Training in the Aging Athlete Carl Foster, PhD, Glenn Wright, PhD, Rebecca A. Battista, PhD, and John P. Porcari, PhD
Corresponding author Carl Foster, PhD Department of Exercise and Sport Science, 133 Mitchell Hall, University of Wisconsin-La Crosse, La Crosse, WI 54601, USA. E-mail:
[email protected] Current Sports Medicine Reports 2007, 6:200–206 Current Medicine Group LLC ISSN 1537-890x Copyright © 2007 by Current Medicine Group LLC
The number of healthy older individuals who are active in sports has increased significantly during the past generation. These individuals continue to perform at a high level, although there appears to be a loss in functional capacity that cannot be overcome by training. No accepted theory of aging exists, but older athletes may be limited primarily by the inability to maintain the same volume and intensity of training. Also, older athletes appear to respond more slowly to the same training load than do younger athletes. The principles of training in older athletes are similar to those in young athletes; however, additional days of recovery and cross training may be necessary to prevent orthopedic injuries. Strategies for maintaining exercise intensity, including resistance training, are advisable to prevent sarcopenia and selective loss of type II muscle fibers.
Introduction One of the most remarkable aspects of exercise physiology is the ability of tissues, organs, and organ systems to adapt to repetitive stress and improve functional ability. Within the context of an aging society, this adaptability not only provides a means of slowing the functional consequences of the aging process but also provides the underlying rationale for rehabilitation programs designed to allow recovery of functional ability following injury and illness. The watershed event in the history of exercise as a health and fitness adjunct was the publication of Aerobics, by Cooper [1], in 1968. Coupled with the pioneering work of White [2,3] and the first Surgeon General’s report on the heath consequences of smoking, the number of adults performing exercise for health and fitness or for competition increased rapidly beginning in the late 1960s. This phenomenon led, inevitably, to a rapid increase in the number of individuals suffering from adverse health consequences
related to their increased activity levels, as evidenced in the number of reports of exertion-related myocardial infarction and sudden death, which led in turn to the hypothesis that exercise can serve as a trigger for myocardial infarction in the presence of underlying cardiovascular disease [4–8]. The risk of both catastrophic and musculoskeletal injuries in a growing number of adult exercisers also contributed to the rapid growth of the American College of Sports Medicine (ACSM) in the early 1970s. A benefit from this increased interest in exercise among middle-aged and older individuals has been a better understanding of the physiologic characteristics of older athletes and of the training response in general. This outcome offers the possibility not only for increased levels of healthy participation in competitive sports by older athletes but also improved training effectiveness for all individuals. At the same time, the increased number of older individuals training at levels beyond those required for basic fitness presents medical and fitness practitioners with the challenge of providing guidance to this population. These individuals may be training in the presence of underlying pathologies, may respond to training more slowly, and may be more subject to injuries than are younger athletes. This article reviews general theories of aging, the performance characteristics of older athletes, the basic principles of training, and training responses in older individuals (particularly athletes) as well as suggesting strategies for optimizing the training of older athletes.
Theories of Aging No widely accepted theory exists showing the ultimate cause or causes of aging. From the standpoint of exercise, evidence from studies in a number of species suggests that the level of spontaneous activity decreases progressively with aging [9,10]. This progression is often associated with a marked sarcopenia, particularly loss in type II muscle fibers [11•]. Leading hypotheses include the progressive accumulation of DNA damage (perhaps related to oxygen free radical exposure), progressive accumulation of microtrauma leading to fibrotic changes in various tissues and organ systems, and development of subclinical pathologies (particularly atherosclerotic cardiovascular disease). Evidence exists for age-related mutations and deletions of mitochondrial DNA [12,13], general reductions in tran-
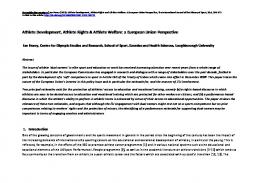
Training in the Aging Athlete Foster et al. 201 Figure 1. Schematic pattern (based on data from multiple sources) of decreases in best performances by age in running (10-km), swimming (1500-m), and weight lifting. Closed symbols represent men, and open symbols represent women. With the exception of swimming, the loss in performance is typically somewhat more rapid in women. It is unclear whether this is a primary sexrelated difference or related to the smaller relative participation rate by women. After age 60, the rate of deterioration may increase in both men and women.
