulmonary hypertension, and mortality in sickle cell disease. JAMA. 2005;294:81-90. [PMID: 15998894] 36. Wiedmer T, Hall SE, Ortel TL, Kane WH, Rosse WF, Sims PJ. Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria. Blood. 1993;82:1192-6. [PMID: 7688991] 37. Hugel B, Socie´ G, Vu T, Toti F, Gluckman E, Freyssinet JM, et al. Elevated levels of circulating procoagulant microparticles in patients with paroxysmal nocturnal hemoglobinuria and aplastic anemia. Blood. 1999;93:3451-6. [PMID: 10233897] 38. Ploug M, Plesner T, Rønne E, Ellis V, Høyer-Hansen G, Hansen NE, et al. The receptor for urokinase-type plasminogen activator is deficient on peripheral blood leukocytes in patients with paroxysmal nocturnal hemoglobinuria. Blood. 1992;79:1447-55. [PMID: 1312369] 39. Maroney SA, Cunningham AC, Ferrel J, Hu R, Haberichter S, Mansbach CM, et al. A GPI-anchored co-receptor for tissue factor pathway inhibitor controls its intracellular trafficking and cell surface expression. J Thromb Haemost. 2006;4:1114-24. [PMID: 16689766] 40. Hartmann RC, Jenkins DE. The “sugar-water” test for paroxysmal nocturnal hemoglobinuria. N Engl J Med. 1966;275:155-7. [PMID: 5938862] 41. van der Schoot CE, Huizinga TW, van’t Veer-Korthof ET, Wijmans R, Pinkster J, von dem Borne AE. Deficiency of glycosyl-phosphatidylinositollinked membrane glycoproteins of leukocytes in paroxysmal nocturnal hemoglobinuria, description of a new diagnostic cytofluorometric assay. Blood. 1990;76: 1853-9. [PMID: 2145990] 42. Hall SE, Rosse WF. The use of monoclonal antibodies and flow cytometry in the diagnosis of paroxysmal nocturnal hemoglobinuria. Blood. 1996;87:5332-40. [PMID: 8652849] 43. Diep DB, Nelson KL, Raja SM, Pleshak EN, Buckley JT. Glycosylphosphatidylinositol anchors of membrane glycoproteins are binding determinants for the channel-forming toxin aerolysin. J Biol Chem. 1998;273:2355-60. [PMID: 9442081] 44. Brodsky RA, Mukhina GL, Nelson KL, Lawrence TS, Jones RJ, Buckley JT. Resistance of paroxysmal nocturnal hemoglobinuria cells to the glycosylphosphatidylinositol-binding toxin aerolysin. Blood. 1999;93:1749-56. [PMID: 10029605] 45. Brodsky RA, Mukhina GL, Li S, Nelson KL, Chiurazzi PL, Buckley JT, et al. Improved detection and characterization of paroxysmal nocturnal hemoglobinuria using fluorescent aerolysin. Am J Clin Pathol. 2000;114:459-66. [PMID: 10989647] 46. Mukhina GL, Buckley JT, Barber JP, Jones RJ, Brodsky RA. Multilineage glycosylphosphatidylinositol anchor-deficient haematopoiesis in untreated aplastic anaemia. Br J Haematol. 2001;115:476-82. [PMID: 11703352] 47. Oni SB, Osunkoya BO, Luzzatto L. Paroxysmal nocturnal hemoglobinuria: evidence for monoclonal origin of abnormal red cells. Blood. 1970;36:145-52. [PMID: 5448520] 48. Hu R, Mukhina GL, Piantadosi S, Barber JP, Jones RJ, Brodsky RA. PIG-A mutations in normal hematopoiesis. Blood. 2005;105:3848-54. [PMID: 15687243] 49. Araten DJ, Nafa K, Pakdeesuwan K, Luzzatto L. Clonal populations of hematopoietic cells with paroxysmal nocturnal hemoglobinuria genotype and phenotype are present in normal individuals. Proc Natl Acad Sci U S A. 1999; 96:5209-14. [PMID: 10220445] 50. Luzzatto L, Bessler M, Rotoli B. Somatic mutations in paroxysmal nocturnal hemoglobinuria: a blessing in disguise? Cell. 1997;88:1-4. [PMID: 9019395] 51. Inoue N, Izui-Sarumaru T, Murakami Y, Endo Y, Nishimura J, Kurokawa K, et al. Molecular basis of clonal expansion of hematopoiesis in 2 patients with paroxysmal nocturnal hemoglobinuria (PNH). Blood. 2006;108:4232-6. [PMID: 16940417] www.annals.org
Physiology of Complement-Related Hemolytic Anemia 52. Wang H, Chuhjo T, Yasue S, Omine M, Nakao S. Clinical significance of a minor population of paroxysmal nocturnal hemoglobinuria-type cells in bone marrow failure syndrome. Blood. 2002;100:3897-902. [PMID: 12393738] 53. Hillmen P, Muus P, Du¨hrsen U, Risitano AM, Schubert J, Luzzatto L, et al. Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria. Blood. 2007;110:4123-8. [PMID: 17702897] 54. Antin JH, Ginsburg D, Smith BR, Nathan DG, Orkin SH, Rappeport JM. Bone marrow transplantation for paroxysmal nocturnal hemoglobinuria: eradication of the PNH clone and documentation of complete lymphohematopoietic engraftment. Blood. 1985;66:1247-50. [PMID: 3904867] 55. Saso R, Marsh J, Cevreska L, Szer J, Gale RP, Rowlings PA, et al. Bone
Review
marrow transplants for paroxysmal nocturnal haemoglobinuria. Br J Haematol. 1999;104:392-6. [PMID: 10050724] 56. Takahashi Y, McCoy JP Jr, Carvallo C, Rivera C, Igarashi T, Srinivasan R, et al. In vitro and in vivo evidence of PNH cell sensitivity to immune attack after nonmyeloablative allogeneic hematopoietic cell transplantation. Blood. 2004;103:1383-90. [PMID: 14525787] 57. Brodsky RA, Young NS, Antonioli E, Risitano AM, Schrezenmeier H, Schubert J, et al. Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria. Blood. 2008;111:1840-7. [PMID: 18055865] 58. Brodsky RA, Jones RJ. Aplastic anaemia. Lancet. 2005;365:1647-56. [PMID: 15885298]
DOWNLOAD IMPORTANT REFERENCES
TO
CITATION MANAGERS
At www.annals.org, article citations may be directly downloaded to any of the following formats: EndNote, Reference Manager, ProCite, BibTeX, or Medlar.
www.annals.org
15 April 2008 Annals of Internal Medicine Volume 148 • Number 8 595