Objectives: To investigate the accuracy of 2DCT orthoradial reformatted images from spiral computed tomography (CT) for pre-surgical planning of dental ...
Dentomaxillofacial Radiology (1998) 27, 329 ± 333 ã 1998 Stockton Press All rights reserved 0250 ± 832X/98 $12.00 http://www.stockton-press.co.uk/dmfr
Validation of spiral computed tomography for dental implants MGP Cavalcanti1,2, J Yang3, A Ruprecht2,4 and MW Vannier2 1
Department of Radiology, Faculty of Odontology, University of SaÄo Paulo, Brazil; 2 Department of Radiology, College of Medicine, University of Iowa, USA.; 3Division of Oral Radiology, Department of Oral Medicine, Temple University School of Dentistry, USA; 4 Department of Oral Pathology, Radiology, and Medicine, College of Dentistry, University of Iowa, USA
Objectives: To investigate the accuracy of 2DCT orthoradial reformatted images from spiral computed tomography (CT) for pre-surgical planning of dental implants in proximity to the mental foramen. Methods: Eight cadaver heads were imaged by spiral CT (S/Xpress, Toshiba - America, Tustin, CA) with 1 mm thick axial slices by 1 mm/sec of table feed. The image data set was transferred to a networked computer workstation. Using computer graphics the data was analysed with 2D orthoradial reformatting using the ToothPix2 (Cemax, Fremont, CA, USA) protocol. Linear measurements were made by two oral radiologists independently from the superior border of the mental foramen to the crest of the alveolar process and from the inferior border of the mental foramen to the mandibular inferior border. The soft tissues were removed and physical measurements made using a 3 Space2 (Polhemus, Colchester, VT) electromagnetic digitizer with a personal computer running Windows1 95. Results: The dierences between the measurements on orthoradial 2DCT images and the physical measurements were not statistically signi®cant (P40.05). Conclusions: Two-dimensional spiral CT imaging allows highly accurate measurements for dental implant placement in proximity to the mental foramen. Computer graphics software, using reformatted reconstruction, is suitable for implant planning. Keywords: tomography, X-ray computed; dental implantation; mandible; image processing, computer-assisted
Introduction Implant placement is a rapidly growing component of dental practice. Accurate dental implant placement requires comprehensive pre-operative radiographic examination. In the mandible, accurate localization of the mental foramen is necessary. It has been demonstrated that CT provides better visualization of this structure than other radiographic methods1 ± 3. Axial scanning with reformatted cross-sectional images has been advocated by some authors as the method of choice for pre-implant radiographic evaluation.1,2,4 ± 6 Spiral CT represents the latest technological advance in CT imaging. It involves simultaneous translatory movement of the patient while the X-ray source rotates, so that continuous data acquisition and
Correspondence to: Dr M Cavalcanti, Department of Radiology, University of Iowa Hospitals and Clinics, 200 Hawkins Dr., Iowa City, IA 52242, USA Received 20 April 1998; accepted 13 July 1998
archiving occurs as the entire volume of interest is scanned. Special algorithms allow multiplanar computer-reformatted two-dimensional (2D), three-dimensional (3D) and panoramic reconstructions. Our goal was to determine the accuracy (validity) of 2D images reformatted from spiral CT, using a desktop workstation, for pre-surgical planning of dental implants related to the mental foramen. Materials and methods The study was based on eight cadaver heads (®ve males and three females), ages between 60 and 70 years, provided by the Department of Anatomy and Cell Biology of the College of Medicine, The University of Iowa. All specimens were edentulous posterior to the mental foramen. The heads were examined in a spiral CT scanner (Xpress S/X, Toshiba-America Medical System Inc., Tustin, CA, USA) beginning superior to vertex and extending inferiorly to below the mandible.
Spiral CT MGP Cavalcanti et al
330
software facilitates interactive visualization, measurement and analysis of the images generated. Twodimensional reconstruction provides detail of the anatomical structures involved. This 2D volumetric rendering can be used for the quantitative analysis of complex craniofacial fractures and to evaluate treatment.7 Placing implants into the mandible requires accurate diagnostic information to avoid damaging vital anatomical structures. Standard 2D radiographs, such as panoramic views, because they are unable to generate cross-sectional images of the alveolar ridge, do not provide information on bone thickness or the location of vital structures in a buccal-lingual direction.3,4 As well, radiographic images obtained with traditional panoramic systems may be magni®ed by as much as 30%.2 Consequently, one must know the magni®cation factor for an area of interest in order to make accurate measurements. Lam et al4 compared panoramic radiography and orthoradially reformatted
High-resolution, 1 mm thick axial slices were obtained with 1 mm/sec table feed at 120 kVp and 150 mA. A low frequency ®lter cut-o was used in the reconstruction algorithm. The FOV was 20.3 cm, (5126512 matrix). The archived CT data were originally stored on optical disks (Imation Optical, 3M, rewritable optical disk, Imation Enterprises Corporation, Oakdale, MN, USA), to allow full retrospective review of any image. The image was transferred to a networked computer workstation (Sun Microsystems, Mountain View, CA, with VIP version 1.4 software, Cemax, Fremont, CA, USA), to generate 2D reformatted volumetric images. The ToothPix2 (Cemax) software protocol was used for subsequent image manipulation and analysis. The resulting 2D images represented 2 mm thick orthoradial slices through the buccal and lingual cortices of the mandible. Linear measurements, with a caliper, were made by two oral radiologists (MC, JY), independently, from the superior border of the mental foramen to the crest of the alveolar process, and from the inferior border of the mental foramen to the inferior border of the mandible, bilaterally. In total, 64 measurements were made. The soft tissues were subsequently removed, and the same measurements were repeated using a 3 Space2 electromagnetic digitizer (Polhemus, Colchester, VT, USA) with a 486 personal computer (IBM, Armonk, NY, USA) and Windows1 95 (Microsoft, Redmond, WA, USA). Student's paired t-test for unequal measurements was used for statistical analysis which was performed with SAS 6.09 (Statistical Analysis Systems, Institute Inc., Cary, NC, USA).