100
World record, %
90 80 70 60
Men 10-km run Women 10-km run Men 1500-m swim Women 1500-m swim Men weight lift Women weight lift
50 40 30 20 20
30
40
50 Age
60
70
80
Sports Medicine Reportsheavy SR06-3-2-04 1 script levels, and Current synthesis rates of myosin chains fig. Principles of Training 324 pts. W/ 192 pts. D (27 x 16) in older individuals, potentially related to the progressive The fundamental paradigm of exercise training is conAuthor: Foster Editor: Michele Artist: Dan reductions in androgen concentrations (at least in men) tained in the story of the semi-legendary Milo of Crotona. [12–16]. Evidence also suggests that post-transcriptional Milo was the farm boy who was so proud of a newly suppression of protein synthesis may take place in older foaled bullock that he carried it around the farm yard individuals. Alternatively, given that a higher propensity every day. As the calf grew heavier, Milo became stronger, for injury limits the volume and intensity of training that until he became the strongest man in the world and one of older athletes can tolerate, the training response in older the great champions of the original Olympic games. This athletes may be limited by nothing more than the inability story led to the principle of progressive overload (increasof older athletes to tolerate heavy training loads. From a ing training load gradually to continuously challenge molecular perspective, the reduced training load that can adaptations in strength), the cornerstone of the theory of be tolerated by older individuals can be viewed as a limita- exercise training. tion in the molecular signaling for adaptation. Our understanding of the training response is dependent on the availability of a widely accepted outcome measure, or marker, to establish when training Performance Trends in Relation to Age has occurred. This model was provided in 1968 when Tanaka and Seals [17] have presented an elegant analysis the World Health Organization recognized the maxiof performance losses in relation to age in master athletes, mal oxygen uptake (VO2 max) as essentially equivalent including both cross-sectional and longitudinal data. to endurance [20]. The presence of VO2 max as a widely This pattern of deterioration is also depicted schemati- accepted outcome measure led to an extensive series of cally in Figure 1. Little loss in performance ability has studies in the 1970s, primarily by Pollock and Wilmbeen documented in athletes before they reach their mid ore, in which the effects of various permutations of 30s, although athletes commonly report more difficulty training (frequency, intensity, and time) on the increase in avoiding injury or persistent problems related to prior in VO2 max in previously sedentary young and middleinjuries as early as their late 20s and early 30s. From the aged adults were examined [21]. Subsequent studies, mid 30s to about the age of 60 years, a slow but progres- primarily by Hickson, using controlled reductions of sive loss occurs in performance ability. Beyond the age of training, have confirmed the impressions derived from 60 years, an accelerated loss in performance ability has training onset studies [22–24]. These studies, along been observed even in athletes who are able to main- with others from the same generation, have been well tain training volume and intensity. A larger decrement integrated in the recommendations of the ACSM [25]. is apparent in the performance of female athletes, the Other guidelines, such as those by Kraemer et al. [26], cause of which is unclear. Given the loss of the anabolic present the overriding principles of resistance trainhormone-related advantage of men with aging, common ing, although the absence of an agreed-upon outcome sense would argue that men and women would respond measure for muscular performance has led to a lack of in a more similar manner to training as they age. That agreement. Although we now recognize that there is this is not the case, and that women actually deteriorate more to endurance training than changes in VO2 max more than men, remains a topic of research interest. Simi- [27], the use of changes in VO2 max as a marker of the lar findings have been observed for weight lifting, power training response has been helpful for a generation and lifting [18], and rowing [19]. retains much of its intrinsic validity.
202 Training
The response to training generally follows the same saturation curve in relation to dosage that might be expected from pharmaceutical agents. A clear minimal level of training is required to provoke adaptations, which is highly related to the characteristics of the individual who is training (less fit individuals respond at a lower dosage of training). Side effects of training, likewise, follow an accelerating pattern in relation to training load. Recent studies have demonstrated that the integrated product of training frequency, intensity, and time (ie, training load) provokes the same type of response to training as demonstrated for the individual elements of training [28,29]. Very heavy training loads, as often accomplished by athletes, often lead to a paradoxic and persistent decrease in performance (overtraining syndrome). This complex issue, reviewed recently by Meeusen et al. [30], is clearly related to failures in the recovery aspect of the training program. Recent evidence demonstrates enhanced responses to alternating days of hard and easy training compared with equivalent training performed with a more consistent pattern [31]. Coupled with the effect of training monotony on the likelihood of developing overtraining syndrome [32], this pattern suggests that the process of periodizing (systematic alteration in the training load) is fundamentally sound.
