1247
Virtual Reality and Haptics as a Training Device for Movement Rehabilitation After Stroke: A Single-Case Study Jurgen Broeren, MSc, OT, Martin Rydmark, PhD, MD, Katharina Stibrant Sunnerhagen, PhD, MD ABSTRACT. Broeren J, Rydmark M, Sunnerhagen KS. Virtual reality and haptics as a training device for movement rehabilitation after stroke: a single-case study. Arch Phys Med Rehabil 2004;85:1247-50. Objective: To investigate whether training in a virtual environment with a haptic device will improve motor function in the left hemiparetic arm of a stroke subject. Design: Single case, A-B-A design. Setting: University hospital research laboratory. Participant: A man in his late fifties (right handed), with a right-hemisphere lesion that caused a deficit in the left upper extremity. Intervention: The subject trained with a 3-dimensional computer game during a 4-week period that consisted of twelve 90-minute sessions. Main Outcome Measures: Three tests (Purdue pegboard test, dynamometer hand-grip strength, upper-extremity test) and a subjective interview were used to evaluate motor performance. Results: Improvements were found in fine manual dexterity, grip force, and motor control of the affected upper extremity. The subject reported that there was a change in his day-to-day use of the upper extremity and that he was able to use it in activities that were previously impossible for him. Conclusions: Training with virtual reality and haptics can promote motor rehabilitation. Key Words: Hemiparesis; Rehabilitation; Stroke; Virtual systems. © 2004 by the American Congress of Rehabilitation Medicine and the American Academy of Physical Medicine and Rehabilitation HE IMPAIRMENT OF the upper extremity is a prime obstacle in reacquiring competence in managing everyday T activities. Stroke survivors perceive the loss of upper-extremity function as a major problem.1 Broeks et al2 assessed the longterm motor and functional recovery of arm function after stroke and concluded, as many have before, that there is a need to develop active treatment methods for upper-extremity function. The recovery of the affected upper extremity is, like every other training situation, dependent on regularity and intensity
From Mednet (Broeren, Rydmark); and Department of Clinical Neuroscience and Rehabilitation Medicine (Broeren, Sunnerhagen), Sahlgrenska Academy, Go¨teborg University, Go¨teborg, Sweden. Presented in part at the 4th International Conference on Disability, Virtual Reality and Associated Technologies, September 18 –20, 2002, Veszpre´m, Hungary. Supported in part by the Swedish Stroke Victims Association, the Hjalmar Svensson Research Foundation, and the Federation of Swedish County Councils (VGregion). No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit upon the authors(s) or upon any organization with which the author(s) is/are associated. Reprint requests to Jurgen Broeren, MSc, OT, Dept of Clinical Neuroscience and Rehabilitation Medicine, Sahlgrenska Academy, Go¨teborgs University, Guldhedsgatan 19, SE 413 45 Go¨teborg, Sweden, e-mail:
[email protected]. 0003-9993/04/8508-8397$30.00/0 doi:10.1016/j.apmr.2003.09.020
in training, as well as on specificity.3 To stimulate recovery, a training program must allow the individual to develop and reestablish the motor system. Training programs should be made appealing, to motivate the patient. Target-oriented rehabilitation approaches and individually adapted training programs are essential for recovery. New models must be developed for patients and health professionals. Virtual reality technology is presently being explored as an assessment and training device for improving motor recovery after stroke. “Virtual reality” or virtual environment can be defined as a computer-generated environment, which imitates reality. Virtual reality generates a convincing interface, so that users believe they actually perceive sensory information that is similar to that of the real world. Virtual reality offers therapists new approaches for improving the effects of rehabilitation.4-7 Within a virtual environment, a patient can practice in a controlled environment— individuals can practice simple tasks or more complex tasks and they can measure their success in real time. Although the individual practices various tasks, it is possible for therapists to track movements for analysis.7 However, when an individual performs tasks with the affected upper extremity, sensory feedback is important for the capability to grasp. When manipulating objects in virtual environments, the user’s information must closely approximate information he/she would use in a natural setting. Consequently, the need for haptic force feedback becomes evident. The term “haptic” means interaction with a 3-dimensional environment created in a computer, which besides the visual impressions gives the user physical interaction, enabling him/her to touch the object in the virtual environment. Our report concerns a man whose affected upper extremity was trained with a haptic device in a virtual environment. METHODS Case Description The patient was a man in his late fifties who was right handed and who had a first-occurrence stroke. The time since the stroke was 12 weeks. The cause was an infarction, and the diagnosis was determined by a neurologist after clinical examination and was confirmed by computed tomography scan. The lesion was situated in the right genus of the internal capsule. On admission to the ward, the patient had symptoms in the form of contralateral hemiparesis; this persisted until the conclusion of the study and when training began. The patient was able to ambulate independently and could move his arm partially, with some wrist extension. He had no limitations in finger extension and flexion, but he had weak lateral grasp. His body awareness and spatial competence were normal. There were no limitations in understanding the information given. Most of his activities of daily living (ADLs) were accomplished by compensating with the right arm. Research Design A single-subject design was used to evaluate pre- and posttraining changes and changes at 20-week follow-up (35wk poststroke) posttraining.8 This included a baseline (A), an Arch Phys Med Rehabil Vol 85, August 2004