a
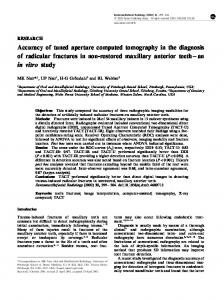
Results Figure 1 shows the relationship between the two sets of measurements made on the 2DCT reconstructions and the physical measurements. Note the relatively small deviation. This is con®rmed in Table 1. The dierences between the measurements were not statistically signi®cant: for the distance between the alveolar crest and the superior border of the mental foramen (P=0.9) and for the inferior border of the mental foramen and the inferior border (P=0.7).
b
Discussion Figure 1 Scatter plot of the imaging and physical measurements (mm) of the distances from (a) the superior border of the mental foramen to the alveolar crest, and (b) the inferior border of the mental foramen to the inferior border of the mandible
Computer-generated reformatted images of craniofacial anatomy can be obtained from spatially mapped CT data. The development of suitable hardware and
Table 1 Difference between the 2DCT and physical measurements on eight cadavers of the distance from the mental foramen to the alveolar crest and the inferior border of the mandible (P=0.05 for significance) Measurement Ms-Ac Mi-Ib
Mean*
s.d.
s.e.
t
df
P
0.94 0.98
1.91 2.31
0.47 0.73
0.120 0.380
28.3 29.9
0.9 0.7
Ms=Superior border of the mental foramen; Mi=Inferior border of the mental foramen; Ac=Alveolar crest; Ib=Inferior mandibular border; *Mean (mm) of the sum of the dierences between the physical and imaging measurements on all eight of the specimens
Spiral CT MGP Cavalcanti et al
a
a
b
b
Figure 2 Photograph showing the use of the 3 Space2 electromagnetic digitizer for measurements on the cadaver heads of the (a) crest of the alveolar process to the superior border of mental foramen, and of the (b) inferior mandibular border to the inferior border of the mental foramen. The arrows indicate the four sites used for the measurements
Figure 3 2DCT reformatted axial views using the ToothPix2 protocol showing the location of orthoradial cross-sectional slices in the mandible. The arrows indicate the slices at the mental foramen selected for the cross-sectional images in Figure 4a and b
Figure 4 2D spiral orthoradially reformatted CT images show in cross-section the relationship of the superior border of the mental foramen to alveolar crest (a) and of the inferior border of the mental foramen to the inferior mandibular border (b) on (a) the right side, and on (b) the left side. The arrows indicate the four sites used for the measurements
331
Spiral CT MGP Cavalcanti et al
332
conventional CT of the jaws and found a statistical dierence in mean bone height between the techniques. Similarly, Todd et al8 compared linear tomography with CT for use with dental implants and found a magni®cation of 28% for linear tomography, in comparison with 4% with CT. Due to these limitations, we believe that neither panoramic radiography nor standard tomography is acceptable in surgical treatment planning for dental implantation. CT equipped with speci®c software designed for implantology can be used to determine the suitability of bone and speci®c sites for implant placement, the size of the implant that can be placed, and the need for pre-implantation ridge surgery. The osseous architecture and the positions of speci®c anatomical structures can be seen clearly. Using interactive software for reformatted CT, it is possible, in the mandible, to determine the distance between the alveolar crest and the mental foramen and inferior alveolar canal. With this technique, the radiologist can determine for the surgeon the exact amount of bone that must be removed or added, and the distance between the implant and vital structures.5 Several other authors have recommended that, for dental implant planning, CT is the method of choice.4,9 ± 11 Most of these articles have been based on use of conventional CT. In 1995 Luka et al12 studied patients using a dental imaging program and spiral CT with a collimation of 1 mm, and a table feed of 1 mm/sec. They stated that only in the 2D reformatted technique could the mandibular canal and mental foramen be identi®ed. It is generally agreed that spiral CT allows faster scanning, thereby decreasing the problem of patient movement during the data acquisition which has resulted in problems with image reconstruction and distortion in the ®nal results. Also, spiral CT allows more resolution in the generated images.13 Images of cadaver heads were measured in simulated implant situations, and validated it by making physical measurements of the same distance on the dissected
specimens with an electromagnetic digitizer (Figure 2). This device has previously been validated by Hildebolt and Vannier,14 as well as by several other researchers.15 ± 17 The mental foramen is an important area for examination, because it transmits the mental nerve. The violation of this site by an implant can result in permanent injury to the mental nerve and permanent paresthesia or anesthesia of the lower lip. In this research we used Cemax ToothPix2 software, which allows 2 mm thick 2D orthoradial multiplanar reformatted images to be reconstructed. The plane of the images is perpendicular (orthogonal) to the curvature of the dental arch. We were able to easily identify the mental foramen in cross-sectional images. Using the slice identi®cation numbers on the axial view we selected the two slices nearest the mental foramen (Figure 3). Subsequently, measurements were made from the superior border of the mental foramen to the alveolar crest, and from the inferior border of the mental foramen to the inferior mandibular border (Figure 4). Both observers found these points easy to localise. The low standard deviation (Table 1) indicates that the imaging technique is very accurate. Further, within approximately 20 min it was possible to generate images from the spiral CT, reformat them, and, after printing to perform measurements. In conclusion, spiral CT allows a high degree of accuracy when planning dental implants in proximity to the mental foramen, making it possible to formulate a more accurate diagnosis and treatment plan.