Training Issues Relevant to Older Athletes In 1998, ACSM published a position paper concerning exercise and physical activity for older adults [33]. However, this document focused largely on the health benefits of increased physical activity by sedentary older adults rather than the needs of athletes. Several issues related to older athletes affect their response to training, including 1) the presence of underlying pathologies independently related to age; 2) the presence of residual injuries; 3) reduced hormonal concentration, which affects the rapidity and magnitude of the response to exercise; and 4) the need for longer recovery times from hard training bouts in older individuals. Additional factors affecting older individuals include the lack of available time for training and competition and a reduced drive to achieve performance excellence due to characterization of sport as a recreational activity (even among elite competitors), as compared with younger athletes.
Changes in VO2max
Three major longitudinal studies have evaluated changes in VO2max in aging adult athletes. The first is an older study of champion runners from the 1940s and 1950s as they enter middle age, conducted by Dill et al. [34]. The second reports follow-up results in former American championship and world class athletes after 22 years, as the athletes entered middle age [35–38]. The third study is a 20-year follow-up of former masters champions as they enter into old age [39–41]. Following studies of the best
American distance runners in the late 1960s through mid 1970s, Trappe et al. [35,36] and Widrick et al. [37,38] reported 22-year follow-up data suggesting that athletes who maintained high exercise training intensity had a smaller decrease in VO2max than did those who decreased their training intensity. However, the overall rate of decrease in VO2max was comparable with or larger than norms for sedentary populations. In a companion group of highly fit older individuals who were not elite athletes but who continued to train at fairly high intensity, a significant decrease in VO2max was documented beyond the age of 60 years. Following a cross-sectional study of champion track athletes aged from 40 to 75 years, which demonstrated elevated physiologic values compared with those of control subjects, a significant decline was observed after age 60 [39]. Pollock et al. [39–41] reported follow-up results for these subjects after 10 and 20 years. Athletes who maintained high or moderate training intensity showed decreases in VO2max that were parallel to cross-sectional norms though still at higher absolute values than in sedentary control subjects. Athletes who reduced their training to lower intensity, consistent with fitness recommendations, showed comparatively large decreases in VO2max (particularly after age 60) to values typical of active but not athletic age-matched individuals. The results of both of the contemporary studies are consistent with the concept that regular high-intensity training is necessary to allow maintenance of high VO2max values across age. These results are reflected in several other smaller series of studies with aging athletes [42,43]. This pattern of response, in which athletes who might, at a common sense level, be expected to age relatively more slowly than sedentary individuals, is well explained in the work of Tanaka and Seals [17]. Athletes—even those who are still training at the highest possible intensity of exercise—will actually decrease the volume and intensity of their training substantially. Thus, the stimulus (signaling) to maintain VO2max is actually substantially reduced in those who are initially the most active. Particularly considering the substantial effect of reductions in training intensity evident in the studies of Hickson et al. [24], the tendency for older athletes to reduce training intensity seems to be an adequate explanation for the functional losses observed in the longitudinal studies of athletes. Thus, strategies for maintaining exercise intensity may be the key to minimizing the loss of functional ability as athletes age.
Changes in Body Composition The longitudinal study by Pollock et al. [40,41] provided evidence of the tendency of older athletes to lose lean body mass and, as a result, to become fatter even as they continue to train. In this study, some athletes succeeded in resisting the tendency to lose muscle mass. They were, uniformly, performing resistance exercise to supplement
Training in the Aging Athlete Foster et al. 203
their primarily aerobic training or were sprint athletes who were using resistance training to augment their running performance. This pattern, which is also evident in the longitudinal data of Trappe et al. [35,36] and Widrick et al. [37,38], suggests the importance of circulating hormone concentrations to the preservation of lean body mass, at least in male athletes. Recent evidence [44] indicates that elderly men have similar relative testosterone responses to high-intensity resistance training as do young men, albeit at a lower absolute level. Thus, the pattern of hormonal responses to training is capable of supporting the transcriptive upregulation that is characteristic of the training response, although the magnitude of the transcriptive response in relation to a given level of signaling is likely to be smaller in older athletes. These data support the concept of resistance training as an important countermeasure against the sarcopenia of aging.