1248
VIRTUAL REALITY AND HAPTICS FOR STROKE REHABILITATION, Broeren
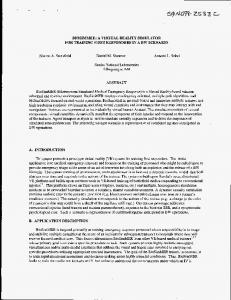
right-hand dominant, with a mean age of 50 years (range, 46 –73y), completed the same test as did the subject. In the fourth test, after the follow-up, the subject was interviewed about use of the affected upper extremity in ADLs at home. Apparatus Haptics were added to a computer workstation by using Reachin 3.0.c Reachin API is a programming environment that allows interactive manipulation of a 3-dimensional model by using a haptic interface. Haptic force feedback is provided by using the PHANToM haptic device. The patient connects to the mechanism by grasping the stylus, which provides a forcereflecting interface between a human user and a computer and creates a convincing illusion of interaction with solid physical objects. This sense of touch includes not only translational force feedback, but also rotational or torque feedback. Stereoscopic visualization is accomplished by using a standard Crystal Eyesd CE-2 setup (fig 1). Crystal Eyes allows the user to view 3-dimensional objects through a special display monitor mode and special stereo viewing glasses. The left and right images are alternated rapidly on the monitor screen and create the illusion that on-screen objects have depth and presence outside of the display. Fig 1. Virtual reality setup. The Reachin display, a stereoscopic display system with the PHANToM haptic device and Crystal Eyes CE-2 setup.
intervention phase (B), and a follow-up phase (A), with withdrawal of the direct intervention provided the occupational therapist. Procedure The patient was selected because he had an obvious deficit in his left arm that could be observed in ADLs. Three tests and a subjective interview were used to evaluate motor performance in the university hospital’s laboratory. The first test was the Purdue pegboard test, which measures unilateral and bilateral dexterity for 2 types of activity: gross movements of hands, fingers, and arms, and finger dexterity. Two subtests were used: (1) the ability to put as many pegs as possible with the left hand into holes on the left side of the board and (2) the ability, using both hands, to insert as many pegs as possible into the board. The score was the number of pins handled as quickly as possible in a 30-second period.9 In the second test, the dynamometer hand-grip strength by Grippita was recorded.10 Peak maximum grip force and the mean value of the 10-second sustained grip were measured. The third test was an upperextremity test, in which the subject moved the PHANToMb haptic device to different targets (generated positions) on the screen. The target placements (32) appeared randomly to the patient, but were actually set according to a preset cinematic scheme. The targets were numbered from 1 to 9, starting with number 1 at the lower right-hand side of the computer screen, continuing with 2 and 3 to the left. The fourth target was placed above target 1, 5 over 2, and so on. Motions of the upper extremity were divided in different directions—that is, sideways (left to right, right to left), up and down, diagonal (left to right), up and down. The x, y, and z coordinates for the haptic device and the targets were continuously sampled. Time, speed, trajectory distance (actual pathway of the upper extremity), and intertarget distance (geometric shortest distance between the targets) to complete the exercise were recorded to evaluate the performance. For purposes of comparison, a reference group was added to this test. Nine healthy men, all Arch Phys Med Rehabil Vol 85, August 2004
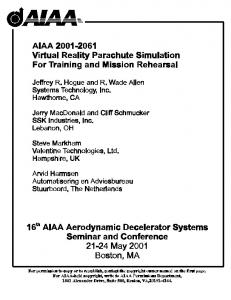
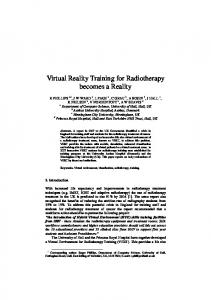
Training With his left upper extremity, the subject played a computer game, 3-dimensional bricks (fig 2), developed by Reachin Technologies. At the start of the game, the subject grasped the haptic device with his left hand. He then viewed a ball in a court filled with bricks. The game starts when the subject strikes the ball. The subject receives credit for the bricks knocked down. On the return, when the subject misses the ball, he collects minus points. The game was customized to operate at 4 speeds. Modifying the speed from 4 to 3 to 2 to 1 caused the program to increase the velocity of the ball. The level of difficulty was changed after the subject had reached a given score in 3 consecutive games. RESULTS Fine manual dexterity with the Purdue pegboard test improved on both subtests for the subject: for the left hand (impaired limb), it improved by 11% units after the intervention period and continued to improve from baseline to 17%
Fig 2. Screenshot of the computer game, 3-dimensional bricks.