Acknowledgements Support for Dr Cavalcanti was provided from Foundation of Research of Sao Paulo State (FAPESP), 96/8851-2, Brazil. We thank Mrs Jane Jakobsen, Department of Preventive and Community Dentistry, for her assistance with the statistical analysis.
References 1. Shimura M, Babbush CA, Majima H, Yanagisawa SW, Sairenji E. Presurgical evaluation for dental implants using a reformatting program of computed tomography: maxilla/mandible shape pattern analysis (MSPA). Int J Oral Maxillofac Implants 1990; 5: 175 ± 181. 2. Abrahams JJ. Anatomy of the jaw revisited with a dental CT software program. AJNR 1993; 14: 979 ± 990. 3. DelBalso A, Hall RE. Advances in maxillofacial imaging. In: Current problems in Diagnostic Radiology 1993; 22: 92 ± 142. 4. Lam EW, Ruprecht A, Yang J. Comparison of two-dimensional orthoradially reformatted computed tomography and panoramic radiography for dental implant treatment planning. J Prosthet Dent 1995; 74: 42 ± 46. 5. James RA, Lozada JL, Truitt HP. Computer tomography (CT) application in implant dentistry. J Oral Implantol 1991; 17: 10 ± 15. 6. DelBalso AM, Greiner FG, Licata M. Role of diagnostic imaging in evaluation of dental implant patient. Radiographics 1991; 14: 699 ± 719.
7. Alder ME, Deahl ST, Matteson SR. Clinical usefulness of twodimensional reformatted and three-dimensionally rendered computerized tomographic images: literature review and a survey of surgeon's opinions. J Oral Maxillofac Surg 1995; 53: 375 ± 386. 8. Todd AD, Gher ME, Quintero G, Richardson AC. Interpretation of linear tomography and computed tomograms in the assessment of implant recipient sites. J Periondontol 1993; 64: 1243 ± 1249. 9. Yanagisawa K, Friedman C, Vinning E, Abrahams JJ. Denta Scan imaging of the mandible and maxilla. Head and Neck 1993; 15: 1 ± 7. 10. Weinberg LA. CT scan as a radiologic data base for optimum implant orientation. J Prosthet Dent 1993; 69: 381 ± 5. 11. Bessimo C, Lambrecht JT, Nidecker A. Dental implant planning with reformatted computed tomography. Dentomaxillofac Radiol 1995: 24: 264 ± 267.
Spiral CT MGP Cavalcanti et al
12. Luka B, Brechtelsbauer D, Gellrich NC, Konig M. 2D and 3DCT reconstructions of the facial skeleton: an unnecessary option or a diagnostic pearl? Int J Oral Maxillofac Surg 1995; 24: 76 ± 83. 13. Steenbeck JCM. Principles and applications of volumetric CT. Medicamundi 1993; 38: 20 ± 29. 14. Hildebolt CF, Vannier MW. Three-dimensional measurement accuracy of skull surface landmarks. Am J Phys Anthropol 1988; 76: 497 ± 503. 15. Hildebolt CF, Vannier MW, Knapp RH. Validation study of skull three-dimensional computerized tomography measurements. Am J Phys Anthropol 1990; 82: 283 ± 294.
16. Richtsmeier JT, Paik CH, Elfert PC, Cole TM 3rd, Dahlman HR. Precision, repeatability, and validation of the localization of cranial landmarks using computed tomography scans. Cleft Palate Craniofac J 1995; 32: 217 ± 227. 17. Cavalcanti MGP, Vannier MW. Three-dimensional spiral CT for craniofacial surgical planning and evaluation. In Proc in Biomedical Optics, Surgical-Assist Systems, of SPIE, 1998, 3262, pp. 26 ± 34.
333