Changes in Skeletal Muscle The sarcopenia of aging, including that in older athletes, is probably attributable to reductions in type IIa and IIb fibers [45,46]. These changes may be a function of reductions in activity, particularly high-intensity training; neuromuscular function [47]; or hormone concentrations [16,48]. Deterioration of motor end-plate structures, deficits in excitation-contraction coupling, and decreased motor unit recruitment may be other factors [49]. Collectively, these changes may be viewed under the rubric of motor unit “remodeling,” which includes denervation of type II fibers and the re-innervation of type I fibers due to synaptic changes at the neuromuscular junction [47]. This process may be caused by progressive loss of motor neurons. Accordingly, fibers innervated by larger motor neurons may become progressively denervated or be innervated by smaller (type I) neurons. However, because most of the data are cross-sectional rather than longitudinal, it is unclear whether this trend toward a reduction in type II muscle fibers is related to changes in activity level or is a primary effect of aging. Training studies in older individuals have indicated an attenuated training response compared with that of younger individuals, although the differences in the hypertrophic response do not seem to be attributable to differences in myogenic regulatory factors [50]. The difference in the hypertrophic response appears to relate to a suppression of transcript levels induced by exercise [51]. However, despite an attenuated response to training, older individuals show both neuromuscular and hypertrophic responses [52], including selective growth of the type II fibers, which are most at risk during aging [49]. Beyond the direct changes in skeletal muscle that occur during aging, which are to some degree countered by exercise, changes also occur in the connective tissue, best characterized by the loss of tendon stiffness, which reduces the efficiency of the transfer of muscle forces to the
skeleton. Recent evidence suggests that tendon stiffness increases after training [53]. Whether these adaptations observed in training studies of sedentary individuals apply to athletes remains to be determined.
Optimizing Training in Older Athletes Optimal training in older athletes is fundamentally similar to optimal training in younger athletes. Ample evidence indicates that older athletes may need relatively more recovery [11•,50], which suggests that the frequency of either high-intensity or high-volume training might need to be reduced, compared with training in younger athletes. In essence, the periodization cycle for older athletes may need to be longer than that normally used by younger athletes (Fig. 2). However, recent evidence suggests that less frequent but heavier training per training day may be optimal even for young individuals [31]. Furthermore, compelling evidence indicates that even young athletes respond best when they have two to three very hard training sessions per week, with the larger volume of training performed on recovery days. This approach is designed to allow for recovery/repair and increase the amount of heavy training that can be tolerated on hard training days [28,31,54] Given the pattern of losses in VO2max and muscle mass (specifically type II fibers), it probably makes sense to include as much high-intensity training as possible, because high-intensity training is more provocative of supporting VO2max, is more likely to lead to preservation of muscle mass, and is more likely to be associated with recruiting type II fibers. However, prolonged high-intensity training is often quite uncomfortable, is associated with large disturbances in homeostasis that older athletes may avoid due to lower motivation, and may contribute to the risk of catastrophic events in individuals with underlying cardiovascular disease [4–8]. Evidence exists showing that brief high-intensity interval training may be tolerated even in clinical populations [55]. Accordingly, brief (30 sec) interval training at intensities approximating the VO2max (which is likely to recruit type II muscle fibers) might be particularly useful in older athletes. Training with a pattern of 30 sec/60 sec high versus low intensity has been shown to be tolerated well in patients with cardiovascular disease, including those with chronic heart failure severe enough to require cardiac transplantation, and may be a viable technique in older athletes. Similarly, strategies that make resistance training more tolerable without decreasing the absolute intensity of training might be useful for preserving muscle mass and type II muscle fibers without being dangerous or onerous. For example, performing two sets of five repetitions with a resistance that might ordinarily be limiting at one set of 10 repetitions might allow appropriate recruitment of type II muscle fibers without the discomfort associated with more all-out resistance training. Assuming
204 Training
1000
Young athletes
Training load
750
500
250
0 1
8
15
22
1000
29 Days
36
43
50
36
43
50
Older athletes
Training load
750
500
250
0 1
8
15
22
29 Days
Figure 2. Schematic periodization plan in younger and older athletes preparing for the same competition (eg, 10-km run). Note that Current Sports Medicine Reports fig.week. 2 the younger athletes are on a cycle of 3 progressively harder weeks, followedSR06-3-2-04 by a recovery Within each week are three hard 492 pts. 384 pts.and D duration (41x 32) of that day’s training. For the most part, recovery training sessions, which may be achieved by manipulating theW/ intensity Author: Foster Editor: Michele Artist: Danharder weeks followed by a recovery week. training is mode specific (eg, running). The older athletes are on a cycle of 2 progressively Within each week there are only two hard training sessions. Note that, with allowances for a slightly slower rate of progression in the older athletes, the hard workouts are very similar between younger and older athletes. Although most if not all of the training by the younger athletes is mode specific, in the older athletes recovery training 2 to 3 days a week should be in an alternative mode (eg, cross training) in order to augment recovery.