VIRTUAL REALITY AND HAPTICS FOR STROKE REHABILITATION, Broeren
1249
Fig 3. Fine manual-dexterity values with the Purdue pegboard test for the left hand and both hands, measured as a percentage of a normal population.
units at follow-up. The results of the bilateral test improved with 22% and persisted during the follow-up (fig 3). The mean grip force at baseline was 13% of grip force in the normal ageand sex-matched population and increased to 57% at follow-up (table 1). The median intertarget time to complete the virtual reality test changed from 1.27 to 0.96 seconds posttraining and further decreased to .86 seconds during the follow-up. The reference group median intertarget time was .73 seconds, with some variation. Figure 4 shows the subject’s time results before and after training and at 20-week follow-up, compared with a reference group of 9 healthy men. The quotation of the trajectory distance (actual pathway of the upper extremity) and intertarget distance (geometric shortest distance between the targets), which reflects the degree of superfluous movements of the hand along the trajectory to the targets, did not indicate any major changes after the intervention period and during the follow-up. The values were close to the values of the reference group after the training period and during the follow-up. As a consequence, the velocity of movement was calculated and expressed basically as the inverse of the time results. The velocity to complete the assessment trial increased from pretraining values of .18m/s to normal values of .31m/s (reference group, .34m/s) after training, a result that persisted during the follow-up. In the follow-up assessment, the subject reported that a couple of weeks after the training he was able to use his left arm in several ADLs that were previously impossible for him (eg, buttoning his shirt, emptying the dishwasher with 2 hands). He felt that he could rely more on his left upper extremity. DISCUSSION Virtual reality technology was found to have potential as an assessment and training device in stroke rehabilitation. We observed that finger dexterity, grip force, and endurance increased after the treatment, which started 12 weeks after the stroke. Time to complete the exercise decreased considerably and approached normal values. The results imply that intensive training with virtual reality can reduce motor impairment and that it could optimize the stroke survivor’s motor skills. This is
Table 1: Grip Force Peak and Average Values During 10 Seconds (newtons) for the Left Hand
Peak Average 10s
Pretraining
Posttraining
Follow-Up (20wk)
Range
68 52
264 176
316 228
327–549 324–484
Fig 4. The time to perform the test is shown as a boxplot (25th, 75th percentiles) at 3 different time settings, as well as the result from the reference population (nⴝ9). Median value (thick black line) with 10th and 90th percentiles are shown at the end of the lines.