that the usual recommendation for resistance training in young individuals is three times weekly, the additional recovery required by older athletes might be provided by limiting training to twice weekly or by taking more frequent recovery weeks. In younger athletes, the low specificity of cross training (~ 25% in non-muscularly similar and ~ 50% in muscularly similar activities) makes it less desirable for training during the primary portion of the competitive year [56,57]. Cross training is, therefore, primarily useful during periods of active recovery and during recovery following injury. However, in older athletes, in whom microtrauma resulting from either prolonged or high-intensity specific training might require several days of recovery, cross training may be particularly valuable. Cross training, used as a strategy to avoid orthopedic stress, may be more helpful than the
strategy of low-intensity training between heavy training sessions used by younger athletes. For endurance athletes, resistance training may contribute directly to improved performance [58], further supporting the value of cross training. This pattern is also reflected in the improved walking tolerance observed after resistance training in sedentary individuals. If strength is the primary goal of training, the addition of endurance training may interfere with strength development [59].
Conclusions Older individuals represent an increasing number of athletic participants. The problems faced by older athletes can be summarized as the accumulation of residual injuries that limit the volume and intensity of training
Training in the Aging Athlete Foster et al. 205
they can tolerate and may reduce their potential for responsiveness to training. This pattern leads to reductions in VO2 max and to sarcopenia, particularly loss of type II muscle fibers. The losses in functional ability seem to be particularly noticeable after 60 years of age, even in individuals who can maintain a relatively high level of training into the seventh decade. Training strategies should be focused on training patterns that allow much more recovery between hard training sessions or hard training weeks, on maintaining high-intensity training potentially by shortening the duration of hard segments (for example 30 sec/60 sec vs 3:00/6:00 in young endurance athletes), and on resistance training to preserve muscle mass. To minimize the orthopedic stress of training, cross training might be particularly useful in older athletes, especially during training performed for recovery between high-intensity or highvolume specific training.
References and Recommended Reading Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
14.
15. 16. 17.
18. 19. 20.
21. 22. 23. 24.
1.
Cooper KH: Aerobics. Garden City, NJ: Ballentine Books; 1968. 2. White P: The pulse after a marathon race. JAMA 1918, 71:1047–1048. 3. White P: Bradycardia (below rate of 40) in athletes, especially long distance runners. JAMA 1942, 120:642. 4. Thompson PD: Historical concepts of the athlete’s heart. Med Sci Sports Exer 2004, 36:363–370. 5. Waller BF, Roberts WC: Sudden death while running in conditioned runners aged 40 years or over. Am J Cardiol 1980, 45:1292–1300. 6. Siscovick DS, Weiss NS, Fletcher RH, Lasky T: The incidence of primary cardiac arrest during vigorous exercise. N Engl J Med 1984:874–877. 7. Mittleman MA, Maclure M, Tofler GH, et al.: Triggering of acute myocardial infarction by heavy physical exertion. N Engl J Med 1993, 329:1677–1683. 8. Willich SN, Lewis M, Lowel H, et al.: Physical exertion as a trigger of acute myocardial infarction. N Engl J Med 1993, 329:1684–1690. 9. Holloszy JO, Smith ER, Vining M, Adams S: Effect of voluntary exercise on longevity of rats. J Appl Physiol 1985, 59:828–831. 10. Himann JE, Cunningham DA, Rechnitzer PA, Patterson DH: Age related changes in speed of walking. Med Sci Sports Exerc 1988, 20:161–166. 11.• Hunter GR, McCarthy JP, Bamman MM: Effects of resistance training on older adults. Sports Med 2004, 34:329–348. Excellent review of causes of sarcopenia and exercise countermeasures. 12. Melov S, Shoffner JM, Kaufman A, Wallace DC: Marked increase in the number and variety of mitochondrial DNA rearrangements in aging human skeletal muscle. Nucleic Acids Res 1995, 23:4122–4126. 13. Sohal RS, Weindruch R: Oxidative stress, caloric restriction and aging. Science 1996, 273:59–63.
25.
26. 27.
28.
29. 30. 31. 32. 33. 34. 35.
Balagopal P, Schimke JC, Ades P, et al.: Age effect on transcript levels and synthesis rate of muscle MHC and response to resistance exercise. Am J Physiol Endocrinol Metab 2001, 280:E203–E208. Hameen M, Harridge SDR, Goldspink G: Sarcopenia and hypertrophy: a role for insulin like growth factor-1 in aged muscle. Exerc Sport Sci Rev 2002, 30:15–19. Lamberts SW, van den Beld AW, van der Lely AJ: The endocrinology of aging. Science 1997, 278:419–424. Tanaka H, Seals DR: Dynamic exercise performance in masters athletes: insight into the effects of primary human aging on physiological functional capacity. J Appl Physiol 2003, 95:2152–2162. Anton MM, Spirduso WW, Tanaka H: Age-related declines in anaerobic muscular performance: weightlifting and powerlifting. Med Sci Sports Exer 2004, 36:143–147. Seiler KS, Spirduso WW, Martin WC: Gender differences in rowing performance and power with aging. Med Sci Sports Exerc 1998, 30:121–127. Shephard RJ, Allen C, Benade AJS, et al.: The maximum oxygen intake: an international reference standard of cardiorespiratory fitness. Bull Wld Hlth Org 1968, 38:757–764. Pollock ML: The quantification of endurance training programs. In Exercise and Sport Sciences Reviews. Edited by Wilmore JH. New York: Academic Press; 1973:155–188. Hickson RC, Rosenkoetter MA: Reduced training frequencies and maintence of increased aerobic power. Med Sci Sports Exerc 1981, 13:13–16. Hickson RC, Kanakis C, Davis JR, et al.: Reduced training duration effects on aerobic power, endurance and cardiac growth. J Appl Physiol 1982, 53:225–229. Hickson RC, Foster C, Pollock ML, et al.: Reduced training intensities and loss of aerobic power, endurance and cardiac growth. J Appl Physiol 1985, 58:492–499. Pollock ML, Gaesser GA, Butcher JD, et al.: The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness and flexibility in healthy adults. Med Sci Sports Exerc 1998, 30:975–991. Kraemer WJ, Cafarelli E, Dudley GA, et al.: Progression modules in resistance training for healthy adults. Med Sci Sports Exerc 2002, 34:364–380. Meyer T, Lucia A, Earnest CP, Kindermann W: A conceptual framework for performance diagnosis and training prescription from submaximal parameters—theory and application. Int J Sports Med 2005, 26:1–11. Foster C, Daniels JT, Seiler KS: Perspectives on correct approaches to training. In Overload, Performance Incompetence and Regeneration in Sport. Edited by Lehmann M, Foster C, Gastmann U, Keizer H, Steinacher J. New York: Plenum Press; 1999:27–41. Foster C, Daines E, Hector L, et al.: Athletic performance in relation to training load. Wisc Med J 1996, 95:370–374. Meeusen R, Duclos M, Gleeson M, et al.: Prevention, diagnosis and treatment of the overtraining syndrome. Eur J Sport Sci 2006, 6:1–14. Hansen AK, Fischer CP, Plomgaard P, et al.: Skeletal muscle adaptation: training twice every second day vs training once daily. J Appl Physiol 2005, 98:93–99. Foster C: Monitoring training in athletes with reference to overtraining syndrome. Med Sci Sports Exerc 1998, 30:1164–1168. Mazzeo RA, Cavanagh P, Evans WJ, et al.: Exercise and physical activity for older adults. Med Sci Sports Exerc 1998, 30:992–1008. Dill DB, Robinson S, Ross JC: A longitudinal study of 16 champion runners. J Sports Med Phys Fitness 1967, 7:4–27. Trappe SW, Costill DL, Fink WJ, Pearson DR: Skeletal muscle characteristics among distance runners: a 20-yr follow-up study. J Appl Physiol 1995, 78:823–829.
206 Training 36. 37.
38.
39. 40. 41. 42. 43. 44.
45. 46.
47.