in line with the results of the Copenhagen Stroke Study, which showed that the function of upper-extremity recovery after a stroke with initial paresis occurred predominantly within the first 3 weeks and no further recovery of function should be expected after 11 weeks.11 We used a single-subject design. With a single-subject design, conclusions can be drawn about treatment effectiveness.8 Grip-force improvement increased considerably; this change could account for the improvement in endurance while playing the 3-dimensional computer game. By the end of the intervention period, the subject progressed to game level 1 (most difficult). The time it took the subject to complete the assessment trial decreased from the pretraining period to the posttraining period and approached normal values, a result that persisted during the follow-up (fig 4). The trajectory/intertarget distance quotient measure, indicating smoothness (precision, accuracy) of motion, did not change before or after training. These measures were already normal at the initial preassessment, compared with the reference group. The basis for training routines should be based on the patient’s specific neurologic demands as detected (ie, during the virtual reality haptic assessment), the neurologic status evaluation, and the results of the occupational therapy (OT) assessment. Our patient had an obvious deficit in his left arm, which we observed during ADLs, and poor performance in time to complete the virtual reality assessment, but he showed no lack of accuracy and precision. Before playing the 3-dimensional computer game, the level of difficulty was adjusted to his needs—that is, we modified the speed of the ball for each training session to maximize the effectiveness of the treatment. Maximizing the rehabilitative effectiveness of training programs as a means of reinforcing the patient’s motor performance requires both commitment and engagement in the process. The subject reported an increased awareness in using his affected left upper extremity; this is consistent with methods Arch Phys Med Rehabil Vol 85, August 2004
1250
VIRTUAL REALITY AND HAPTICS FOR STROKE REHABILITATION, Broeren
used in OT, which are intended to encourage the patient to use the impaired upper extremity in ADLs. After discharge from hospital units, many patients who have had a stroke still need qualified rehabilitation. Yet, the alternatives offered to patients after hospital discharge are limited in availability and vary locally and regionally. Home rehabilitation might be an important complement that can produce results comparable to institutional rehabilitation.12 The virtual reality setup presently used is easy to distribute but still expensive (⬇$20,000). We hope that a refined commercial alternative eventually will be affordable for health care providers. This could be installed, for example, in patients’ homes, and the Internet could be used for data transfer to the clinic, allowing the occupational therapist to monitor a patient’s progress remotely. In this way, one could reduce treatment costs in the long-term training process and improve patient quality of life. CONCLUSIONS The virtual environment’s potential to support tasks that address the specific needs of motor rehabilitation is promising. The use of meaningful and rewarding activities has been shown to improve a patient’s motivation to practice.13 Our results confirm the efficacy of the treatment and justify further clinical trials. A larger trial is required to determine the differences in improvement in motor ability of the upper extremities in stroke survivors using virtual reality with haptics. References 1. Feys HM, De Weerdt WJ, Selz BE, et al. Effect of a therapeutic intervention for the hemiplegic upper limb in the acute phase after stroke: a single-blind, randomized, controlled multicenter trial. Stroke 1998;29:785-92. 2. Broeks JG, Lankhorst GJ, Rumping K, Prevo AJ. The long-term outcome of arm function after stroke: results of a follow-up study. Disabil Rehabil 1999;21:357-64.
Arch Phys Med Rehabil Vol 85, August 2004
3. Kwakkel G, Wagenaar RC, Twisk JW, Lankhorst GJ, Koetsier JC. Intensity of leg and arm training after primary middle-cerebralartery stroke: a randomised trial. Lancet 1999;354:191-6. 4. Piron L, Cenni F, Tonin P, Dam M. Virtual reality as an assessment tool for arm motor deficits after brain lesions. Stud Health Technol Inform 2001;81:386-92. 5. Merians AS, Jack D, Boian R, et al. Virtual reality-augmented rehabilitation for patients following stroke. Phys Ther 2002;82: 898-915. 6. Broeren J, Bjorkdahl A, Pascher R, Rydmark M. Virtual reality and haptics as an assessment device in the postacute phase after stroke. Cyberpsychol Behav 2002;5:207-11. 7. Jack D, Boian R, Merians AS, et al. Virtual reality-enhanced stroke rehabilitation. IEEE Trans Neural Syst Rehabil Eng 2001; 9:308-18. 8. Zhan S, Ottenbacher KJ. Single subject research designs for disability research. Disabil Rehabil 2001;23:1-8. 9. Hamm N, Curtis D. Normative data for the Purdue Pegboard on a sample of adult candidates for vocational rehabilitation. Percept Mot Skills 1980;50:309-10. 10. Nordenskiold UM, Grimby G. Grip force in patients with rheumatoid arthritis and fibromyalgia and in healthy subjects. A study with the Grippit instrument. Scand J Rheumatol 1993;22:14-9. 11. Nakayama H, Jorgensen HS, Raaschou HO, Olsen TS. Recovery of upper extremity function in stroke patients: the Copenhagen Stroke Study. Arch Phys Med Rehabil 1994;75:394-8. 12. Early Supported Discharge Trialists. Services for reducing duration of hospital care for acute stroke patients. Cochrane Database Syst Rev 2002;(1):CD000443. 13. Nelson DL, Konosky K, Fleharty K, et al. The effects of an occupationally embedded exercise on bilaterally assisted supination in persons with hemiplegia. Am J Occup Ther 1996;50:639-46. Suppliers a. AB Detector, Box 17124, 402 61 Gothenburg, Sweden. b. SensAble Technologies Inc, 15 Constitution Way, Woburn, MA 01801. c. Reachin Technologies AB, Årstaa¨ ngsva¨ gen 24, 117 43 Stockholm, Sweden. d. StereoGraphics Corp, 2171 E Francisco Blvd, San Rafael, CA, 94901.