Trappe SW, Costill DL, Vukovich MD, et al.: Aging among elite distance runners: a 22yr longitudinal study, J Appl Physiol 1996, 80:285–290. Widrick JJ, Trappe SW, Blaser CA, et al.: Isometric force and maximal shortening velocity of single muscle fibers from elite master runners Am J Physiol 1996, 271: C666–C675. Widrick JJ, Trappe SW, Costill DL, Fitts RH: Force velocity and force power properties of single muscle fibers from elite master runners and sedentary men. Am J Physiol 1996, 271: C676–C683. Pollock ML, Miller HS, Wilmore J: Physiological characteristics of champion American track athletes 40–75 years of age. J Gerontol 1974, 29:645–649. Pollock ML, Foster C, Knapp D, et al.: Effect of age and training on aerobic capacity and body composition of master athletes. J Appl Physiol 1987, 62:725–731. Pollock ML, Mengelkoch LJ, Graves JE, et al.: Twenty-year follow-up of aerobic power and body composition of older track athletes. J Appl Physiol 1997, 82:1508–1516. Kasch FW, Boyer JL, Schmidtg PK, et al.: Aging of the cardiovascular system during 33 years of aerobic exercise. Age Ageing 1999, 28:531–536. Rogers MA, Hagberg JM, Martin WH, et al.: Decline in VO2max with aging in master athletes and sedentary men. J Appl Physiol 1990, 68:2195–2199. Baker JR, Bemben MG, Anderson MA, Bemben DA: Effects of age on testosterone response to resistance exercise and musculoskeletal variables in men. J Strength Cond Res 2006, 20:874–881. Proctor DN, Dalagopal P, Pair KP: Age related sarcopenia in humans is associated with synthetic rates of specific muscle proteins. J Nutr 1998, 273:E790–E800. Kim JS, Dosek DJ, Petrella JK, et al.: Resting and load induced levels of myogenic gene transcripts differ between older adults with demonstrable sarcopenia and young men and women. J Appl Physiol 2005, 88:2149–2158. Brooks SV, Faulkner JA: Skeletal muscle weakness in old age: underlying mechanisms. Med Sci Sports Exerc 1994, 26:432–439.
48.
49. 50.
51.
52. 53. 54.
55.
56. 57. 58. 59.
Kostka T, Arsac LM, Patricot ML, et al.: Leg extension power and dehydroepiandosterone sulfate, insulin like growth factor I, and testosterone in healthy active elderly people. Eur J Appl Physiol 2000, 82:83–90. Aoyagi Y, Shephard RJ: Aging and muscle function. Sports Med 1992, 14:376–396. Kosek DJ, Kim JS, Petrella JK, et al.: Efficiency of 3 days/week resistance training on muscular hypertrophy and myogenic mechanisms in young and older adults. J Appl Physiol 2006, 101:531–544. Balagopal P, Schimke JC, Ades P, et al.: Age effect on transcript levels and synthesis rate of muscle MHC and response to resistance exercise. Am J Physiol Endocrin Metab 2001, 280:E203–E208. Tracy BL, Ivey FM, Hurlbut D, et al.: Muscle quality II: Effects of strength training in 65 to 75 yr old men and women. J Appl Physiol 1999, 86:195–201. Reeves ND, Narici MV, Maganaris CN: Myotendinous plasticity to ageing and resistance exercise in humans. Exp Physiol 2005, 91:483– 498. Seiler KS, Kjerland GO: Quantifying training intensity distribution in elite endurance athletes: Is there evidence for an optimal distribution. Scand J Med Sci Sports 2007, in Press. Meyer K, Foster C, Georgakopoulous N, et al.: Left ventricular function during interval and steady state exercise in patients with chronic heart failure. Am J Cardiol 1998, 82:1382–1387. Foster C, Hector L, Wlesh R, et al.: Effects of specific versus cross-training on running performance. Eur J Appl Physiol 1995, 70:367–372. Loy SF, Holladd GJ, Mutton DK, et al.: Effects of stair climbing vs run training on treadmill and track running performance. Med Sci Sports Exerc 1993, 25:1275–1278. Hickson RC, Dvorak BA, Gorostiga EM, et al.: Potential for strength and endurance training to amplify endurance performance. J Appl Physiol 1988, 65:2285–2290. Hickson RC: Interference of strength development by simultaneously training for strength and endurance. Eur J Appl Physiol 1980, 45:255–263.